
Abstract
This article applies a hazard-based approach to the identification of physical, mental, and psychosocial health needs of post-9/11 veterans. The weaponry, survival, and population of servicemen and women by the military have evolved over time, particularly during the post-9/11 era. It is evident that military hazards and potential exposures vary depending on not only the deployment era but also the specific location and role. Many individual factors may affect the development of health problems. Recent evidence-based literature about post-9/11 veterans’ long-term complex health issues is summarized, so occupational health nurses can advocate for the provision of veteran-sensitive care.
Keywords
Many post-9/11 veterans do not seek care from Veterans Health Administration (VHA) providers, so it is of the utmost importance that not only VHA providers, but also non-VHA providers, understand the health needs of veterans (National Center for Veterans Analysis and Statistics [NCVAS], 2015a). As is true in any workplace, occupational and environmental hazards must be considered when providing care to veterans. The identification of occupational hazards is complex and relates to specific exposures veterans may have experienced as well as many other personal, environmental, and occupational factors.
Method
A literature review was conducted using the following research question:
The Ovid, MEDLINE, PsycINFO, and Cochrane databases were searched using the keyword “veteran*.” The PubMed database was also searched using keywords “veteran*” in the article title and “health.” To limit the results and focus on more widely published and repeatedly studied topics, results were filtered for systematic reviews and meta-analyses focused on humans and published in English during the five previous years. Only articles pertaining to post-9/11 veterans were included; articles focused on the needs of veterans’ families or treatment modalities were excluded. Additional data and primary research articles were found on the Wounded Warrior Project website, U.S. Department of Veterans Affairs (VA) websites, and in the references of systematic reviews and meta-analyses.
Who Are Veterans?
According to the U.S. Census Bureau, veterans are men and women who have served, but are not currently serving, on active duty in the U.S. Army, Navy, Air Force, Marine Corps, or Coast Guard, or who served as a U.S. Merchant Marine during World War II (Veterans, 2013). Members of the Reserve (any military branch) and National Guard (Army and Air Force) are not considered full-time but may be deployed at any time; they train one weekend each month and 2 weeks each year (Veterans Employment Toolkit Handout, 2012). Individuals who served in the National Guard or Reserves are classified as veterans only if they were ever called to active duty. Active duty means working full-time for the military either at a base or via deployment (Veterans Employment Toolkit Handout, 2012). Therefore, a veteran is not necessarily someone who was deployed overseas. Although a veteran could be as young as 17 years of age, a veteran is defined as being 18 years or older (Veterans, 2013). Notwithstanding these definitions, veterans may deny their veteran status as this definition depends on veterans’ own perspectives of the veteran definition.
Several post-9/11 military operations have been initiated with differing nomenclature depending on the time frame and location. As described in Table 1, these wars (e.g., Operation Enduring Freedom [OEF], Operation Iraqi Freedom [OIF], Operation New Dawn [OND], Operation Inherent Resolve [OIR], and Operation Freedom’s Sentinel [OFS]) were primarily served in Iraq and Afghanistan. Most studies of post-9/11 veterans have focused on OEF and OIF veterans. Approximately 2.4 million U.S. Armed Forces have served in Iraq and Afghanistan since September 9, 2011, and this growing veteran population was projected to increase by 51% between 2013 and 2018 (NCVAS, 2015a).
Post-9/11 Military Operations (Fischer, 2015)
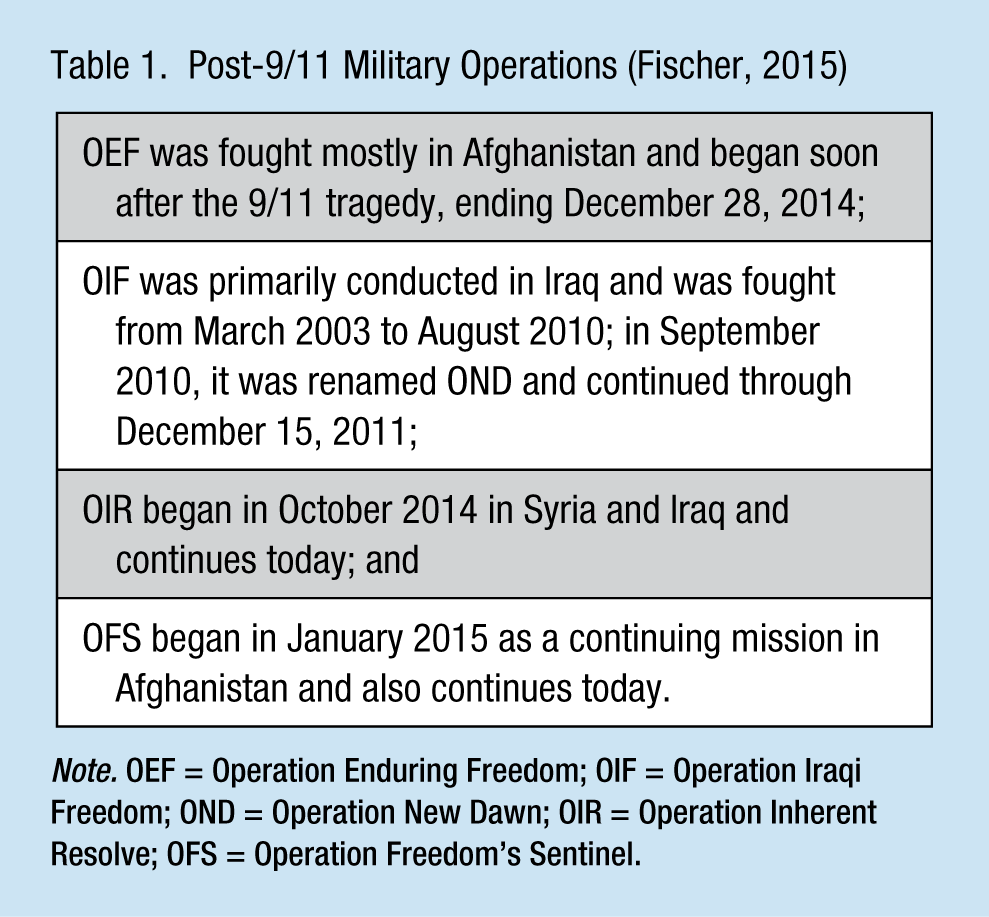
Note. OEF = Operation Enduring Freedom; OIF = Operation Iraqi Freedom; OND = Operation New Dawn; OIR = Operation Inherent Resolve; OFS = Operation Freedom’s Sentinel.
The Unique Post-9/11 Veteran Population
The post-9/11 military is more diverse (i.e., more women and minorities) compared with other military service eras. More than 30% of post-9/11 veterans are women, and this percentage has more than doubled since the Vietnam service era (NCVAS, 2015b). The male post-9/11 population is more diverse than other service eras with almost double the number of non-White veterans (20%) and more than double the Hispanic veterans (11.5%). The female post-9/11 population is even more diverse with 32% non-White and 13% Hispanic veterans (NCVAS, 2015a). About 75% of post-9/11 veterans are below age 44 with a median age of 33; veterans from other service eras are mostly above age 55 (NCVAS, 2015a). In 2013, the post-9/11 veteran is more likely to be non-White, single, younger, uninsured, and have no income compared with veterans from other service eras (NCVAS, 2015a). In 2013, only 17.8% of post-9/11 veterans were enrolled and used VHA care; this is less than any other veteran-era groups (NCVAS, 2015a).
The post-9/11 service era has resulted in fewer deaths from battle wounds compared with previous military service eras. More soldiers survive horrific brain injuries and amputations. As of June 2015, 6,855 military and civilian casualties have died during the post-9/11 wars; the post-9/11 survival rate from wounds is about 87%, which is 18% higher than the survival rates of the Vietnam and Gulf wars (“America’s Wars,” n.d.; Fischer, 2015).
Improved survival is a result of better protective gear (e.g., body armor and helmets) as well as better health care delivery on the battlefield (Gawande, 2004; Okie, 2005; Wallace, 2009). Better medics and corpsmen training and more advanced and timely response to the wounded are additional factors (Gajewski & Granville, 2006). For veterans with limb loss, early tourniquet application, early use of broad-spectrum antibiotics, more frequent use of hemostatic dressings for tissue preservation, and more efficient evacuation of unstable soldiers have all contributed to survival. The average evacuation in Vietnam took 45 days; in Iraq and Afghanistan, an evacuation can be completed within 96 hours (Gajewski & Granville, 2006).
Because more soldiers are surviving, they are also being redeployed. A study of more than 289,000 post-9/11 veterans showed 33% were redeployed at least once (Seal et al., 2009). Compared with previous war eras, the current military is smaller and serving as a voluntary force with multiple and longer deployments (Seal et al., 2009). Because of this increased exposure to trauma, post-9/11 veterans may have multiple, more complex health-related needs.
Post-9/11 Military Hazards
Potential hazard exposures depend on the specific job performed during military service. For example, exposure to fuels (e.g., diesel or JP-8) from military vehicles may have long-term respiratory effects, or exposure to chemical agent resistant coating (CARC) may affect the skin, respiratory system, eyes, or kidneys (“Occupational Hazards,” 2015). Having conversations with veterans to understand their specific work role can identify hazards to which they were potentially exposed during military service. Notwithstanding the “healthy soldier effect” (i.e., soldiers tend to be healthier and more physically fit than the average civilian), veterans may be at higher risk for particular health conditions because of the hazards to which they were exposed during military service (Kang et al., 2015).
A plethora of hazards specific to the post-9/11 service era have been identified. These include, but are not limited to, air pollution, combat smoke, burn pits, landmines, improvised explosive devices (IEDs), gunshots, rocket-propelled grenades, mortar and rocket fire, depleted uranium, and aircraft and artillery noise (Falvo, Osinubi, Sotolongo, & Helmer, 2015; Franklin et al., 2015; Gajewski & Granville, 2006; Kelly, Boyd, Valente, & Czekanski, 2014). Soldiers may have also carried heavy equipment: armor and weapons weighing more than 100 pounds (Alford, Seal, Sachs, Lin, & Hardesty, 2014). The annual Wounded Warrior Project survey included 23,200 post-9/11 veterans with a service-related physical injury or mental illness; the survey data revealed many potentially traumatic military experiences, such as the following:
78% of veterans had a friend who was seriously wounded or killed during the war;
73% of deployed veterans saw dead or seriously injured noncombatants;
63% smelled decomposing bodies; and
18% were responsible for the death of a civilian (Franklin et al., 2015).
Other military hazards may apply to any veteran regardless of service era, such as vaccine inoculations, insect bites, insect repellent, temperature extremes, contaminated food or water, physical trauma, mental trauma, and sexual trauma.
Burn Pits
Burn pits were used in Iraq and Afghanistan to eliminate waste at military sites; the waste included chemicals, paint, metal, plastic, rubber, and wood as well as medical and human waste. Research by the Department of Defense (DOD) has not shown any long-term health problems from burn pit exposures, although an Institute of Medicine (IOM; 2011) report on the long-term health consequences of burn pit exposures in Iraq and Afghanistan shows a possible association between exposure to combustion products and reduced lung function.
Depleted Uranium
Depleted uranium, a by-product of the uranium enrichment process for nuclear production, occurs naturally and has radioactive and chemical properties; it was first used as a projectile in the 1991 Gulf War because it can penetrate armor from greater distances (Squibb et al., 2012). Significant exposures to depleted uranium may have occurred during the Gulf War, and in Iraq, Afghanistan, and Bosnia. When these projectiles strike, they break into smaller particles and fine aerosols; soldiers may be exposed by way of inhalation, ingestion, or wound contamination (Squibb et al., 2012). Therefore, if soldiers are near buildings or vehicles when (or soon after) they are struck by friendly fire, exposure to depleted uranium is possible.
The VA initiated a monitoring program for veterans who may have been exposed to depleted uranium in 1993 and also opened the Toxic Embedded Fragment Surveillance Center in 2008 to observe Iraq and Afghanistan veterans with retained fragments from IEDs (“Depleted Uranium Fact Sheet,” 2014; Squibb et al., 2012). Veterans need not be eligible for VHA benefits to participate in this program (“Depleted Uranium Fact Sheet,” 2014). Biomonitoring and other surveillance of these participants have not identified clinically significant long-term health effects to date (Squibb et al., 2012).
To clarify, veterans are concerned about not only the exposures they may have had during service but also which exposures should be of concern. A study of 486 Iraq and Afghanistan veterans representing all military branches who were clinically evaluated at the War-Related Illness and Injury Study Center in New Jersey between 2006 and 2010 revealed that almost all veterans had a postdeployment health concern and on average were concerned about eight or more exposures (Osinubi et al., 2012). The following exposures were of concern by 90% or more of participants: air pollution, burn pits, contaminated food and water, depleted uranium, biological warfare, and chemical weapons; interestingly, the hazards to which veterans were exposed were not necessarily the same hazards for which they were most concerned (Osinubi et al., 2012).
Most Common Health Problems Treated and Reported
More than half of post-9/11 veterans who reported receiving care from VHA providers since 2002 (based on International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] coding) were treated for musculoskeletal or connective tissue diseases, an ill-defined condition or symptom or sign, or a mental disorder; more than one third were treated for an endocrine or nutritional or metabolic disease or a digestive disease (Epidemiology Program, Post-Deployment Health Group, 2015). The Wounded Warrior Project survey, which included post-9/11 veterans and service members who had incurred a service-related injury, illness, or wound, showed the most common self-reported health problems included posttraumatic stress disorder (PTSD); sleep disorders; back, neck or shoulder problems; or depression (Franklin et al., 2015). Of the identified post-9/11 military operations, OEF veterans experienced the most wounds with more than 200,000 as of July 2015 (Fischer, 2015). The following section will highlight health conditions which may be of concern to post-9/11 veterans.
Physical Trauma—Limb Loss
Inherent in the role of a combat soldier, physical trauma (e.g., burns, blunt force trauma, traumatic brain injury [TBI], multiple injuries, or limb loss) may occur. Through June 2015, 1,645 post-9/11 era soldiers incurred a major limb amputation (Fischer, 2015). Veterans with one or more lost limbs have a number of complex needs: psychosocial issues, phantom pain, itching, wound and stump care, adjustment to the prosthesis, and motor relearning (Boudiab & Kolcaba, 2015). These veterans may no longer be able to perform typical personal and work activities and experience new identity, adaptions, social integration, and functioning post deployment (Messinger, 2009). The last phase of rehabilitation for an amputee can include advanced training for motor and vocational skills to regain the ability to be active and optimize functioning (Gajewski & Granville, 2006). Limb loss may have occurred on the soldier’s dominant side making recovery even more challenging. Remarkably, some veterans who have sustained limb loss choose to return to combat (Gajewski & Granville, 2006).
Behavioral Health Conditions
All deployed veterans experience lack of privacy, being away from family and friends with little regular contact, isolation and boredom, and combat conditions (Lange, 2009). The intense stress soldiers experience can lead to a number of mental illnesses, including depression, anxiety, PTSD, or sleep disorders (Babson, Del Re, Bonn-Miller, & Woodward, 2013; Tanielian & Jaycox, 2008). Previously deployed veterans are 3 times more likely than soldiers without previous deployments to screen positive for PTSD (Adjusted Odds Ratio [AOR] = 3.69, 95% confidence interval [CI] = [2.59, 05.24]) or depression (AOR = 3.07, 95% CI = [1.81, 5.19]; Kline et al., 2010).
Potential influences on veterans’ mental health include factors related to deployment. Research by G. H. Cohen, Fink, Sampson, and Galea (2015) has captured the nature of the development of behavioral health disorders post deployment. In addition to factors that relate to deployment (e.g., comorbid psychopathology, combat exposure, deployment [location, length, and frequency], family and personal concerns and fears, and unit cohesion and support), providers must also consider factors that influence mental health before (e.g., personality, preparedness, prior psychopathology, prior psychiatric treatment, smoking status, and social support) and after (e.g., attitudes regarding outcome of conflict, comorbid psychopathology, readjustment stress, and social support) deployment. Clearly, the development of behavioral health disorders for veterans is complex and related to unpredictable factors.
PTSD
According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013a, 2013b), PTSD is classified as a trauma- and stress-related disorder, featuring symptoms from four clusters:
Reexperiencing symptoms (e.g., spontaneous memories, recurrent dreams),
Avoidance symptoms (distressful thoughts or feelings),
Negative alternations in cognition and mood, and
Alterations in arousal and reactivity (flight or fight reactions, aggression, sleep disturbances).
For a PTSD diagnosis, an exposure to a traumatic event is required; these symptoms must persist for at least 1 month causing distress and functional impairment, and no substance or comorbid condition can be the cause of this symptomatology (APA, 2013; Yehuda, Lehrner, & Rosenbaum, 2015). A meta-analysis including 33 studies and nearly 5 million OEF and OIF veterans from 2007 to 2013 showed an overall PTSD prevalence of 23%, nearly one of every four veterans (Fulton et al., 2015).
In addition to the traumatic event experience, a number of other risk factors should be considered in the development of PTSD. The risk for PTSD is 2.5 times higher in the presence of another mental health diagnosis (95% CI = [2.01, 3.16]) and 1.16 times higher after suffering physical injuries (95% CI = [1.01, 1.34]; Sandweiss et al., 2011). Other PTSD risk factors include type and severity of trauma, female gender, age (younger), enlisted rank, no relationships, less education, race, predeployment mental health, history of trauma, and postdeployment social support stressors (Peterson, Luethcke, Borah, Borah, & Young-McCaughan, 2011; Wall, 2012). Former prisoners of war (POW) and veterans with extended or multiple deployments are also at increased risk for developing PTSD (Seal et al., 2009; Wall, 2012).
Clinicians should screen for PTSD-related dysphoria symptoms, a notably strong predictor of health-related quality of life (Tsai, Whealin, Scott, Harpaz-Rotem, & Pietrzak, 2012). Studies showed dysphoria and numbing of response and affect (i.e., part of the avoidance symptoms) are positively associated with impaired interpersonal relationships and an indicator of how long the PTSD will persist (Hassija, Jakupcak, & Gray, 2012). Symptoms of dysphoria should be monitored to improve the quality of not only mood but also relationships (Hassija et al., 2012).
Various screening tools are available to identify veterans with PTSD; these tools can be used in conjunction with a clinical diagnostic evaluation. The Posttraumatic Stress–Related Functioning Inventory (PRFI) is a 27-item questionnaire of self-reported symptoms. The tool has adequate internal consistency and test–retest reliability with post-9/11 veterans and can assess their functioning (McCaslin et al., 2016). Another tool tested with veterans is a seven-factor model of the DSM-5; the tool has adequate specificity with comorbidities, suicidal ideation, functioning, and quality of life (Pietrzak et al., 2015).
Providers must take into consideration veterans who score just below the threshold for a PTSD diagnosis. A study of 275 Iraq and Afghanistan veterans showed subthreshold PTSD associated with hopelessness and suicidal ideation compared with veterans with PTSD, yet those with subthreshold PTSD were less likely to seek mental health treatment (Jakupcak et al., 2011). This group should be referred for mental health treatment before mental health issues escalate.
Veterans with PTSD may be at increased risk for other conditions or problems. A study that included a sample of 638,451 veterans (not all from the post-911 era) diagnosed with PTSD in 2012 had a 21.9% prevalence of a comorbid substance use disorder; These veterans were more likely to be homeless than veterans with PTSD and no comorbid substance use disorder (Bowe & Rosenheck, 2015). A study of more than 2 million obese veterans (not specific to the post-9/11 era) demonstrated significant associations between obstructive sleep apnea and PTSD as well as major depressive disorders (Babson et al., 2013). Other comorbidities common to veterans with PTSD include metabolic syndrome, dementia, obstructive sleep apnea, sexual dysfunction, and suicidal ideation. These conditions are highlighted along with their corresponding odds ratios (ORs) and study descriptions in Table 2.
PTSD and Risk for Comorbidities and Other Health Problems
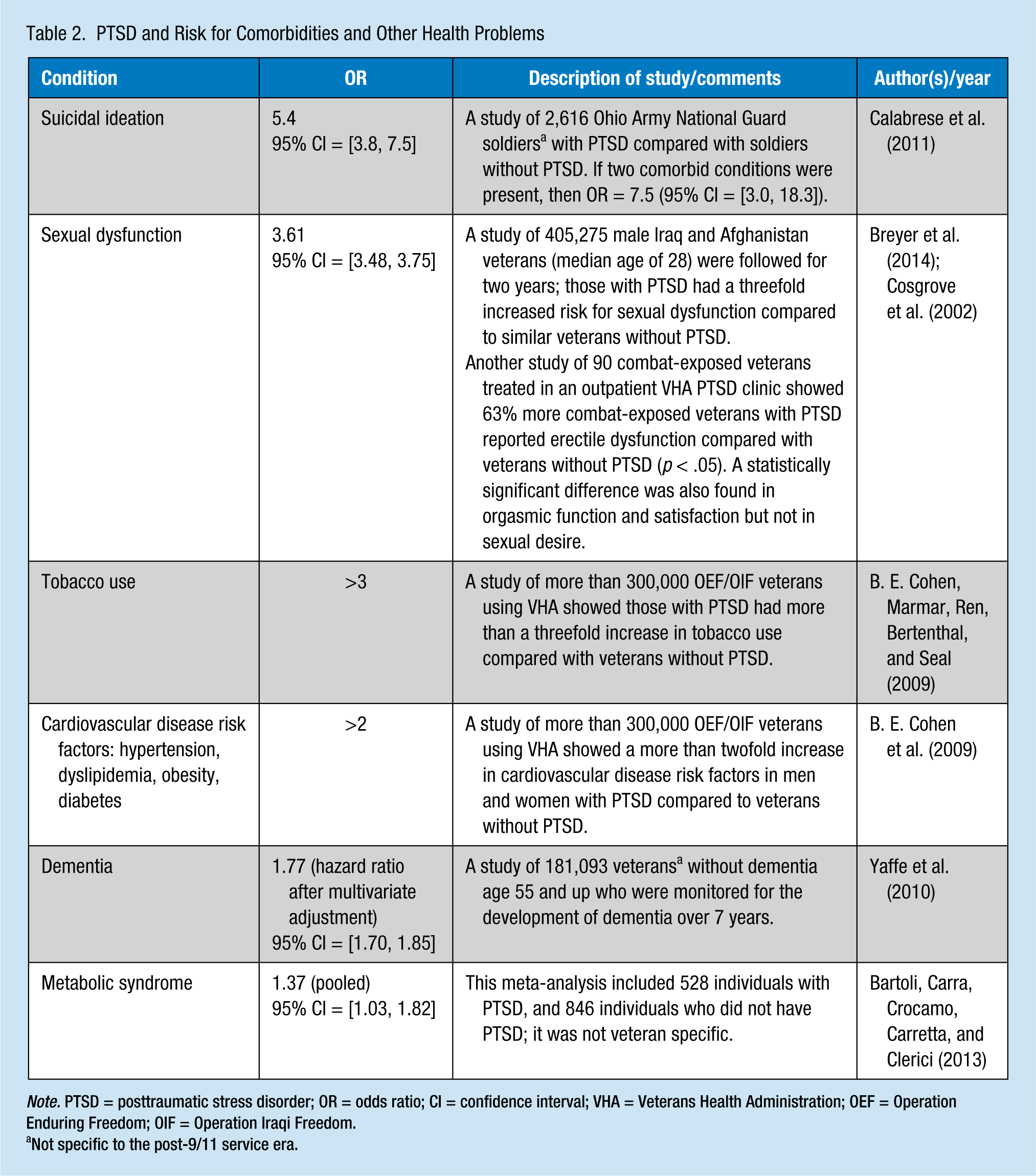
Note. PTSD = posttraumatic stress disorder; OR = odds ratio; CI = confidence interval; VHA = Veterans Health Administration; OEF = Operation Enduring Freedom; OIF = Operation Iraqi Freedom.
Not specific to the post-9/11 service era.
Military Sexual Trauma (MST)
Military sexual trauma is defined as psychological trauma, which results from a physical assault or sexual battery or harassment (i.e., repeated, unsolicited verbal or physical contact, which is threatening and sexual in nature); these experiences must occur while veterans are serving on active duty or training (“Veterans’ Benefits,” n.d.). A retrospective study of 125,729 OEF/OIF veterans’ health records who sought care from VHA primary or behavioral health providers showed 15.1% of women and 0.7% of men had an MST diagnosis associated with increased risk for mental health problems, including PTSD, anxiety, depression, and substance use disorder (Kimerling et al., 2010). An anonymous survey of more than 7,000 female active duty military personnel specifically focused on unwanted sexual contact; self-reported prevalence was 13.4%, and unwanted sexual contact was statistically significantly associated with depression (AOR = 2.04), anxiety (AOR = 2.20), PTSD (AOR = 2.78), suicidal ideation (AOR = 2.76), suicide attempt (AOR = 2.47), and recent tranquilizer misuse (AOR = 1.35; Stahlman et al., 2015).
Sexual Dysfunction
A notable connection has been established between sexual function and mental health problems. One of the explanations for this connection is the parallel between combat “highs” and sexual feeling. For example, PTSD may interfere with desire, arousal, and satisfaction because of PTSD hyperarousal and aggression (Yehuda et al., 2015). A small study of 197 Iraq and Afghanistan veterans showed that those veterans with sexual problems had higher PTSD symptom scores, particularly related to numbing symptoms (e.g., detachment and loss of interest; Nunnink, Goldwasser, Afari, Nievergelt, & Baker, 2010).
The common ages of deployed soldiers can also affect significant sexual development (Cameron et al., 2011). Military culture values hypermasculinity, hypersexuality, and traditional sex rules during deployment. For this reason, veterans may experience difficulty with intimacy and vulnerability post deployment (Cameron et al., 2011). The military culture may also have an impact on the 2.2% of veterans who are lesbian, gay, or bisexual (Gates, 2010). Limited access to contraceptives and lack of contraceptive education by the military could contribute to unprotected, risky sexual behaviors leading to unintended pregnancy and sexually transmitted infections (Duke & Ames, 2008).
Dementia
An increased risk for dementia has been noted with longer and more frequent deployments, PTSD, and possibly TBI (Sibener et al., 2014; Yaffe et al., 2010). A study of 51 athletes with chronic traumatic encephalopathy (CTE) showed symptoms (e.g., memory loss, irritability, aggression, headaches, and problems with speech, gait, and cognition) can appear as young as 25 years old; CTE is associated with repeated closed head injuries (McKee et al., 2009). The evidence is unclear, but CTE may develop from a single TBI event (McKee et al., 2009). Dementia is predicted to become more prevalent among veterans as post-9/11 veterans age and experience repeated trauma (McKee et al., 2009).
Traumatic Brain Injury (TBI)
Traumatic brain injury is a structural injury or physiological disruption of brain function from traumatic force; TBI is associated with decreased levels of consciousness, memory loss, altered mental state, neurological deficits (which may or may not be transient), and intracranial lesion (Wall, 2012). Traumatic brain injury has three categories of clinical presentation:
Somatic or sensory (e.g., headaches, dizziness, sensitivity to light and noise, difficulty sleeping)
Psychological (e.g., anxiety, irritability, depression)
Cognitive (problems with memory or concentration; Wall, 2012).
Mild TBI can vary from moderate to severe cases depending on symptoms, time course, and impairment; for example, a mild case may involve less than 30 minutes of loss of consciousness (Hoge, Goldberg, & Castro, 2009). Traumatic brain injury typically resolves within several days to several weeks (Schneiderman, Braver, & Kang, 2008).
Traumatic brain injury is common in Iraq and Afghanistan and is usually mild. A report by the RAND Corporation stated about 20% of OEF and OIF veterans experienced a probable TBI during deployment (Tanielian & Jaycox, 2008). The prevalence of TBI was up to 41% among 360 OEF and OIF veterans with burn and explosion injuries (Gaylord et al., 2008; Wall, 2012). A study of more than 2,000 Iraq veterans, mostly Marines, with TBI experienced between 2004 and 2008 showed 95% of TBI were due to blasts and 89% of TBI were mild; multiple injuries were common (MacGregor, Dougherty, & Galarneau, 2011). Traumatic brain injuries may also be caused by bullets, shrapnel, blasts, motor vehicle accidents (MVAs), air or water transport, and falls (Schneiderman et al., 2008).
Although TBI symptoms usually resolve within the month, some still experience persistent postconcussive symptoms (e.g., headache, dizziness, and balance issues); when symptoms of TBI continue beyond this time frame, the disorder is known as persistent postconcussion syndrome (PPCS; O’Neil et al., 2014). In a study of 275 OEF and OIF veterans who incurred mild TBI in combat, 35% reported PPCS associated with comorbid PTSD and three or more mechanisms of injury (Schneiderman et al., 2008). Persistent postconcussive syndrome occurs much more commonly among post-9/11 veterans than civilians with TBI (Hoge et al., 2009). Other risk factors (e.g., older age, female, less education, premorbid or reoccurrence of mental health problems, reduced resiliency, lack of support systems, chronic pain, severity of injury and acute symptoms presentation, and alcohol use) also contribute to the prevalence of this syndrome (Tsai et al., 2012; Wall, 2012).
A screening tool, TBI-4, can be used to identify veterans who could benefit from mental health services; a study of veterans with TBI showed those who scored TBI-4 positive were in greater need of such services (Olson-Madden et al., 2014). Screening for TBI is essential because about 57% of OEF and OIF veterans with TBI were never evaluated by a physician at the time of the injury or thereafter (Tanielian & Jaycox, 2008). Veterans with TBI should also be screened for behavioral health disorders (e.g., PTSD), which can present with similar symptoms (e.g., depression, irritability, and difficulty sleeping).
Polytrauma: The Interplay of Pain, PTSD, and TBI
The “signature” illness of post-9/11 veterans is polytrauma, described as an overlap of the following three conditions: pain, PTSD, and PPCS; in a study of 340 post-9/11 veterans who visited a VHA Polytrauma Network Site, all three of these heath conditions were present simultaneously in 42% of participants (Lew et al., 2009). A negative synergistic effect (i.e., each health condition worsened in the presence of the other health conditions) exists when pain can elicit PTSD symptoms and PTSD symptoms can exacerbate pain (Lew et al., 2009). A study analyzing the burden of illness in 90,000 OEF and OIF veterans showed those soldiers with PTSD had more comorbidities than those without a mental health condition; the most frequent condition reported for men and women with PTSD was lumbosacral spine disorders (Frayne et al., 2011). A small study showed 60% of 18 combat veterans with PTSD and mild TBI were prescribed medications (e.g., sedative, opioid, or mood stabilizer) that could affect performance, compared with only 6% of 33 control veterans without PTSD and TBI (Swick, Honzel, Larsen, Ashley, & Justus, 2012). Although a very small study, these findings are a glimpse into the complexity of veterans living with polytrauma. Providers should be cautious with regard to veterans who may be experiencing symptoms and taking prescriptions that can affect their ability to drive safely.
Substance Use Disorder
Substance use is common in veteran populations. A systematic review of 72 studies from 1995 to 2013 included more than 125,000 pooled veterans (97% male) and showed a 32% prevalence of alcohol use disorder and 20% prevalence of drug use disorder (Lan et al., 2016). As noted previously, veterans with TBI or PTSD are at increased risk for substance use disorder, and male veterans are at twice the risk for substance abuse compared with female veterans (Seal et al., 2009). Veterans with mental health conditions are more likely to use an opioid pain reliever, exhibit high-risk behaviors, and experience adverse clinical outcomes (Seal et al., 2012).
All veterans should be screened for substance use disorders. Expanding the use of substance abuse screening tools (e.g., Alcohol Use Disorders Identification Test [AUDIT], the CAGE Substance Abuse Screening Tool, and the Drug Abuse Screening Tool [DAST]) is recommended (Lan et al., 2016). Another tool found to differentiate high and low risk for opioid abuse, but not necessarily tested for validity with the veteran population, is the Opioid Risk Tool (ORT; Passik & Kirsh, 2008). Veterans with substance abuse issues should be carefully evaluated for other mental health problems and suicide risk.
Suicide
Veteran suicide is on the rise and occurs frequently (Bryan et al., 2015; Kang et al., 2015; McCarten, Hoffmire, & Bossarte, 2015). A retrospective cohort mortality study of 1.3 million Iraq and Afghanistan veterans showed a significantly higher risk for suicide among post-9/11 veterans compared with the U.S. population (Standardized Mortality Ratio [SMR] = 1.61, 95% CI = [1.53, 1.69]); interestingly, this risk was even higher among nondeployed veterans compared with deployed veterans (Kang et al., 2015). A meta-analysis of 22 studies covering many service eras, branches, and roles showed 25% of deployed veterans are at increased risk for suicide-related outcomes: ideation, attempt, or death (p < .0001; r = .08; Bryan et al., 2015). A cross-sectional study of 39,408 veteran suicides (i.e., not limited to veterans who used the VHA) showed the suicide rate increased 15% for men and 35% for women between 2001 and 2010 (McCarten et al., 2015).
In addition to a perhaps obvious, but important risk factor for depression, other suicide risk factors should be considered. A longitudinal study of more than 3 million veterans (not specific to the post-9/11 era) over 7 years assessed 7,684 suicides; the most prevalent risk factor for suicide among men was bipolar disorder (hazard ratio = 2.98, 95% CI = [2.73, 3.25]) and among women was substance use disorders (hazard ratio = 6.62, 95% CI = [4.72, 9.29]; Ilgen et al., 2010). Another study of more than 2,000 mentally ill veterans (not specific to the post-9/11 era), assessed through the National Survey on Drug Use and Health, showed self-reported alcohol dependency in the previous year increased the odds of suicide by 103% (AOR = 2.03, 95% CI = [1.20, 3.42], p < .01; Becerra, Becerra, Hassija, & Safdar, 2016). A cross-sectional retrospective study by Lemaire and Graham (2010) of 1,740 OEF and OIF veterans showed several factors were statistically significant for increasing the risk of suicide (Table 3). Other suicide risk factors included White race and ethnicity, recent demotion, junior enlisted rank, combat exposure, length of deployment, and survivor guilt as well as the experience of combat exposure coupled with PTSD and TBI (Bryan et al., 2015; Schoenbaum et al., 2014).
Suicide Risk Factors (Lemaire & Graham, 2010)
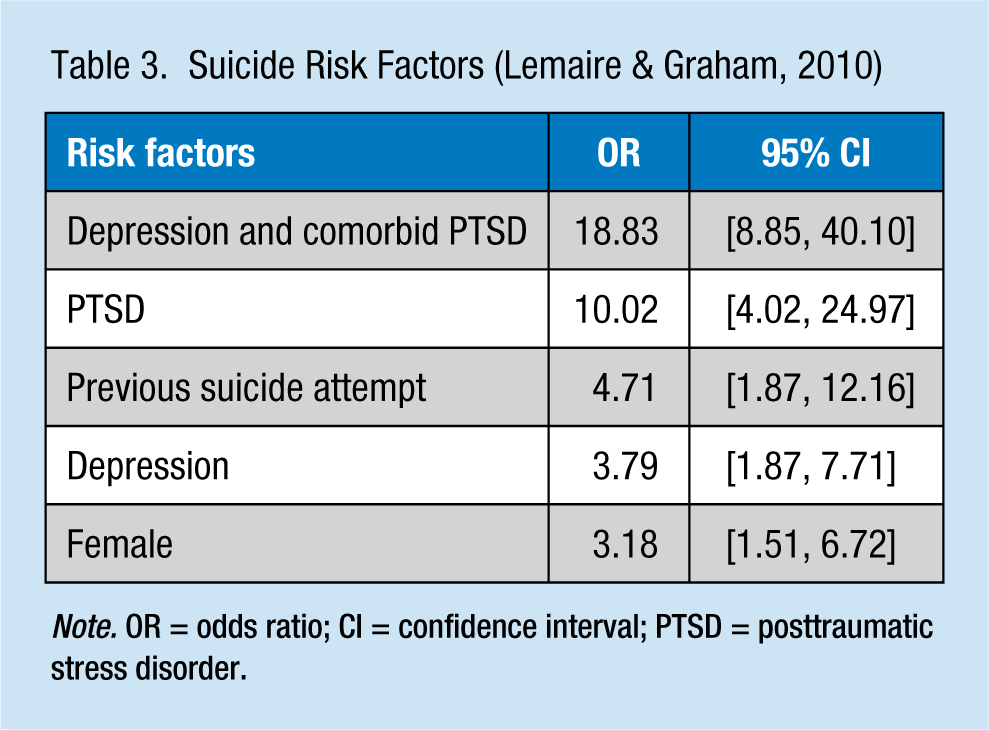
Note. OR = odds ratio; CI = confidence interval; PTSD = posttraumatic stress disorder.
All post-9/11 veterans should be assessed for suicide, not just upon their return from service, but continuously. Suicide rates for post-9/11 veterans were highest in the first 3 years after leaving the military (Kang et al., 2015). A systematic review of suicide risk assessment tools concluded that current research is not sufficient to validate a screening tool for suicide, but the Affective States Questionnaire (ASQ) may have some utility (Haney et al., 2012). Another approach is administering an evidence-based, comprehensive depression screening tool, such as the Patient Health Questionnaire 2 (PHQ2) or Patient Health Questionnaire 9 (PHQ9), to screen for depression as a suicide prescreening (Blue Ribbon Work Group Report, 2008). The VA and DOD have published a Clinical Practice Guideline for the Assessment and Management of Patients at Risk for Suicide to provide some structure and improve care for veterans (Assessment and Management of Risk for Suicide Working Group, 2013). Veterans should be asked about their access to firearms as they may have more knowledge about their use. A study of 320,890 males from several military service eras revealed veterans are 58% more likely than civilians to use firearms over other suicide methods (Kaplan, Huguet, McFarland, & Newsom, 2007).
Clinicians should also be mindful that although suicidal ideation may not be reported, suicide risk factors may be present (Ganz & Sher, 2013). If a veteran is determined to be at risk for suicide, immediate assistance can be accessed through the National Suicide Prevention Lifeline (1-800-273-TALK [8255]); veterans and their families should press 1. This service is available to all veterans regardless of VHA eligibility and can also be accessed via online chat at https://www.veteranscrisisline.net or by text to 838255. Postdeployment support has been shown to protect against the risk of suicide for post-9/11 veterans (OR = 0.95, 95% CI = [0.92, 0.98]; Lemaire & Graham, 2010). Another resource for veterans is the National Alliance on Mental Illness (NAMI) Homefront website for general resources from the DOD; this is a comprehensive list of resources available to veterans, including a 24/7 Real Warriors Live Chat, a resource to sort resources (NAMI, 2014).
Hearing or Visual Impairments
Hearing loss and tinnitus are two of the most commonly awarded service-related disabilities. Although some active noise reduction measures have been implemented in tanker helmets and in some aircraft applications over the last few decades, an IOM report stated military hearing conservation programs are not enough to adequately protect the hearing of service members (Humes, Joellenbeck, & Durch, 2005). About 75% of combat injuries are related to blasts, yet not all soldiers may be wearing hearing protection. In a systematic review of 14 studies, the prevalence of hearing problems ranged from 7% to 27%; more than half of veterans with hearing problems experienced a blast exposure (Theodoroff, Lewis, Folmer, Henry, & Carlson, 2015). Blasts can lead to hearing problems, such as permanent sensorineural loss or tympanic membrane rupture (Saunders & Echt, 2012). Notwithstanding potential hazardous noise levels in the military, the confirmation of hearing loss as service related can be difficult when pre- and postdeployment audiograms were not performed. Adding to this challenge, hearing difficulties have been reported by veterans exposed to blasts, even when no identified abnormal pure-tone sensitivity exists (Saunders & Echt, 2012).
Tinnitus can occur with or without hearing loss, although hearing loss increases the risk for tinnitus (Humes et al., 2005). The effects of tinnitus may affect veterans’ mental health and overall well-being, potentially affecting sleep, concentration, and the ability to function; tinnitus may lead to anxiety, fear, frustration, depression, and increased suicide risk (Humes et al., 2005). The interplay of symptoms among conditions is a consideration, particularly as the veteran is assessed for comorbid behavioral health disorders. For example, individuals with tinnitus and concurrent PTSD have been shown to have significantly poorer coping skills than those with tinnitus alone (Fagelson & Smith, 2016).
Blast injuries can also result in visual impairments. A cross-sectional study of 65 veterans with blast-related traumatic brain injuries showed a 25% prevalence of ocular surface injuries (Cockerham et al., 2014). Veterans who sustained a blast injury may have impaired visual acuity if there is an ocular surface injury or endothelial cell abnormalities; interestingly, no relationship has been found between the use of ballistic eyewear and the presence of ocular surface injuries from a blast (Cockerham et al., 2014). Other visual blast and closed head injury effects may include photosensitivity, oculomotor problems, and visual field losses as well as difficulties with color discrimination, spatial perception, and visual processing (Saunders & Echt, 2012). The veteran with visual damage from a blast may have difficulty with mobility and reading (Saunders & Echt, 2012).
Veterans exposed to blasts may incur both auditory and visual damage, known as dual-sensory impairment (DSI). This condition can affect veterans’ psychosocial functioning. For example, challenges communicating, particularly when the veteran has difficulty understanding speech, in addition to limitations in identifying visual nonverbal cues, may exist (Saunders & Echt, 2012). More research is needed on DSI to inform assessment and rehabilitation practices.
Respiratory Problems
Post-9/11 veterans may have been exposed to high levels of ambient particular matter. The World Health Organization’s (WHO) allowable daily pollution exposure level is 25 µg/m3, yet in Iraq and Afghanistan, the pollution exposures reached 10,000 µg/m3 for prolonged periods; geological dust, burn pit smoke, and heavy metal condensates were found in the three main components of air samples taken from Afghanistan, Iraq, and Kuwait (Engelbrecht et al., 2009). This high-ambient particulate matter is associated with short- and long-term respiratory effects. Iraq air pollution exposures, in particular, were associated with a significantly increased risk of asthma (OR = 1.58, 95% CI = [1.18, 2.11]) compared with the air pollution exposures of nondeployed veterans (Szema, Peters, Weissinger, Gagliano, & Chen, 2010). A longitudinal study of 46,000 veterans from all branches of the service who participated in the Millennium Cohort Study showed respiratory symptoms for Army and Marine Corps veterans and a linear association between respiratory symptoms and length of deployment for those in the Army (Smith, Wong, Smith, Boyko, & Gackstetter, 2009). Another study of 60,000 OEF and OIF randomly selected veterans showed deployed veterans were 29% more likely to have sinusitis compared with nondeployed veterans (AOR = 1.30, 95% CI = [1.13, 1.49]; Barth, Dursa, Peterson, & Schneiderman, 2014). Authors of a systematic review of 19 studies from 2001 to 2014 concluded more research is needed in regard to chronic lung disease and related exposures (Falvo et al., 2015). Compounding the risks of potential pollution exposures, approximately 42% of military men and 29% of military women aged 18 to 25 years smoke tobacco; about 22% of veterans smoke, which is slightly higher than the general adult population (Bondurant & Wedge, 2009).
Chronic Conditions
Chronic conditions are ubiquitous among veterans (Krejci, Carter, & Gaudet, 2014). A retrospective, cross-sectional study of cost data for the VHA health system studied trends with the most expensive patients. More than 5 million veterans were included, and the most expensive 5% of veterans accounted for 47% of all VHA costs. About two thirds of the most expensive 5% of veterans had three or more chronic conditions; the more multisystem morbidity, the higher the outpatient costs and the lower the inpatient costs. This finding underscores the need for well-coordinated care for chronic disease across outpatient services (Zulman et al., 2015). The following conditions were most common among the most expensive veterans:
Hypertension (63%)
Mental health (48%)
Diabetes (34%)
Depression (29%)
Ischemic heart disease (27%)
Cancer (25%)
Homelessness (14%).
Some studies showed higher frequencies of overweight or obese veterans, but a study of more than 287,000 veterans (not specific to post-9/11 veterans; Almond, Kahwati, Kinsinger, & Porterfield, 2008) revealed 73% of men and 54% of women are overweight and 25% of men and 21% of women are obese. The authors concluded no difference in overweight and obesity between veterans and the general population (Almond et al., 2008). Eating disorders may be present but also no more frequent than in the general population; eating problems may relate to trauma, the military’s strict physical requirements, or the condition of having little time to eat or binge eat after long periods without food (Bartlett & Mitchell, 2015).
Other Health Needs/Reintegration
Consideration should be given to psychosocial, cultural, and environmental dimensions of health (Boudiab & Kolcaba, 2015). Veterans who have just returned from deployment are adapting to civilian life and their predeployment roles in their households. The transition to civilian life post deployment can include a number of stressors (e.g., social exclusion, homelessness, alcohol misuse, unemployment, and mental health disorders; Ganz & Sher, 2013; Lange, 2009). Psychosocial needs can affect sleep, relationships, and parenting (Messinger, 2009). If an impairment or disability is present, veterans may lose their identities, not being able to engage in productive skills, hobbies, and other activities that were a part of veterans’ lives before deployment. This sense of loss can be intensified, especially if veterans’ injuries occurred during loss of control (Messinger, 2009). The veterans may have new environmental needs, such as wheelchair access in their homes. Despite the resources available to veterans, almost half of them report not receiving any support for reintegration into civilian life post deployment (Osinubi et al., 2012).
Post-9/11 Female Veterans
Although women may not work in combatant roles, they still may be exposed to combat or work in combat-exposed areas (Conard & Sauls, 2014). A study of 592 OEF and OIF female veterans showed they are just as resilient to combat-related stress as men (Vogt et al., 2011). Chronic multisymptom illness (CMI), which includes medically unexplained symptoms that lead to a loss of normal function (e.g., chronic fatigue syndrome, fibromyalgia, and irritable bowel syndrome [IBS]), is twice as prevalent among female Iraq and Afghanistan veterans than the average female veteran (p = .01; Mohanty et al., 2015). Compared with male veterans, female veterans are more likely to report a service-connected disability, a mental disorder, more prior life stressors, sexual harassment, depression, more PTSD comorbidities, and non-PTSD anxiety (Frayne et al., 2011; NCVAS, 2015a; Vogt et al., 2011).
The Role of the Occupational Health Nurse
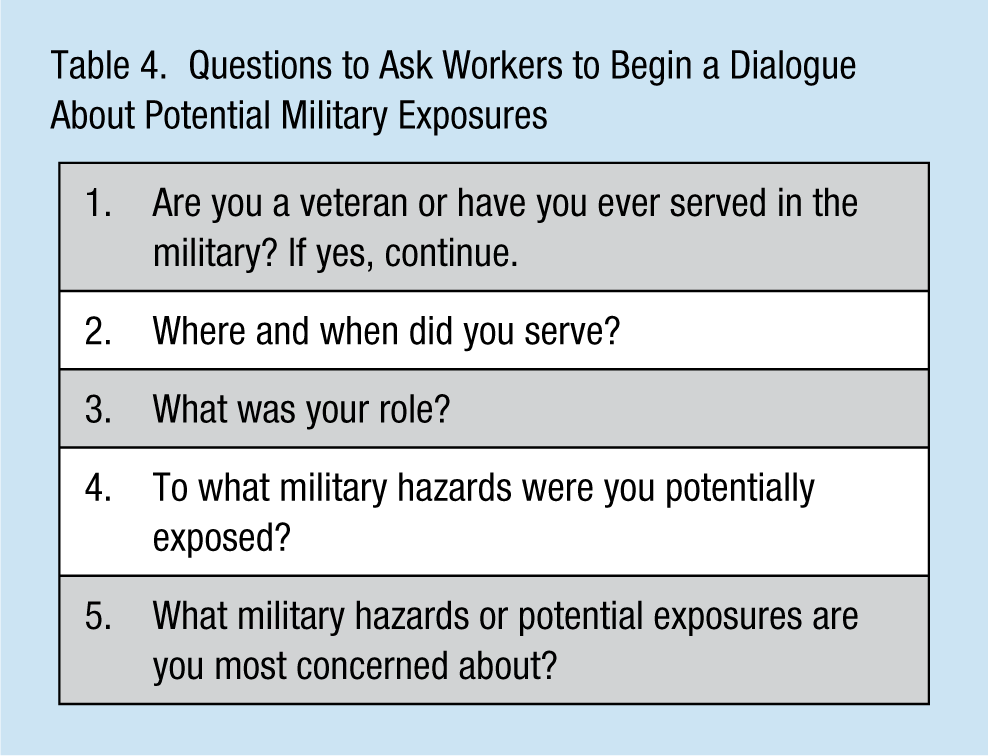
The health care needs of post-9/11 veterans may be poorly understood or appreciated. The primary step for nurses is to identify veterans by asking them whether they have ever served in the military and initiate a conversation to gain an understanding of their service experience; some sample questions to initiate this dialogue are provided in Table 4. Nurses should use a multidisciplinary approach to the care of veterans and include input from their spouses, children, or other family members, who may be able to shed more light on the needs and functioning of the veterans. The variety of military hazards to which veterans may have been exposed and health problems for which they may be at high risk are summarized in Table 5. Nurses can advocate for substance use disorders, PTSD, depression, and suicide risk evaluation of all veterans regardless of military experience. Validated screening tools, such as some examples listed in Table 6, can be used in addition to a clinical diagnostic evaluation to identify these conditions.
Questions to Ask Workers to Begin a Dialogue About Potential Military Exposures
Health Problems Among Post-9/11 Veterans Depending on Military, Individual, and Other Factors Before, During, and After Service
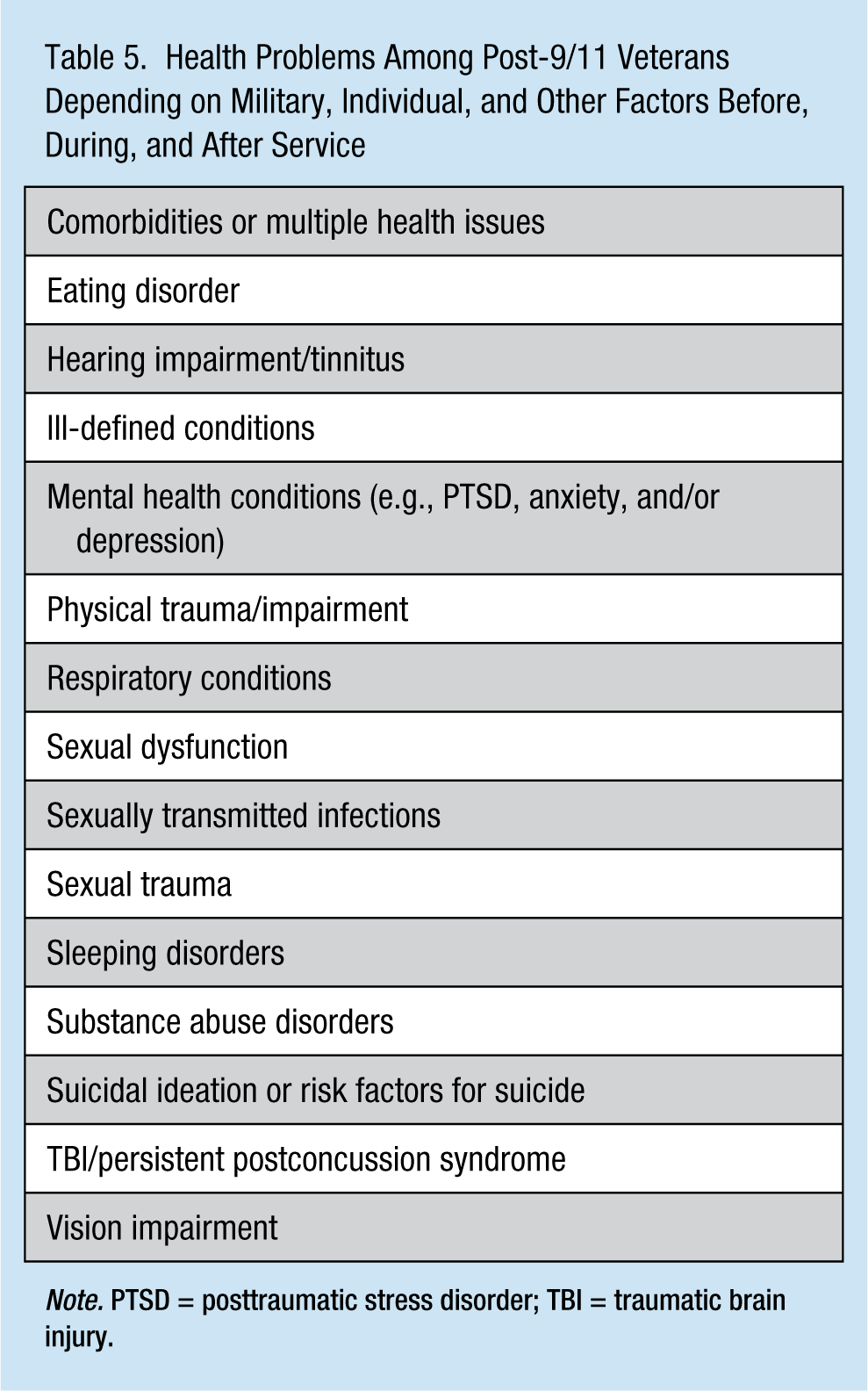
Note. PTSD = posttraumatic stress disorder; TBI = traumatic brain injury.
Summary of Screening Tools for the Occupational Health Nurse Providing Care to Post-9/11 Veterans
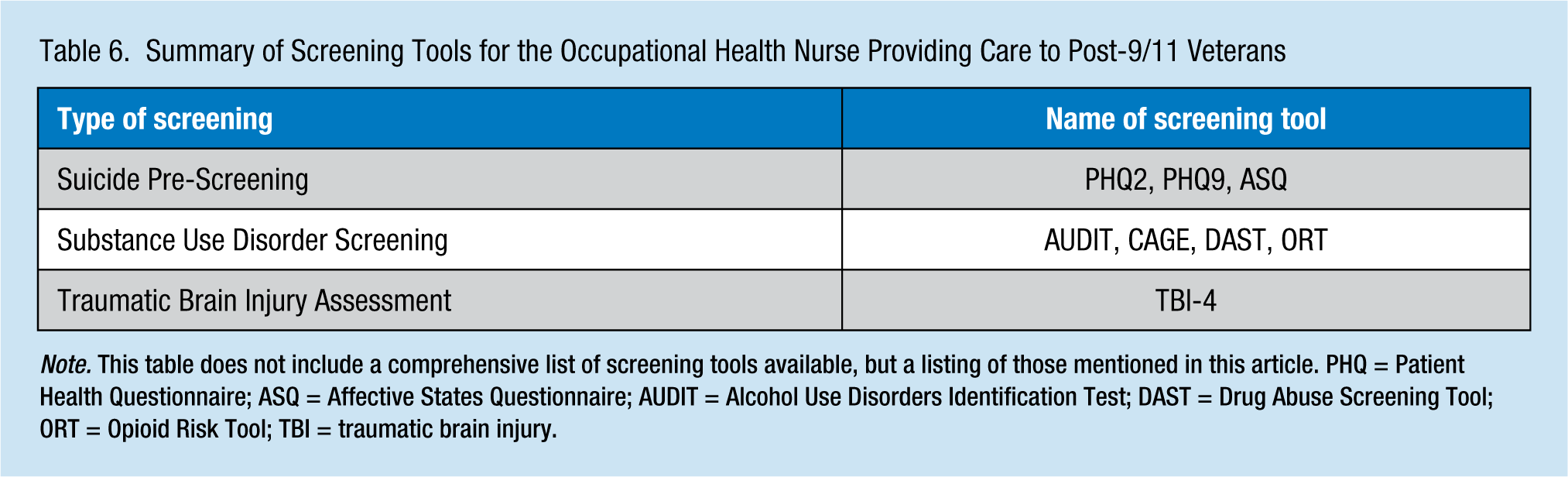
Note. This table does not include a comprehensive list of screening tools available, but a listing of those mentioned in this article. PHQ = Patient Health Questionnaire; ASQ = Affective States Questionnaire; AUDIT = Alcohol Use Disorders Identification Test; DAST = Drug Abuse Screening Tool; ORT = Opioid Risk Tool; TBI = traumatic brain injury.
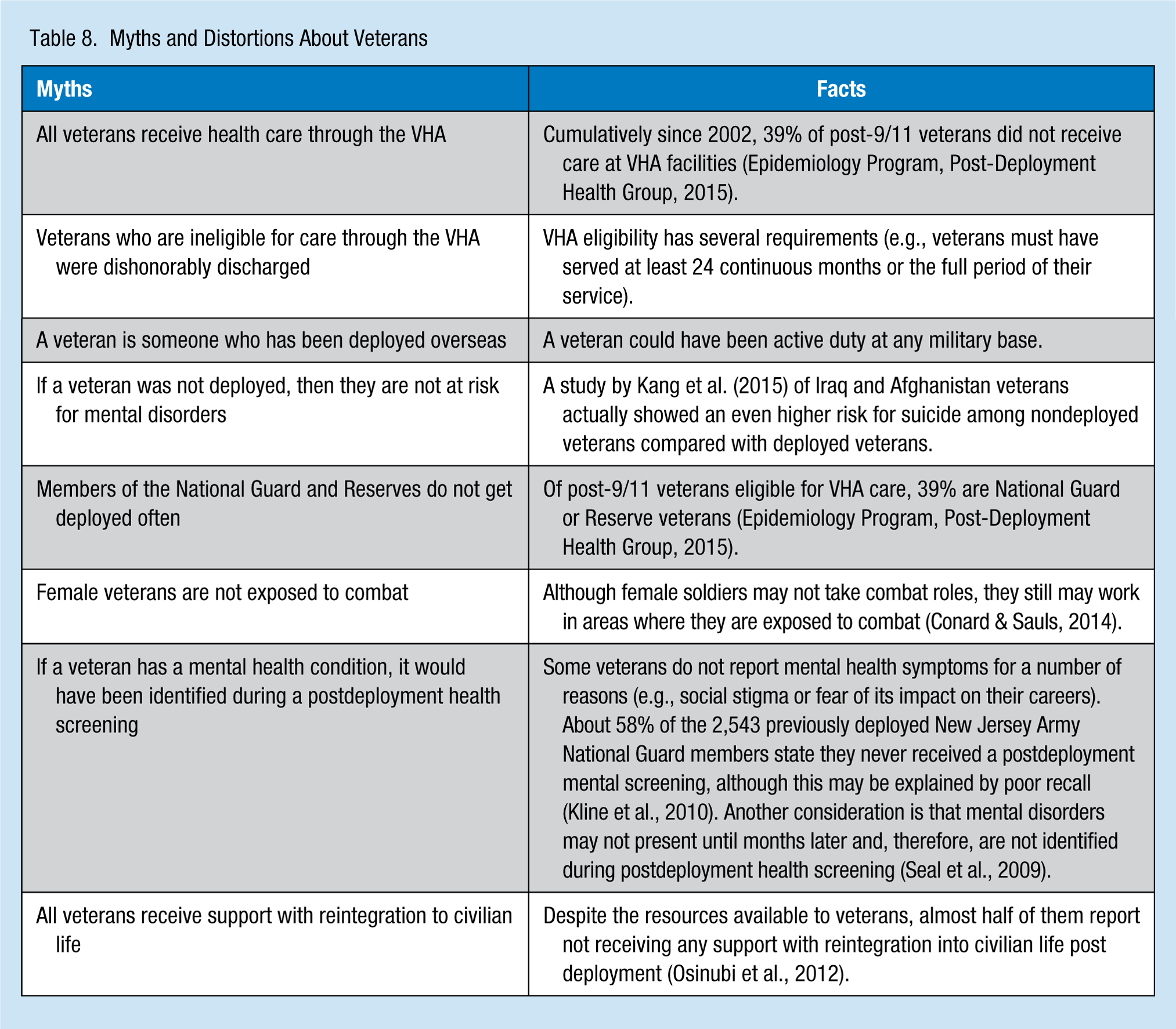
Many potential barriers to care, such as structural limitations, personal beliefs, and socioeconomic factors, are confronted by veterans (Tanielian & Jaycox, 2008). It is important for veterans to access appropriate health care. A veteran with unmet health care needs has a significantly increased risk for suicide compared with veterans without unmet health care needs (AOR = 4.11, 95% CI = [2.74, 6.17], p < .001; Becerra et al., 2016). Many studies have found social support is a factor in veterans’ behavioral health outcomes including PTSD (Wright, Kelsall, Sim, Clarke, & Creamer, 2013). Nurses should ensure veterans have access to primary and behavioral health care, social support, and other specialty health care services (e.g., rehabilitation or smoking cessation programs) and have coordination and continuity of care among health care providers. The importance of psychosocial, cultural, and environmental elements and how these elements may affect the health of veterans should not be underestimated, especially the adequate provision of basic essential components (e.g., safe and adequate housing, access to healthy food, and employment). A list of resources available to veterans are shown in Table 7. Nurses can educate themselves and their colleagues about this unique working population to break the myths and false beliefs about veterans (Table 8).
Resources for the Occupational Health Nurse Providing Care to Post-9/11 Veterans
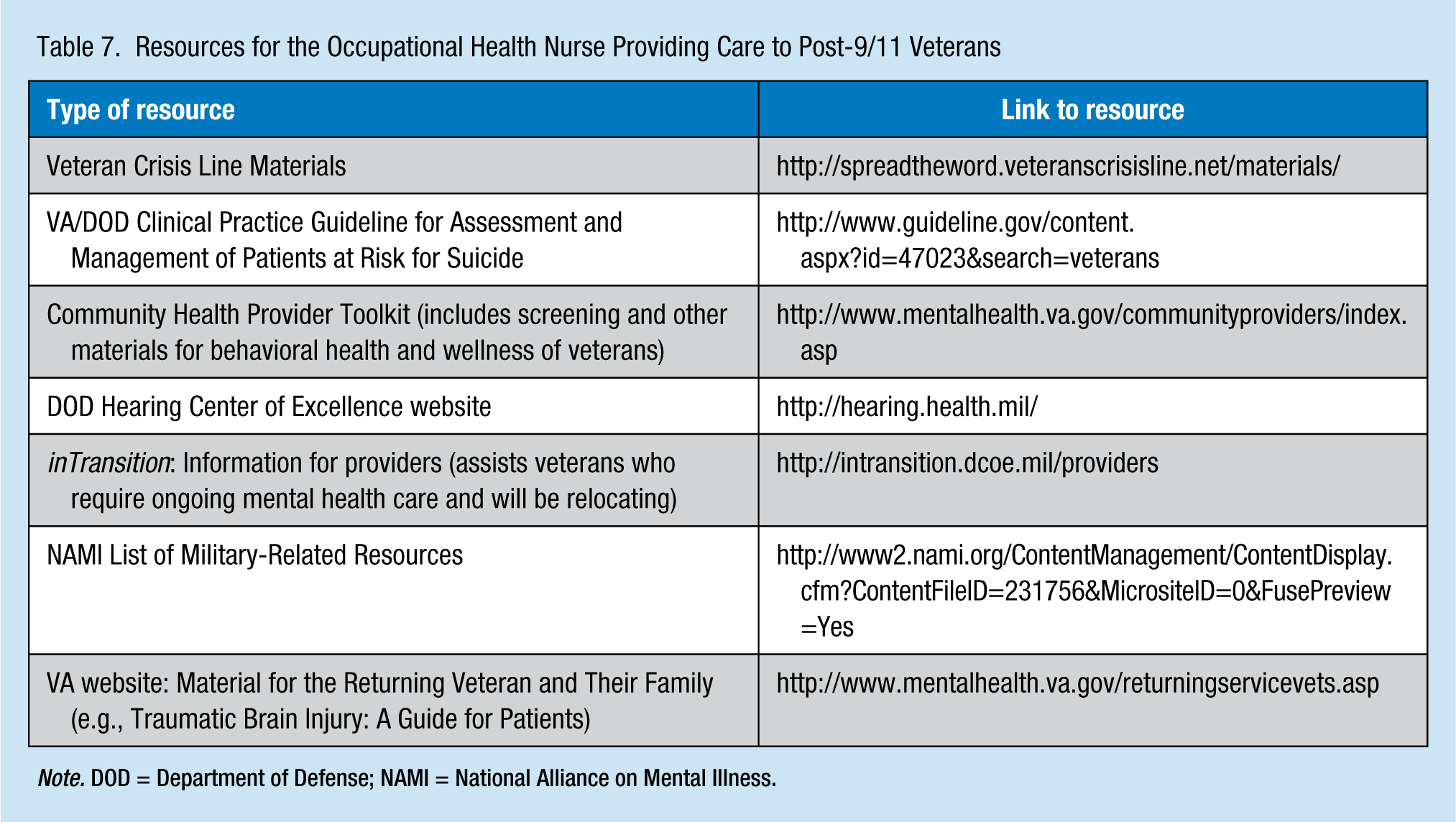
Note. DOD = Department of Defense; NAMI = National Alliance on Mental Illness.
Myths and Distortions About Veterans
Summary
It is not uncommon for veterans to seek care from civilian health care systems, so it is important for all health care providers to be informed about veterans’ needs to ensure the provision of appropriate care to veterans in an environment that is comfortable for them. Today’s post-9/11 veterans have complex, comorbid primary and behavioral health needs (e.g., polytrauma, multiple injuries, chronic health conditions, and ill-defined problems). Although some post-9/11 veterans may have served in the same military operation, their exposures and experiences differ. Becoming more familiar with the nature of military hazards and complexity of veterans’ health needs is one step toward ensuring the provision of veteran-sensitive care.
Limitations
Potential work exposures for veterans are vast and multifactorial. This article identified the more common issues for post-9/11 veteran populations. Most of the research presented was found in or through systematic reviews and meta-analyses published within the last 5 years. Therefore, individual primary studies with findings that have not been summarized in a review or studies older than 5 years may not be included.
Results of the included studies are not necessarily generalizable to other types of veterans (e.g., other branches, eras, or locations). Most studies of post-9/11 veterans were based on VHA data, yet many veterans do not seek care through the VHA. Cumulatively since 2002, 39% of post-9/11 veterans did not receive care within the VHA (Epidemiology Program, Post-Deployment Health Group, 2015). Data collected by the DOD, especially related to mental health, may be underreported (Kline et al., 2010). Inconsistencies in the terminology used in studies (e.g., definitions and calculations of veterans, PTSD, depression, and suicide) may differ dramatically (Tanielian & Jaycox, 2008).
Applying Research to Practice
There is a large, growing, and diverse population of veterans from the post-9/11 era who have unique and complex primary and behavioral health needs relating to polytrauma, co-morbid chronic conditions, and/or ill-defined problems. This article summarizes some of the most common health problems reported and treated in this population. Becoming more familiar with these issues will inform occupational health providers and ensure the provision of more veteran-sensitive care. The most important first steps are to understand who a veteran is and who they are within the workforce. Veterans should be interviewed to understand the nature of their military experiences and potential hazard exposures as well as what kind of health issues they may be having or are concerned about. This detail can provide important information regarding the veteran’s history and needs, so the occupational health nurse can advocate and connect them to resources accordingly.
Footnotes
Acknowledgements
The authors thank Laura A. Fennimore for her guidance with this research and Maria Falca-Dodson, Mary Ditri, Lori S. Frank, and George May for their thoughtful input.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Daria L. Waszak is a faculty member with the RN-to-BSN Fast Track Program at Felician University in New Jersey and a DNP student at the University of Pittsburgh.
Aline M. Holmes is the senior vice-president for Clinical Affairs and director of the Institute for Quality and Patient Safety with the New Jersey Hospital Association. She is also codirector of the New Jersey Nursing Initiative and a U.S. Navy Nurse Corps veteran.