
Abstract
Nurses are at significant risk for work-related injury, and ultimately disability. The purpose of this intrinsic single-case study guided by Yin’s and Stake’s iterative analytic processes was to examine one case of a registered nurse with a profound disability to determine whether this experience aligned with previous research and to examine whether a nurse with a profound physical disability could remain working in a clinical setting. The case study subject (a nurse with a profound physical disability) and the participants (people who knew, worked, and cared for the subject) were interviewed using a semi-structured interview guide. Interviews were transcribed and analyzed using Yin’s mental framework and iterative analytic process. Participant verification, whereby the researcher confirms the data with each participant, was obtained. The results were aligned with previous studies and support the need to provide environments that utilize and retain nurses with physical disabilities. Nurses with physical disabilities can practice safely in patient care settings, provided there is a supportive culture and willingness to make accommodations. Occupational health nurses have the expertise to take the lead in educating nurses and managers to provide this supportive culture.
Introduction
To date, research on the experiences of nurses with disabilities has consistently revealed perceptions of discrimination, resulting in their inclination to hide their disability whenever possible (Neal-Boylan, 2012), and attempts to compensate for what others question based on the assumptions about patient safety (Neal-Boylan, 2014; Wood & Marshall, 2010). Nurses with disabilities frequently go back to school to prepare themselves for less physical jobs (Neal-Boylan, 2012, 2014; Neal-Boylan, Fennie, & Baldauf-Wagner, 2011; Neal-Boylan et al., 2012). Others leave the profession altogether. Neal-Boylan and Miller (2017) observed that many nurses with disabilities hide their disabilities while in nursing school and persevere despite the barriers to graduate. In two other studies (Neal-Boylan, 2014; Wood & Marshall, 2010), nurses with disabilities found jobs with employers who were not nurses or who had disabilities themselves and, consequently, had fewer misconceptions and concerns about what nurses with disabilities could do. These employers were supportive of the nurses with disabilities. The nonnurse employers seemed to assume that the nurses knew what they had to do and how to do it safely and did not question their abilities. The nurse employers who had disabilities or chronic illnesses were supportive of nurse employees with disabilities and aware that they were capable of performing safely.
The experience of a nurse with a profound disability is not well represented in the literature. Prior studies have been conducted on nurses with disabilities, but to date, there are no studies using the case study research method (Yin, 2012) to explore a case of a nurse with a disability. The word profound was used to describe the disability of the study subject because the disability was the result of a severe, debilitating injury resulting in significant limitations to the use of both legs. Also, the nurse who is the subject of this case study used the word profound to describe her disability. An in-depth analysis of a case was conducted for purposes of adding to our understanding of what it is like to reenter the profession following an unexpected profound physical disability and attempting to return to previous nursing work. The case of a nurse with a profound disability gives us the opportunity to question whether it is necessary or appropriate to discourage a nurse with any physical disability from working as a nurse in a clinical setting. The answer may also be applicable to other people with disabilities in workplace settings.
Background
Nurses are among the highest occupational groups for sustaining occupational injury that requires lost time from work in the United States (U.S. Department of Labor Bureau of Labor Statistics, 2018), placing them at risk of disability. In 2000, the National Sample Survey of Registered Nurses (RNs) indicated that 7% (n = 1,630) of nurses who responded to the question in the survey identified that they had a disability or illness that resulted in their employment outside of nursing (Spratley, Johnson, Sochalski, Fritz, & Spencer, 2001). In 2008, 1.3% (n = 5,670) of the nurses who responded to the same survey question changed employment because of a disability (Health Resources and Services Administration, 2010).
Although prevalence estimates of RNs with disabilities is not known, approximately 13% of people of all ages living outside of institutional settings consider themselves to be disabled (Erickson, Lee, & Von Schrader, 2014). In a recent study, half of the people who self-reported as having a disability were between the ages of 18 and 64 years (Erickson et al., 2014). Slightly less than half in that age range were employed compared with 76% of people in the same age range without a disability (U.S. Census Bureau, 2015). This employment gap has steadily increased since 2009 (Kraus, 2017).
Research has found that nurses with disabilities tend to hide their disabilities if possible, to avoid stigma and discrimination (Matt, 2008; Neal-Boylan, 2014; Neal-Boylan et al., 2012). Despite their experience and expertise, nurses with disabilities are often encouraged to leave their positions and their organizations due to concerns about patient safety and misconceptions about the level of care the nurse can safely provide (Matt, 2008; Neal-Boylan, 2014; Neal-Boylan et al., 2012). However, some nurses have been able to find employment despite their disabilities (Neal-Boylan & Miller, 2017). Nurses are typically unaware of their legal rights and may not ask for help when they think their rights have been violated (Neal-Boylan & Miller, 2017). A prevailing theme in the research on nurses with disabilities is that they want to be treated like everyone else while still having their individual needs addressed, in the context of potential accommodations (Neal-Boylan & Miller, 2017).
Method
A single intrinsic case study design was selected with the intent of increasing our understanding of a case of particular interest. This case is not necessarily representative of other cases and was not studied to develop or build a theory describing a particular phenomenon (Baxter & Jack, 2008; Stake, 1995). A single-case study allows the researcher to systematically analyze a situation, organization, or experience in depth, to enhance the understanding of a situation, and is appropriate if the researcher seeks to explore contexts that may be relevant to a situation (Baxter & Jack, 2008; Stake, 1995). The case study approach is based on a constructivist foundation that truth depends on perspective (Baxter & Jack, 2008; Stake, 1995). The study was approved by the Massachusetts General Hospital (Partners Organization) Institutional Review Board (IRB).
Description of the Subject of the Case
Marcia (pseudonym) was a baccalaureate-prepared RN in her early 30s living in the northeast U.S. when she suffered a severe debilitating injury that resulted in the loss of function in both legs. She had been working on a very busy medical floor in a large teaching hospital in major metropolitan area. The job was extremely physical. The nurses and support staff on the hospital unit developed a culture of support. Marcia worked in clinical care for 5 years before her accident. Following the accident, multiple surgeries, and extensive rehabilitation, she had reduced mobility and energy. She could not stand for long periods and sometimes had to use crutches or a wheel chair to take the pressure off of her lower extremities. Her recovery lasted 5 years before she felt she could resume working as a nurse.
Participants: The Case Subject’s Coworkers and Care Givers
The subject identified five people for the researcher to interview who could add depth and understanding to the experience of the subject. Two nurses and one former nurse’s aide had worked with the subject prior to her disabling injury, and one occupational therapist (OT) and one physical therapist (PT) took care of her following her injury. All the participants had remained in close contact with the subject and could speak to both her past and current experiences. The doctorally prepared OT, age 32 years, met the case subject approximately 1 year after the initial injury and treated her while she was undergoing inpatient and outpatient rehabilitation. She has known the subject for 4 years. The doctorally prepared PT, age 33 years, met the subject approximately 1 year after the initial injury. The baccalaureate-prepared RN, age 49 years, has known the subject for 10 years and worked on the same unit when the subject was injured. A family nurse practitioner, age 29 years, was working as an RN on the same unit before the injury. Finally, a nurse practitioner, age 28 years, was a nurse’s aide when she met the subject on the same unit before the injury.
Data Collection
The case study subject was interviewed on three occasions for approximately 1 hour each. Each of five participants, whom the subject identified as able to provide depth and breadth to the analysis, was interviewed for 1 hour. Interviews were audiotaped and transcribed verbatim. As each interview was completed, it was compared with the other interviews and new themes emerged. The researcher reviewed the data using an iterative approach, coding for similar themes as the interviews and analysis progressed. Themes were placed into a coding structure and were eventually grouped through a process of constant comparative analysis. As new themes emerged from each interview, they were used to develop questions for the interviews that remained. Analysis of themes occurred keeping in mind Stake’s (1995) focus on direct interpretation of the individual situation and categorical aggregation to search for meaning. Participants confirmed the accuracy of the data via participant verification. Rigor was established and maintained through this iterative process, purposeful sampling, systematic collection and organization of the data, a detailed record of the process, and participant verification (Gray, Grove, & Sutherland, 2017).
An unstructured interview guide was developed and provided a mental framework (Yin, 2012) from which the researcher derived the questions and helped determine the flow of the interview. Yin (2012) recommends that the researcher retain a degree of skepticism and consider other explanations than what is discovered during the study. This is akin to “bracketing bias” in other qualitative studies. Interviewing both nurse colleagues and the subject’s caregivers supported this effort. The researcher also sought to clarify whether each of the participants felt similarly to the others on specific points. Consequently, the researcher specifically asked participants about topics and points raised by the other participants to discover discrepancies. Participants were asked how they knew Marcia, and for how long and in what capacity. They were asked to describe how they thought Marcia had been affected by the disability, specifically in her work and in school. Participants were also provided with opportunities to add additional comments.
The subject gave informed consent and the five participants were each provided with a one-page document that listed participant information. Per IRB instructions, participation in the interviews was considered consent. The subject was interviewed in person on the first occasion and over the phone on two subsequent occasions. The five participants were interviewed individually over the phone. The unstructured interview guide was used to begin the interview, but as themes emerged from the data, questions were added to explore these themes. The researcher used active listening and probing questions to encourage sharing from the subject and the participants. Clarifying questions were asked, as needed and appropriate to confirm the researcher’s understanding.
Findings
One of the participant coworkers described the unit on which Marcia had worked before the injury and to which Marcia desired to return: As long as a nurse comes to work and does the job she/he’s supposed to do, no one is going to care if they’ve had a crisis at home or hold it against them if they have something personal going on. We have each other’s backs and support colleagues if they have to switch shifts or make a change because of personal issues. Management deals with those issues because the nurse doing bedside care doesn’t have the time or inclination to worry about those issues.
Three major themes emerged from the study: nursing self and others, the new normal, and empathy.
Nursing Self and Others
During rehabilitation, Marcia’s therapists initially found her to be overwhelmed. She was not used to being a patient, let alone a patient with a profound disabling injury undergoing therapy with others who had similar injuries. She was frustrated and had little hope for the future. The therapists agreed that personality and inner drive made a difference in Marcia’s recovery. One therapist commented, The keys are the person’s value to the team and their personality. Inner drive and personality are priceless. If you sat around before the injury, you probably will be inclined to do so after the injury, but if you were a driven, motivated person before you will probably continue to be that person and that goes a long way.
The therapists who cared for Marcia during rehabilitation described her nursing knowledge as both an advantage and a disadvantage. One therapist said, Because she was a nurse, she knew a lot more than our average patient and was able to help us help her more than our average patient could. However, having so much information wasn’t always a benefit to her because she knew so much of what she was going through and would be going through. It was definitely an advantage that she knew so much but it was also hard for her sometimes.
Marcia started advocating for her fellow patients. She also helped other patients advocate for themselves. Her natural nursing inclination to advocate for her patients slowly superseded her concerns for herself. She began to take online graduate classes, both to keep herself busy intellectually and to begin to prepare herself for returning to nursing.
The New Normal
Marcia was used to providing care and accommodations for others but not for herself. She had to transition from thinking and moving at a moment’s notice to carefully planning her day and her life. According to Marcia, “As much as I want to be normal and things to go back the way they were, it’s not long before I realize I’m not normal and I bounce back and forth between those two things.”
After several years out of the workforce, Marcia wanted to return to her old unit. She considered herself very fortunate to have a manager who was supportive and willing for her to come back, but she was offered a role created especially for her. The new position involved writing reports, working on projects, and being a second or third nurse in a room during patient care or a crisis. Marcia described her own doubts about returning to her previous position: I’m in a room wondering should I be doing this. I can do it, but what if I trip, fall, what if I lose my balance and pull on someone’s central line. It could have happened before when I was not injured but now that I have this profound disability, I never know what’s going to happen and G-d forbid something does happen, I feel like the blame’s gonna come down on me—I shouldn’t have been doing it.
Marcia struggled to hide her feelings about not being able to return to her previous role while understanding that she could not safely meet the physical demands of the previous role. She said, I do a lot of acting at work now, hiding how I really feel because, I’m overwhelmed with a lot of feelings. I don’t want to bring them into work. Before this happened, I could separate my personal and professional life but since the injury, I’m trying very hard to find my professional side again.
Marcia was keenly aware that patients could detect that she had a disability when her energy level required that she come to work using crutches. She wanted to be anonymous and professional, to have the focus on the patients and not on herself. As she indicated, I don’t feel like I have a right to [my needs] in my nursing world . . . I’m less comfortable voicing my needs. Very different dynamic—patient to nurse and nurse to nurse. As a patient, I could be [a] squeaky wheel. As a nurse, I want to fit in and not be vocal about things.
Marcia struggled with trying to hide the disability and wanting to be “normal” as she said: You wear your disability so publicly. [It’s] hard to go back to professional space and keep it private. The [nursing] shift is not about me, so discussing my journey or my body doesn’t have space there. Nor do I want to talk about the worst day of my life with strangers. Before, I had more privacy then I do now. There’s a push and pull of “I’m so lucky to be here, and what else can I contribute.”
Marcia felt indebted to her coworkers who stood by her throughout her recovery and often stayed with her through multiple surgeries and setbacks. One of the nurse practitioner participants said, [Marcia’s] knowledge of this patient population could be useful to her in other settings. We will all eventually be disabled by illness, age or injury, but I don’t think every job can be done by every person. Our unit has expanded our view of what kind of nurse is important to our floor, but there are still things that cannot be done sitting down. A nurse with an extreme sense of responsibility like [Marcia] will not feel right if she can’t do the job well or properly. It’s better that she use her intellect to be a great nurse.
Empathy
Marcia experienced a grieving process as she worked through the realization that she could not physically manage the job she had done before and had to reinvent herself: It’s like seeing the job I used to do and not doing it. It’s almost for me been more painful to go back to the place where I used to fly around the corner and walk a mile. I didn’t anticipate how painful it would be. Going back to school helped. Recovery was so long, I didn’t know if it would lead to a degree but it was so therapeutic. It didn’t mean I couldn’t keep learning. It started as a way to keep connected to the profession. People were telling me that school was the way to go for me because of what happened, and encouraging me. My mentors knew I wasn’t ever going to return to the job I loved and this was the way to go.
As a patient, Marcia was vocal about her needs. As a nurse, Marcia was less vocal and strived to fit in. She said that she learned to appreciate patient suffering in a way she had not before the injury: It’s a constant reminder—as a nurse we are educated on policies and procedures and how things should feel, but bottom line none of us really know because there are few of us who have really undergone these things. I found myself [reacting] to all the ways I had comforted my patients because it was me in bed. Not wanting to leave the ICU because I was confident and comfortable with the care there. How many times I told patients [insertion of a ] PICC [peripherally inserted central catheter] line was a little sting. My own PICC line . . . was uncomfortable and painful; two failed and they had to go to other arm . . . I’d like to think I gave compassionate care before this happened, but I just don’t really think it’s possible. Maybe some empathy, but we don’t know what it’s like in that bed. As long as we remember that we are never going to know how it feels to be that exact person in that bed with that experience.
Marcia saw herself as a very good nurse before the injury but as a better and different nurse since the injury because she developed an understanding of how catastrophic a profound injury or illness can be and that the platitudes from health professionals really do not help: I come with a different set of skills now in addition to what I had before. To be nice, people say “you will be such a good nurse now.” I was a good nurse when this happened. But I am a totally different person now and a totally different nurse . . . . No matter how many patients you take care of with [a particular disease], you’ll never know what it’s like so that patient will have the expertise you don’t have. The patient is always heard and respected and might help you catch on to things sooner; like [when the] family says “I can’t put my finger on it, something’s happening with my mom today.” A good nurse puts weight in that statement. We can study it. It’s valuable what you learn at the bedside, but can’t replace what the person is experiencing.
In addition, Marcia learned to be less judgmental about what a patient might be going through or feeling: Everything is so much easier said than done. It’s very easy to be on the other side of the bed rails, judge that the person isn’t really trying, a complainer. [It’s] very easy to be dismissive when it’s not you or your loved one. It was a common theme. No matter how much my practitioners, no matter their skill level, I was constantly reminded that I was the one going through this and no one could understand. It was hard not to reflect on my time as a nurse . . . . Was I as empathetic and as kind, as understanding as I could have been? Was I aware of what the patient was going through at that time? I did a lot of reflecting on my own time as a nurse.
Pregnant nurses and others with temporary limitations are treated differently on her hospital unit from nurses with permanent disabilities. According to one of the nurse practitioner participants, “The nurses that do not have disabilities accept that as the way things are and the nurses with disabilities also accept it as the way things are.” Another nurse practitioner stated, Anytime you get a clinician with more life experience in general, you get a better-rounded workforce. A person with disability might point out how you run your unit, how they see the world, [with a] different lens, adding to your workforce. In a way some places are trying to hire nurses with different ethnic backgrounds, they might explain how people [from different cultures] might experience pain differently. I think a nurse with a disability can offer that experience as well.
Limitations and Conclusion
Generalizability of single-case studies is limited. However, the findings from this case study confirm the findings from the previous studies on nurses with disabilities (Matt, 2008; Neal-Boylan, 2012, 2014; Neal-Boylan et al., 2011; Neal-Boylan et al., 2012; Wood & Marshall, 2010). For example, Marcia tried to hide her disability when possible, wanted to be treated like everyone else, and she and others had concerns about nurse and patient safety. Her desire to fit in contrasted with her need to conform to a new normal. Marcia described feeling indebted and that she was not entitled to vocalize her feelings because she was being given a job, even if it was one she found unchallenging to her expertise and abilities. Her vibrant personality helped her meet challenges head on, both while a patient and when considering her return to nursing. Like other nurses with disabilities in previous studies, she returned to school both to keep herself engaged in nursing and to prepare herself for less physically demanding work. She became less proactive when trying to advocate for herself and her own needs once she was back in her nursing role. Her natural inclination to take care of others prevailed over her own pain and limitations. She was profoundly changed by her own experience as a patient and could never practice nursing in the same way again. Marcia learned that the nurse with a disability has a very different perspective on what patients are experiencing and how the settings in which nurses work might be improved as a result of that perspective. She developed greater empathy for patients because she had undergone many of the same experiences as the patients on her old unit.
Implications for Occupational Health Nursing Practice
This case study illustrates that a nurse with a profound physical disability can return to nursing as a better nurse than before. Although she or he may not be able to safely perform the same functions as before or be in the same setting, the nurse has a lot to offer patient care. Marcia’s hospital unit had a naturally supportive culture and her manager was used to and willing to make accommodations, going so far as to develop a new position to keep Marcia on the unit.
Marcia eventually recognized that she could not provide the level of care as before, but she could remain with her colleagues and contribute to the unit. Occupational health nurses are in an ideal position to facilitate return to work for nurses and others with physical disabilities and to encourage a supportive culture (Davidson et al., 2016). Marcia’s high acuity unit created a less physically demanding job for her; however, it is not always possible to remain in the same clinical setting. Occupational health nurses can educate nurses and other staff that a nurse with a physical disability, even one that is profound, is likely to be able to continue to contribute experience and expertise to clinical practice. Presentations to nursing students and faculty might also help to reduce misconceptions regarding what nurses with physical disabilities can contribute to the workplace.
Applying Research to Practice
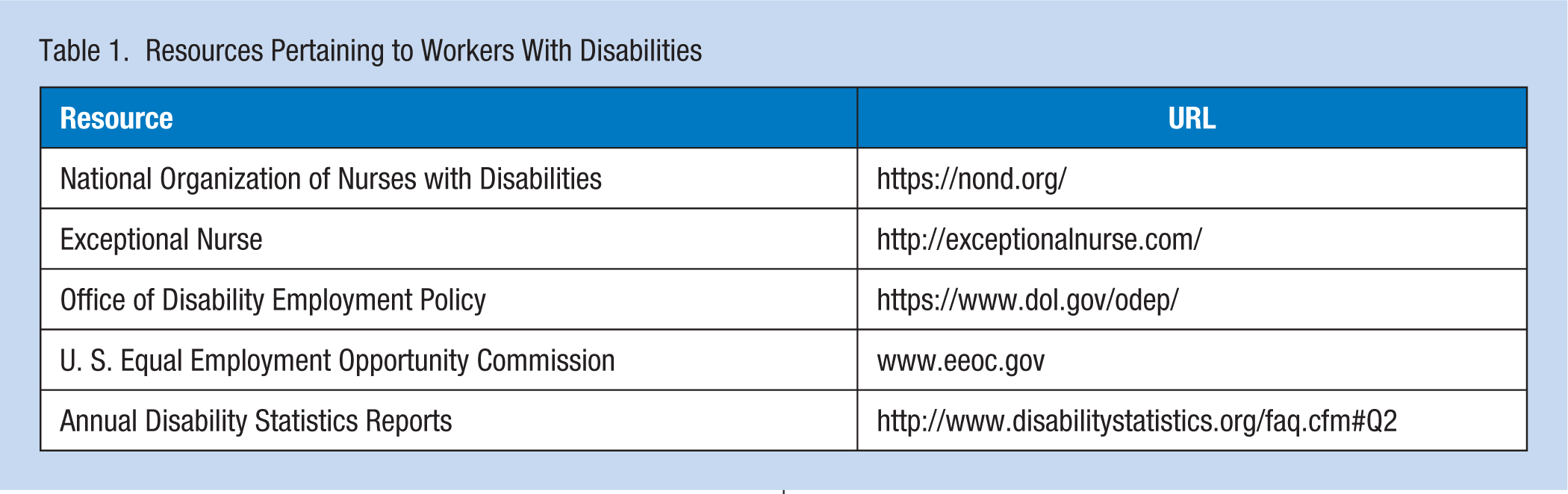
The results of this study and previous studies on nurses with disabilities align with national efforts to bring visibility to the experiences of nurses with disabilities. The National Organization of Nurses with Disabilities (NOND) and ExceptionalNurse.com are two national organizations supporting nurses with disabilities. The NOND and the Office of Disability Employment Policy (ODEP) formed an alliance to share expertise and promote awareness, disseminate information and resources (https://www.dol.gov/odep/alliances/nond.htm). In 2014, this author was invited to sit on a national policy roundtable held in Washington, D.C. The roundtable brought together interested organizations and groups working in disability arenas (Neal-Boylan, Marks, & McCulloh, 2015). The American Nurses Association (ANA; 2013) published a scope and standards document regarding nurses with intellectual and developmental disabilities. While nursing organizations typically include the word disability in their policy statements on diversity, they have, thus far, given relatively little visibility to the issue of nurses with disabilities and the discrimination they frequently face.
Occupational health nurses can use the results of this study and other studies on nurses with disabilities to help increase awareness and educate nurses and other health professionals and managers to recognize that a physical disability does not necessarily impair the nurse’s ability to provide safe or competent care. The experience and expertise of the nurse can still be used to provide quality care, perhaps in a different role or in a different setting than prior to the acquisition of the disability. The occupational health nurse can help dispel misconceptions and recommend that staff and managers focus on the abilities of nurses and not make assumptions about what these nurses can do safely. Table 1 includes resources that pertain to nurses with disabilities. Occupational health nurses are encouraged to use these resources to inform themselves and others so, together, we can eliminate discriminatory practices in employment and retain nurses with disabilities in the profession.
Resources Pertaining to Workers With Disabilities
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Leslie J. Neal-Boylan is the associate dean of academic affairs and program innovation and professor of nursing at the MGH Institute of Health Professions in Boston, MA. She is a family nurse practitioner and has been studying nurses with disabilities, for eleven years.