
Abstract
Background: Health care workers face elevated risk of obesity due to their unique work requirements. The purpose of this systematic review was to present a narrative summary of the characteristics and effectiveness of worksite wellness programs focusing on preventing obesity among health care workers. Method: The databases Medline, CINAHL, Embase, PsycINFO, and PubMed were searched. Experimental and quasi-experimental studies published in English (between 2000 and 2018) that (a) were worksite interventions, (b) had intervention directed toward health care employees, and (c) reported weight-related outcomes were included. We excluded commercial weight loss studies. Two coders extracted data on the following: purpose, key study characteristics, design, type and dosage of intervention, outcome measure(s), attrition rate, and risk of bias. Results: Of the 51 studies included in this review, the majority (75%, n = 38) targeted diet and physical activity behaviors. The majority reported improved weight outcomes in favor of the intervention. Overall, moderate- to high-intensity behavioral strategies, using any mode of intervention delivery (phone, face-to-face, or Internet), delivered by a trained professional were effective in improving weight-related outcomes. Environmental strategies were effective in improving healthier habits. Self-directed strategies worked better for motivated employees. Discussion: Multicomponent interventions offered in health care settings may be successful in improving employee weight. Across study designs, several gaps in the reporting of intervention design, dosage, fidelity, and system-level outcomes were found. Conclusion/Applying research to practice: Occupational health professionals should continue to be creative in developing multicomponent interventions (combining behavioral/educational, environmental, and organizational support) and use evidence guidance frameworks/tools to design an intervention and report dosage outcomes.
Background
Obesity is a major public health concern in the United States and worldwide (Ogden, Carroll, Kit, & Flegal, 2014). More than one third (35.0%) of American adults are obese (as defined by a body mass index [BMI] ≥30 kg/m2), and more than two thirds (69.0%) are either overweight or obese (BMI ≥25 kg/m2) (Ogden et al., 2014). Moreover, population growth estimates suggest that 42.0% of adults in the United States will be obese by 2030 (Finkelstein et al., 2012; Levi, Segal, St. Laurent, Lang, & Rayburn, 2012).
The physical and financial costs associated with obesity are numerous. For example, obesity is a risk factor for adverse health outcomes including coronary heart disease, stroke, high blood pressure, type 2 diabetes, cancer (endometrial, breast, and colorectal), liver and gall bladder disease, respiratory problems, reproductive complications, and mental health conditions (American College of Obstetricians and Gynecologists, 2013; Bonfrate, Wang, Garruti, & Portincasa, 2014; Campitelli, Rosella, & Kwong, 2014; De Pergola & Silvestris, 2013; Mozaffarian et al., 2016; Tison et al., 2015; Xu, Anderson, & Lurie-Beck, 2011).
The annual health care cost associated with obesity in the United States is estimated at US$190 billion (Cawley & Meyerhoefer, 2012). Work-related costs (absenteeism due to obesity-associated medical conditions, loss of productivity on the days at work) and insurance and disability costs are also higher among overweight and obese employees compared with their normal-weight counterparts (Cawley & Meyerhoefer, 2012; Lehnert, Sonntag, Konnopka, Riedel-Heller, & König, 2013; Merrill, Hyatt, Aldana, & Kinnersley, 2011).
Previous research suggests that employer-driven worksite wellness programs aimed to manage employee weight improved individual health and employer costs (Anderson et al., 2009; Katz et al., 2005). Recent meta-analyses on costs and savings associated with worksite wellness programs highlighted a savings of US$35 on monthly health care costs and US$2.73 related to absenteeism for every dollar spent (Baicker, Cutler, & Song, 2010; Dement, Epling, Joyner, & Cavanaugh, 2015).
Certain work settings such as health care are associated with higher prevalence of obesity due to work-related factors such as long work hours (>40 hours/week), shift work, and work-related stress (Luckhaupt, Cohen, Li, & Calvert, 2014; Sharma et al., 2016; Taylor & Bithoney, 2012). Compared with other U.S. workforces, hospital employees face higher cardiovascular risk factors have lower preventive health screening rates, lower participation in wellness programs, and higher emergency room (ER) and inpatient utilization rates (Sharma et al., 2016; Taylor & Bithoney, 2012). Moreover, health care employers are spending more on health care–related costs than employers from other industries (Taylor & Bithoney, 2012). Despite the increased risk of obesity that hospital employees face, we know little regarding intervention characteristics and their impact on obesity prevention among health care employees. To our knowledge, few reviews have thus far evaluated the effects of employee well-being interventions among health care professionals (Chan & Perry, 2012; Power, Kiezebrink, Allan, & Campbell, 2014; Williams et al., 2018). However, these reviews either excluded studies using quasi-experimental designs or did not focus on worksite obesity prevention strategies targeting all types of health care employees. Other published systematic reviews and meta-analyses on worksite obesity prevention did not focus on health care employees (Anderson et al., 2009; Katz, O’connell, Njike, Yeh, & Nawaz, 2008; Katz et al., 2005; Osilla et al., 2012; Watt, Verma, & Flynn, 1998).
To address this gap in knowledge, we conducted a systematic review of randomized controlled trials (RCTs), cluster randomized controlled trials (CRCTs), and quasi-experimental studies to describe the characteristics and effectiveness of worksite wellness interventions to prevent obesity in employees in health care settings (such as hospitals, clinics, and nursing homes).
Method
Data Sources
We searched experimental and quasi-experimental studies using Medical Subject Headings (MeSH) terms identified from those previously used in systematic reviews for worksite wellness studies (Anderson et al., 2009; Osilla et al., 2012). The following terms were identified and used in our search: workplace, worksite, occupational health services, occupational health, obesity, obese, physical activity, motor activity, weight loss, physical fitness, ex, cardiovascular diseases, cholesterol, hyperlipidemia, hypertension, nutrition, diet, body mass, index, primary prevention, risk reduction, behavior risk, management health promotion health, education health, behavior intervention, studies, and program evaluation. These search terms were combined as search sets, using Boolean operators (AND, OR, NOT). Search databases included Medline, CINAHL, Embase, PsycINFO, and PubMed. In addition, we used the reference lists of the searched articles and previous reviews to identify and include additional relevant articles. We excluded duplicate studies from the final search.
Inclusion Criteria
We included experimental and quasi-experimental studies published in English in peer-reviewed journals between the years 2000 and 2018 that were conducted in health care worksite settings (e.g., hospitals, clinics, health care provider office, health care centers, nursing homes, mental health settings). Studies were included if they targeted health care employees (age ≥18 years, of any weight or BMI [normal, overweight, obese] who work at least part-time) and examined weight-related outcomes (BMI, body weight, body fat, body mass, waist circumference, waist-to-hip ratio, skinfold thickness).
Exclusion Criteria
We excluded commercial weight loss efficacy studies (such as Weight Watchers, iDiet, Atkins diets) from the review. The process of inclusion, exclusion, and progress through the systematic review is described using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart (Moher, Liberati, Tetzlaff, & Altman, 2009) (Figure 1).
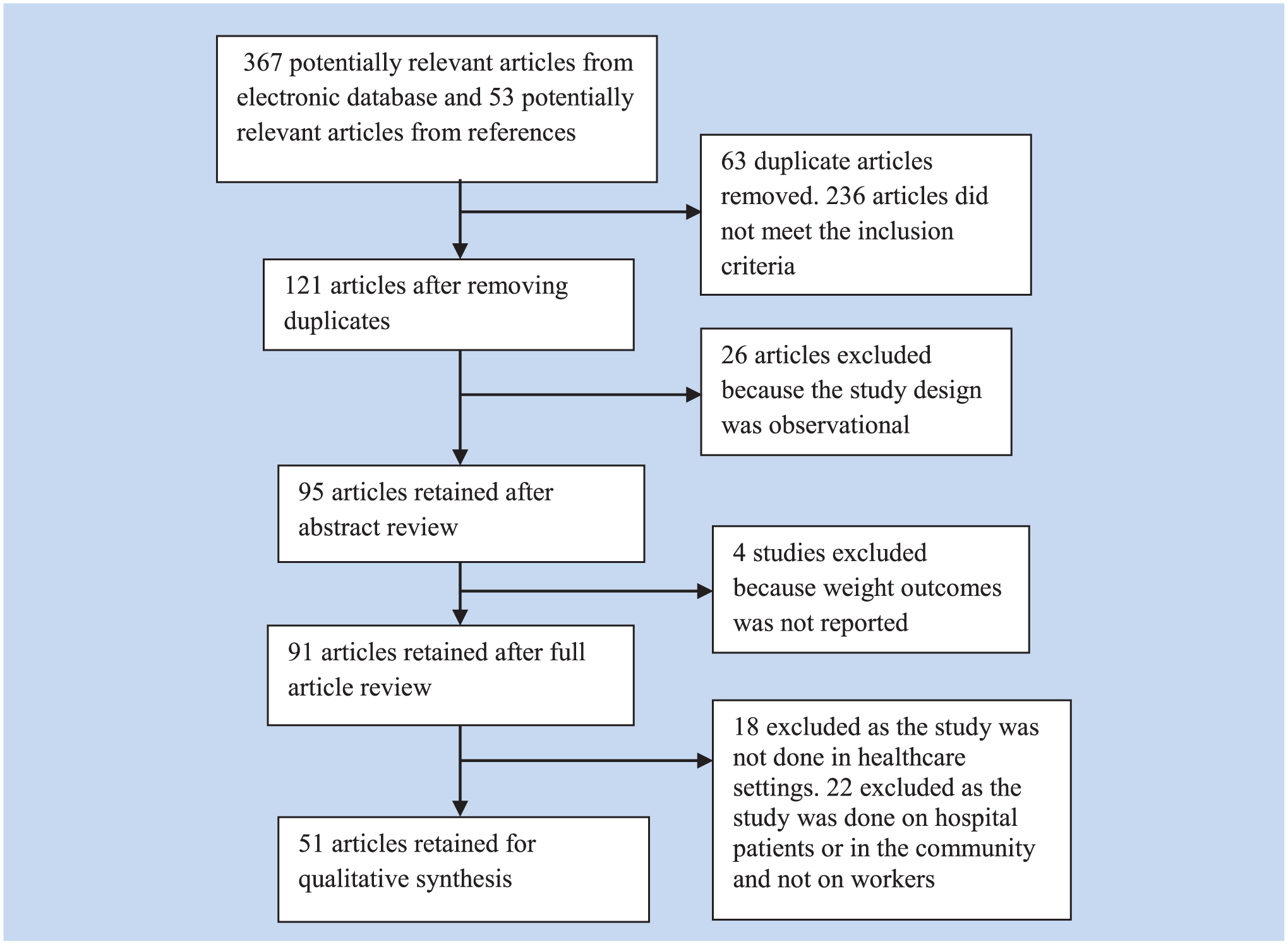
Flowchart depicting exclusion criteria and selection process.
Data Extraction
We assigned unique numbers to all included studies. Title and abstract review were followed by full text review. Key information was abstracted from the articles by two independent coders and categorized in an evidence table using the following codes: purpose, author, year of publication, sample size, research design, type and dosage of intervention, theoretical underpinnings, outcome measure(s), key findings, attrition rate, and risk of bias. Any discrepancy in the coding was resolved by consensus. In addition, a senior researcher with expertise in epidemiology and obesity prevention reviewed the methodology and coding results. Given the heterogeneity of outcome variables and interventions, meta-analysis was not possible.
We used Cochrane’s Risk of Bias matrix table (Higgins et al., 2011) to assess the methodological quality of RCTs and CRCTs. For quasi-experimental studies, a criterion published in previous systematic reviews was used to evaluate the quality of the studies (Benedict & Arterburn, 2008; Malik, Blake, & Suggs, 2014).
Results
A total of 51 studies were included in this review (Table 1 and Supplemental Table 1), with 30 (59%) studies that were conducted in the United States, 14 (27%) in Europe, and seven (14%) in other countries (Canada, Asia, Israel). Of the 51 studies included, 17 (33%) were RCTs and nine (18%) were CRCTs. The remaining 25 (49%) were quasi-experimental designs or nonrandomized trials, of which 10 were one-group pretest–posttest (without comparison group), 11 pretest–posttest (with comparison group), and four prospective study design.
Weight, Diet, and Physical Activity Outcomes for RCTs and CRCTs Included in the Systematic Review Examining the Effect of Worksite Wellness Interventions on Obesity Prevention in Health Care Workers
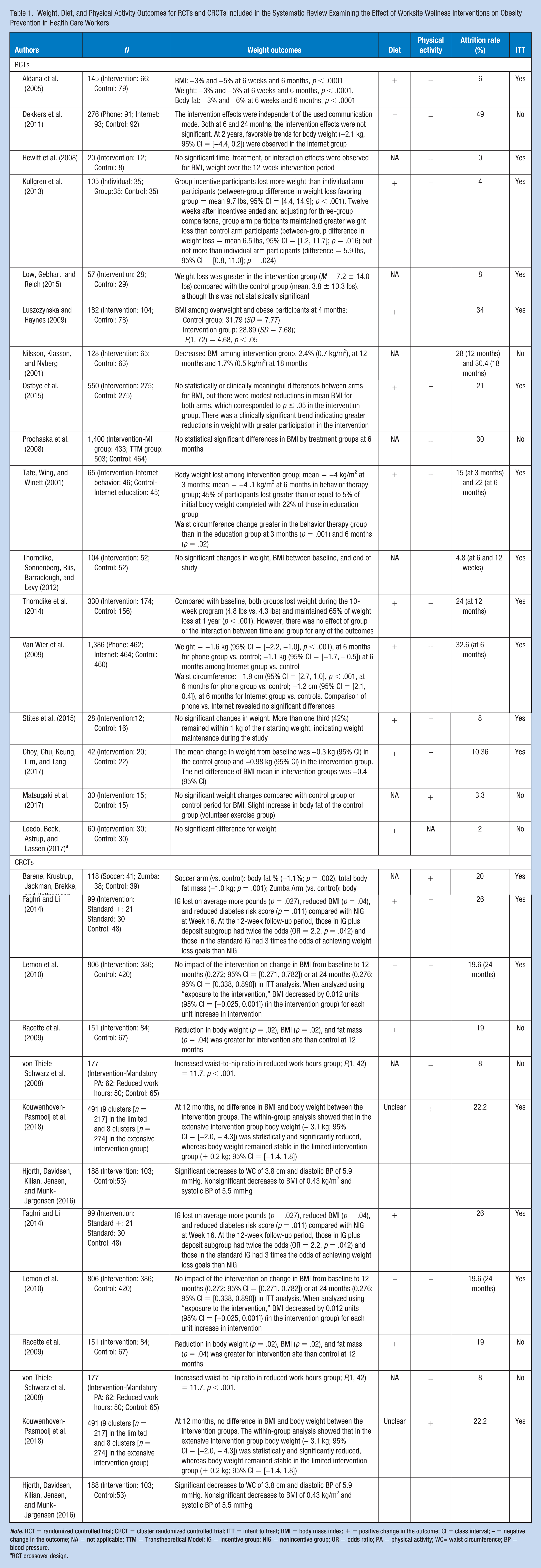
Note. RCT = randomized controlled trial; CRCT = cluster randomized controlled trial; ITT = intent to treat; BMI = body mass index; + = positive change in the outcome; CI = class interval; – = negative change in the outcome; NA = not applicable; TTM = Transtheoretical Model; IG = incentive group; NIG = nonincentive group; OR = odds ratio; PA = physical activity; WC= waist circumference; BP = blood pressure.
RCT crossover design.
RCTs
Of the 17 RCTs included in this review, 12 (70.5%) targeted diet and physical activity behaviors of their employees (Table 1 and Supplemental Table 1). Only two RCTs focused on physical activity behaviors, and three trials focused solely on dietary behaviors. The primary objectives of the RCTs included chronic disease prevention, physical fitness/activity, healthy eating, and improved weight outcomes (body weight, waist circumference, BMI, or fat reduction).
Follow-up from baseline ranged from 1 to 24 months, and only three studies reported long-term follow-up (>12months) for weight-related outcomes (Supplemental Table 1). The sample size ranged from 20 to 1,400 participants. The duration of the interventions ranged from 1 to 12 months. The majority of the studies recruited predominantly overweight or obese employees.
All but one RCT (Leedo, Beck, Astrup, & Lassen, 2017) used some form of structured educational or cognitive/behavioral component, delivered by trained professional online or face-to-face, rather than distributing only informational material to modify behaviors. Eight (47%) RCTs reported some theoretical basis for their intervention arm. Reported theories included Stages of Change Model (Low, Gebhart, & Reich, 2015), Cognitive-Behavioral Theory (Dekkers et al., 2011; Van Wier et al., 2009), Transtheoretical Model of Behavior Change (Prochaska et al., 2008), Choice Architecture (Choy, Chu, Keung, Lim, & Tang, 2017; Stites et al., 2015), and Social-Cognitive Theory (Choy et al., 2017; Luszczynska & Haynes, 2009; Ostbye et al., 2015). Similarly, eight (47%) RCTs reported organizational support strategies (such as offering the intervention within work hours and/or incentives) to promote participation. Only three (18%) RCTs (Low et al., 2015; Stites et al., 2015; Thorndike et al., 2014) used environmental strategies (such as access to on-site fitness center, discounted pricing, and nutrition information for food items offered at worksite) in addition to behavioral components, and one RCT (Leedo et al., 2017) used only environmental intervention (availability of healthy food items at worksite) to modify behavioral outcomes such as diet and physical activity.
With regard to weight-related outcomes, seven (41%) RCTs reported statistically significant positive associations of the intervention on outcomes, including lower BMI, lower weight, body fat, and/or waist circumference (Table 1). In addition to weight-related outcomes, studies reported changes in behavior outcomes (dietary improvement and/or increased physical activity).
With regard to the methodological quality of the sampled RCTs, 14 (82%) reported the specific randomization strategies used in the study. Furthermore, given the nature of behavioral interventions where the participants frequently know which intervention arm they are assigned to, none of the trials reported double-blinded status (of staff and participants), thus potentially introducing performance and ascertainment bias. Supplemental Table 2 reports further details on risk of bias for each of the included trials.
CRCT
Seven (78%) CRCTs targeted both dietary and physical activity behaviors, and the remaining two (22%) focused only on modifying physical activity. The primary objective of the CRCTs included cardiovascular risk reduction, increasing physical activity, obesity reduction, and/or diabetes prevention. The follow-up from baseline ranged from 3 to 24 months. Only one study reported long-term follow-up (>12 months) for weight-related outcomes, whereas all other studies had a follow-up time from 3 to 12 months. The length of the interventions ranged from 3 to 24 months. The sample sizes in these studies ranged from 98 to 806. Although all studies recruited predominantly overweight or obese female employees, one study (Kouwenhoven-Pasmooij et al., 2018) recruited predominantly overweight or obese male employees.
Seven (78%) CRCTs used some form of structured educational or cognitive/behavioral component, delivered by a trained professional (Table 1 and Supplemental Table 1). Similarly, six (67%) studies reported some theoretical basis, such as Cognitive-Behavioral Therapy (Christensen et al., 2011; Christensen, Overgaard, Carneiro, Holtermann, & Søgaard, 2012), Motivational Interviewing (Kouwenhoven-Pasmooij et al., 2018), Social Learning Theory (Hjorth, Davidsen, Kilian, Jensen, & Munk-Jørgensen, 2016), Transtheoretical Model of Behavior Change (Racette et al., 2009), and Ecological Model of Obesity Prevention (Lemon et al., 2010) for their intervention. Five (55%) of the CRCTs used organizational support strategies (such as reduced work hours to promote activity, offering commercially available weight loss programs and/or farmers market at worksite) in combination with other strategies to deliver the intervention. Only two (22%) CRCTs (Lemon et al., 2010; Racette et al., 2009) used environmental strategies (such as stairway signage, walking routes, and cafeteria signage) and/or offered incentives (such as cash and kitchen gadgets) to achieve the target outcomes.
For weight-related outcomes, all but two CRCTs reported one or more positive weight-related outcomes, including lower BMI, lower weight, waist circumference, waist-to-hip ratio, and reduced body fat /mass (Table 1). Two studies (Kouwenhoven-Pasmooij et al., 2018; Lemon et al., 2010) reported no statistical difference in weight outcomes between the intervention and control group, from baseline to intervention period. In addition to weight-related outcomes, two studies reported dietary improvement, and six reported increased physical activity.
Quasi-Experimental Studies
Twenty-five quasi-experimental studies were included in this review.
Of these, 11 (44%) studies used pretest–posttest design (with controls; Table 2 and Supplemental Table 3). The sample sizes ranged from 58 to 4,402 participants. Nine (82%) of the studies recruited predominantly female participants, and one (Moy, Sallam, & Wong, 2006) recruited only males. Although the majority of the studies focused their intervention on modifying both dietary and physical activity behaviors, two studies (Pohjonen & Ranta, 2001; Yuan et al., 2009) focused only on physical activity behaviors. Half (n = 6) of the studies reported some evidence/theoretical basis for the intervention, such as Theory of Planned Behavior (LaCaille et al., 2016), Transtheoretical Model (Long & Sheehan, 2010), Cognitive-Behavioral and Social Learning Theories (LaCaille et al., 2016; Tucker et al., 2011), Behavior-Change Health Practice (Yuan et al., 2009), Ecological Framework (LaCaille et al., 2016), and Experimental Learning and Bridges’ Model of Change (Shahar et al., 2009). The majority of the studies used a combination of behavioral/educational, environmental, and organizational support strategies to modify physical activity and/or dietary behaviors. Follow-up from baseline ranged from 2 to 60 months, with only three studies (Long & Sheehan, 2010; Moy et al., 2006; Pohjonen & Ranta, 2001) reporting long-term (>12 months) weight outcomes. With regard to weight-related outcomes (Table 2), eight (73%) of the studies reported significant change in the weight outcomes favoring the intervention group as compared with the control group, whereas three (LaCaille et al., 2016; Long & Sheehan, 2010; Moy et al., 2006) reported no change in weight-related outcomes.
Weight, Diet and Physical Activity Outcomes for Quasi-Experimental Studies Included in the Systematic Review Examining the Effect of Worksite Wellness Interventions on Obesity Prevention in Health Care Workers
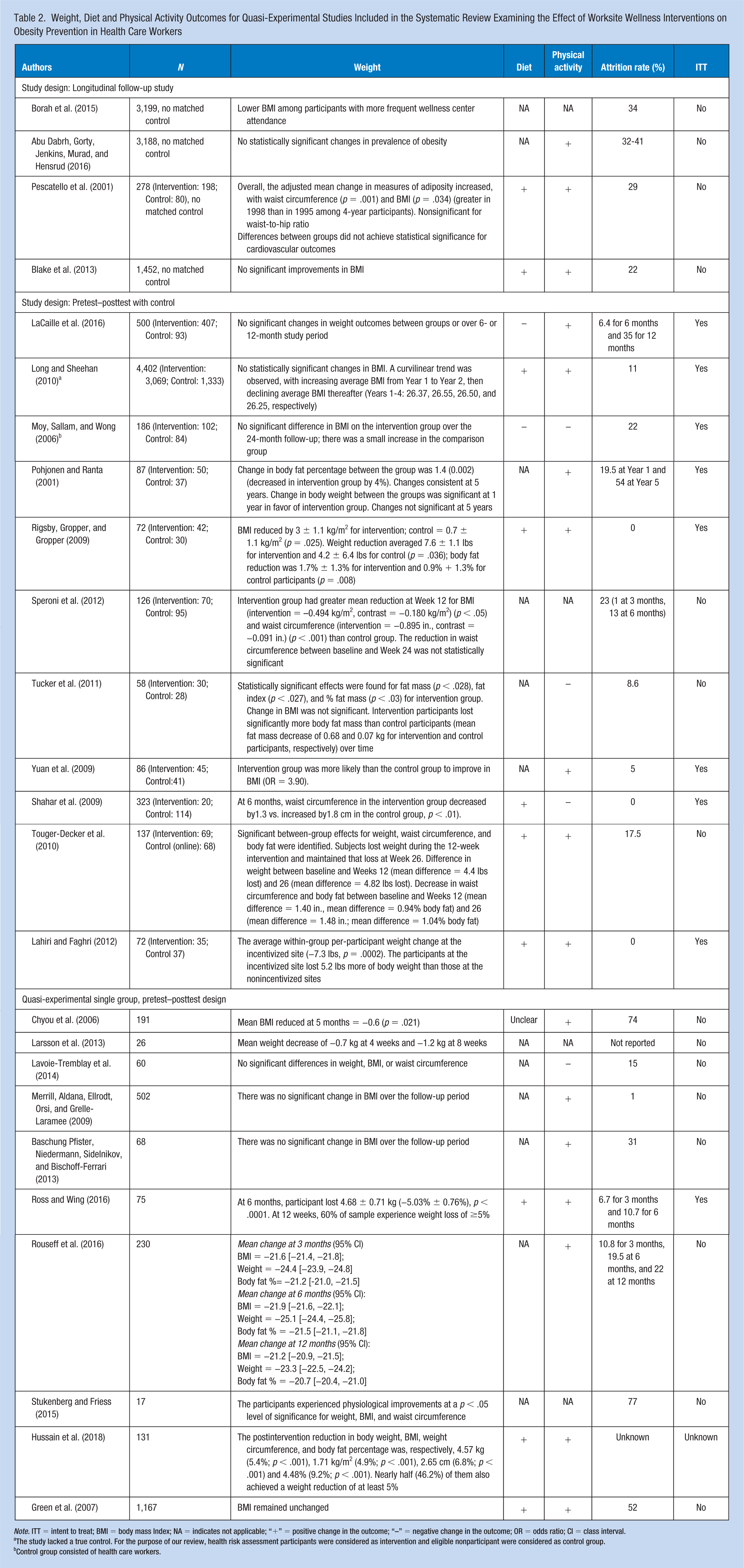
Note. ITT = intent to treat; BMI = body mass Index; NA = indicates not applicable; “+” = positive change in the outcome; “–” = negative change in the outcome; OR = odds ratio; CI = class interval.
The study lacked a true control. For the purpose of our review, health risk assessment participants were considered as intervention and eligible nonparticipant were considered as control group.
Control group consisted of health care workers.
Ten quasi-experimental studies with single-group, pretest–posttest design (without control) were included in this review (Table 2 and Supplemental Table 3). The sample size ranged from 17 to 1,167. Only four studies reported some evidence/theoretical basis (such as Health Belief Model, Merrill, Aldana, Ellrodt, Orsi, & Grelle-Laramee, 2009; Evidenced-Based, Ross & Wing, 2016; Transtheoretical Model, Baschung Pfister, Niedermann, Sidelnikov, & Bischoff-Ferrari, 2013; Empowerment Informatics Framework, Stukenberg & Friess, 2015) on which the intervention strategies were based. Four studies focused their intervention on only physical activity behaviors, and the remaining six studies focused on both physical activity and dietary behaviors of their employees (Table 1). Follow-up from baseline ranged from 1 to 24 months. All studies recruited predominantly female participants. All studies reported using behavioral/educational strategies to modify physical activity and/or dietary behaviors. With regard to weight-related outcomes, six (60%) studies reported significant reduction in the weight-related outcome, whereas four (40%) studies reported insignificant change in the weight outcome, after intervention.
Two of the four longitudinal time trend studies conducted serial surveys of employees and dependents of a large medical center with a fitness facility and reported results at 11-year through 14-year follow-up (Table 2 and Supplemental Table 3). In the first study (Borah et al., 2015), employees were grouped based on attendance or number of visits to the fitness center. The second study (Abu Dabrh, Gorty, Jenkins, Murad, & Hensrud, 2016) compared overall obesity prevalence estimates of the employees with national-level data at the follow-up. Results indicated that although BMI increased in both members and nonmembers of the fitness facility, a higher number of visits to the fitness center was associated with BMI improvements at long-term follow-up.
With regard to quality of the quasi-experimental studies, only seven (28%) analyzed and reported results using intent-to-treat (ITT) analysis. In addition, for studies with a control group, 78% studies reported significant dissimilarities between the intervention and control group at baseline in demographic or adiposity-related outcomes, thus compromising internal validity of the studies (Supplemental Table 4).
Discussion
Obesity prevention interventions are complex and multicomponent in nature. The purpose of this review was to examine experimental and quasi-experimental studies that presented results of worksite-based obesity prevention interventions targeting health care workers and reported intervention effect on at least one weight-related outcome.
Fifty-one publications were included in this review, with majority of the studies targeting both diet and physical activity behaviors. RCTs and CRCTs are gold standard, in the absence of which it is hard to attribute the outcome to the intervention. Across all study designs included in this review, a greater proportion of the CRCTs reported a positive impact of the intervention on at least one weight-related outcomes. Almost half of the RCTs also reported positive impact on at least one weight-related outcome, indicating a positive trend in the weight loss and behavioral outcomes (diet and physical activity).
Studies using only physical activity strategies reported mixed results, as has been documented in previous reviews (Anderson et al., 2009; Power et al., 2014; Verweij, Coffeng, van Mechelen, & Proper, 2011). Overall, our research indicates that interventions targeting both diet and physical activity behaviors have been successful in improving weight outcomes.
Intervention Approach
The majority of the studies used a variety of behavioral (including counseling by a trained professional, physical activity training sessions, cooking demonstration) and educational strategies (such as online or face-to-face lectures, educational material) to modify diet and physical activity behaviors. However, less than 50% of studies provided information on the theoretical underpinnings of the intervention, thus limiting our understanding of the proposed pathway of behavior change.
Although our review identified behavioral and educational strategies to be efficacious in improving weight outcomes, upon directly comparing behavioral with educational strategies as to which ones were more impactful, the results were inconclusive. Results from one feasibility and efficacy trial (N = 65 overweight employees) reported that behavioral strategies were better than educational strategies for short-term weight loss (Tate, Wing, & Winett, 2001). However, another trial (N = 550 obese employee) compared more intensive behavioral and less intensive educational strategies and reported lack of statistical significance between the impact of two strategies for BMI reduction, or dietary or physical activity–related outcomes at long-term follow-up (14 months) (Ostbye et al., 2015). We recommend further studies with larger sample sizes to be conducted in general health care employees to validate the comparative effectiveness of behavioral versus educational strategies for weight loss.
General ecological strategies (such as social marketing campaigns, annual counseling, nutritional labeling information, posters, signage to promote activity, access to wellness center) were not effective in improving weight outcomes or the perceptions about coworker support for healthy behaviors. However, interestingly, these strategies were effective in improving healthier habits (such as reduced smoking status, improved dietary intake, and physical activity) and employee’s perception of organizational commitment to their health (LaCaille et al., 2016; Lemon et al., 2010).
Organizational support strategies such as incentives appeared to be more effective when offered in a group setting (as opposed to individual) for weight loss and in improving diet and physical activity–related behaviors (Kullgren et al., 2013). However, certain subgroup employees such as night shift workers could potentially be isolated from organizational social network and culture and may not benefit from such strategies (Lemon et al., 2010). Individual strategies such as following a written diet plan worked better with participants who were self-motivated (Rigsby, Gropper, & Gropper, 2009). Given the heterogeneity of the health care workers, we recommend customizing the interventions to fit the needs of subgroups of employees.
Environmental strategies create opportunities to promote healthy eating and active living. In our review, one-fourth of the studies used some form of environmental strategies (such as standing work stations, on-site walking routes, access to an on-site wellness center, access to healthier meals) to manage employee weight. Only one study (Leedo et al., 2017) used only environmental strategies to improve weight outcomes and healthy eating behaviors, thus limiting our understanding of the impact of only environmental strategies on obesity prevention among health care employees.
Overall, multicomponent strategies integrating environmental components with intensive behavioral (weekly meeting with a dietitian, weekly or monthly counseling, trainer-led exercise, incentivized goal setting) and/or organizational support strategies (on-site weight watchers meetings, incentives, off-site exercise classes such as Zumba and soccer, reimbursements for gymnasium membership) were successful in improving weight-related outcomes in the health care employee population.
Mode of Delivery of the Intervention
Prior studies suggest that a personalized mode of intervention delivery (face-to-face or phone-based) is more effective than long distance mode (Internet, email, or web) for modifying behaviors related to weight loss (Harvey-Berino, Pintauro, & Gold, 2002; Norman et al., 2007; Wylie-Rosett et al., 2001). In our review, we found that use of any mode of delivery (face-to-face, phone, and Internet) fared better than the absence of the intervention (Aldana et al., 2005; Dekkers et al., 2011; Van Wier et al., 2009). Moreover, studies comparing the mode of delivery (phone vs. Internet) reported a lack of significant difference of the intervention effect on weight outcomes (Dekkers et al., 2011; Prochaska et al., 2008; Van Wier et al., 2009). Corroborating previous research (Harvey-Berino et al., 2010; Norman et al., 2007), these results indicate that using phone versus Internet appears to be similar in the outcomes produced.
Dosage of the Intervention
Overall, moderate-to-intense behavioral strategies (such as daily or weekly counseling/training session delivered by a trained professional) appeared to have fared better than less intensive strategies (such as only educational material, general ecological strategies, group or individual counseling 3-4 times a year, using activity monitor) in improving weight outcomes, indicating that intensity of the delivery matters (Aldana et al., 2005; Choy et al., 2017; Dekkers et al., 2011; LaCaille et al., 2016; Lemon et al., 2010; Moy et al., 2006; Pohjonen & Ranta, 2001; Tate et al., 2001; Thorndike et al., 2014; Thorndike, Sonnenberg, Riis, Barraclough, & Levy, 2012; Tucker et al., 2011; Van Wier et al., 2009; Yuan et al., 2009). However, one limitation is that information on dosage and fidelity of the intervention was not consistently reported across the studies, making it difficult to draw meaningful conclusion about dose–response relationship of various components of the interventions.
Methodological Limitations of Studies
Quality assessment of the RCTs and CRCTs revealed some common methodological issues. Intent to treat is the standard recommendation for assessing the efficacy of randomized trials. However, in this review, one quarter of the randomized trials and majority of the quasi-experimental studies did not use or provide information on the use of ITT analysis. Moreover, only 19% of randomized trials provided adequate data on blinding, and only 54% provided sufficient information on allocation concealment. This lack of information makes it challenging to assess how response and measurement bias was addressed in the studies, thus affecting internal validity of their findings.
In addition, many studies used varied, nonvalidated or self-reported measures to report weight outcomes, thus making direct comparison of those studies with the ones that measure weight outcomes challenging.
Majority of the RCTs targeted their interventions for high-risk employees (such as overweight or obese employees, women aged 40 and above, and those with diabetes), thus limiting the generalizability of the results to normal-weight employees from a primary prevention perspective. Participation of high-risk employees in worksite wellness interventions is not surprising given their intrinsic motivation to lose weight. In addition, many studies included in this review reported weight-related measures as group mean change. Further sensitivity analysis to assess how the participants who had the highest impact on weight outcomes were different from their counterparts who were unsuccessful at losing weight would be helpful for future research in this area. Most interventions were multicomponent in nature. However, information on the feasibility and applicability of the various components was limited, which can provide direction for future studies. Analysis of outcomes by specific subgroups including ethnicity and job profile was also limited and reported in less than a quarter of the studies. Job-related and ethnic differences in response to obesity interventions need to be assessed to offer customized solutions to subgroup of employees such as shift workers. Only 15% of the randomized trials and 32% of quasi-experimental studies reported long-term weight outcomes (12 months or more), thus limiting our understanding of weight loss maintenance. In addition, system-level measures (such as leadership engagement, senior-level management support, organizational readiness), critical in promoting employee participation and successful implementation, were not reported across the study designs.
Health care worksites are well suited for obesity prevention, as an intervention carried out in a hospital or clinic setting has an advantage of being able to target a large and diverse population of employees directly, and that of patients, and their caretakers, indirectly. Many of the interventions included in this review were either conducted off-site (Aldana et al., 2005; Barene, Krustrup, Jackman, Brekke, & Holtermann, 2014; Nilsson, Klasson, & Nyberg, 2001; Pohjonen & Ranta, 2001) or were offered as long-distance counseling/coaching programs (Dekkers et al., 2011; Long & Sheehan, 2010; Prochaska et al., 2008; Ross & Wing, 2016; Van Wier et al., 2009), thus limiting the availability of the intervention for hard-to-reach employees (such as night shift workers) and the larger population of patients and caretakers.
The strengths of this review lie in the inclusion of recent randomized and nonrandomized studies describing worksite wellness in health care employees and extending the knowledge pool from previous systematic reviews (Chan & Perry, 2012; Power et al., 2014). To overcome organizational constraints and ease implementation, sometimes, the intended study design is modified and may lose methodological and scientific rigor compared with RCTs and CRCTs. We feel that including quasi-experimental designs in our review may offer creative solutions for managing employees’ weight in large health care settings, where interventions focusing on complex behavioral changes such as diet and physical activity may face implementation barriers. For appropriate comparability, we presented results segregated by type of design.
Our review has some limitations. We reviewed English publications that reported at least one weight-related outcome, thus omitting relevant studies where these outcomes were either not reported due to statistical reasons or because they were not the primary outcomes. This review also excluded studies that reported only dietary and/or physical activity–related behavioral outcomes. Although the studies included in this review have provided useful direction for weight loss among health care employees, we found several gaps in the reporting of intervention design, dosage, fidelity, and system-level outcomes.
Implications for Occupational Health Practice
This systematic review offers valuable information to organizational support makers, public health researchers, and wellness practitioners on the impact of worksite-based obesity prevention interventions among health care employees, including the impact of various strategies used. Occupational health nurses should continue to be creative in developing multicomponent interventions (combining behavioral/educational, environmental, and organizational support) and use evidence guidance frameworks/tools for obesity prevention to design an intervention. There are several online resources, such as Prevention Group of the International Obesity Task Force (IOTF) framework (Swinburn, Gill, & Kumanyika, 2005), Analysis Grid for Environments Linked to Obesity (ANGELO) framework (Swinburn, Egger, & Raza, 1999), understanding evidence (Puddy and Wilkins, 2011), and solution-oriented research paradigm (Campbell et al., 2000; Robinson & Sirard, 2005), available that can be used for future reference. It is also recommended that future studies and systematic reviews use quality assessment tools (such as Grading of Recommendations Assessment, Development, and Evaluation [GRADE] guidelines, Balshem et al., 2011; EQUATOR network, Simera et al., 2010; quality assessment tool for quantitative studies for effective public health practice, Thomas, 2003; Cochrane definitions and criteria for RCTs, controlled clinical trials (CCTs), and quasi-experimental studies, Higgins et al., 2011; Ryan, Hill, Broclain, Horey, Oliver, & Prictor, 2013) to report the characteristics, dosage, fidelity, and outcomes of the studies so that studies can be compared and summarized quantitatively as well as qualitatively.
Supplemental Material
Supplemental_Tables_2019 – Supplemental material for Obesity Prevention Worksite Wellness Interventions for Health Care Workers: A Narrative Review
Supplemental material, Supplemental_Tables_2019 for Obesity Prevention Worksite Wellness Interventions for Health Care Workers: A Narrative Review by Mudita Upadhyaya, Shreela Sharma, Lisa A. Pompeii, Monica Sianez and Robert O. Morgan in Workplace Health & Safety
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Mudita Upadhyaya, DrPH, MPH, MHA, is the senior program wellness manager at University of Texas, Health Science Center, Houston, Texas. She has an interest in optimizing the health of health care workers at risk of obesity and cardiovascular diseases.
Shreela Sharma, PhD, RD, LD, is an associate professor at University of Texas School of Public Health, Houston, Texas. Her research interests focus on behavioral epidemiology primarily focusing on obesity prevention in children, adolescents, and their families and health disparities research in low-income minority populations.
Lisa A. Pompeii, PhD, RN, FAAOHN, is a senior faculty and codirector (Center for Epidemiology & Population Health, Department of Pediatrics) at Baylor College of Medicine, Houston, Texas. Her research focuses on occupational and injury epidemiology, including effects of maternal occupational exposures and adverse pregnancy outcomes. In addition, she studies occupational health issues specific to health care workers and the effects on quality of patient care.
Monica Sianez, DrPH, MPH, is an adjunct assistant professor of Clinical Research and Leadership at George Washington University. In her scholarship, she uses both quantitative and qualitative research methods to examine health inequities among Latino populations in the United States using a socioecological approach.
Robert O. Morgan, PhD, is professor and department chair of Management, Policy, & Community Health at University of Texas School of Public Health, Houston, Texas. His research interests include health services research, access to care, veterans’ health, and Medicaid and Medicare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.