
Abstract
Background
Provisions of reasonable workplace accommodations can support the retention of nurses and midwives with disabilities in their professional roles. However, many encounter barriers to accessing accommodations in their practice.
Purpose
This review aimed to map the existing knowledge and identify gaps in literature regarding workplace accommodations for nurses and midwives with disabilities.
Method and Procedures
The scoping review adhered to JBI methodology to identify available literature on workplace accommodations in nursing and midwifery practice. A search of CINAHL, SocINDEX, PsycInfo, PubMed, Web of Science, EMBASE, and ProQuest Dissertation identified 4160 articles. Data was extracted from 20 sources that met the eligibility criteria.
Results
Workplace accommodations that employers were both able and unable to provide, as well as informal accommodations made by the employee, were uncovered. Key barriers included unclear processes, experiences of ableism, and self-disclosure difficulties. Alternatively, access to accommodations was facilitated by supportive and collaborative managers and colleagues.
Discussion
Workplace accommodations were found to contribute to nurses’ success, yet the implementation was not without challenges. Workforce barriers must be universally addressed to improve inclusion in nurses and midwifery practice. A significant gap in research regarding accommodations in midwifery was found. Further research on strategies to promote accessibility in nursing and midwifery internationally is needed, with focus on Canada where literature was limited.
Conclusion
Effective provision of workplace accommodations requires clear policies, processes, and communication, which is currently lacking. A streamlined process would help to reduce absenteeism and retain nurses and midwives with disabilities.
Background and Purpose
A global nursing and midwifery shortage has been declared which has led to increased focus on their recruitment and retention (Ferguson, 2024; Nove et al., 2021). One proposed strategy to address this issue centers on enhancing recruitment and retention initiatives for health professionals who experience disabilities (Calloway & Copeland, 2021). However, a scoping review by Baker et al. (2023) found that nurses and midwives with disabilities may leave the profession due to persistent symptoms, negative work environments, and a lack of workplace accommodations. Workplace accommodations involve any change in the work environment or terms of employment that enables individuals with disabilities opportunities to perform their job (Canadian Association for Supported Employment, 2024). The purpose of an accommodation is to reduce or eliminate barriers for people with disabilities (Dubsky, 2017). Employees with accommodations must continue to demonstrate that they are qualified to perform the essential requirements of the job (Neal-Boylan & Miller, 2015).
Legislation is in place throughout most of the world to protect the rights of people with disabilities. Legislation requires that employers make reasonable accommodation to support continued employment of people with disabilities (Government of Canada, 1985; Matt et al., 2015). In Canada, the duty to accommodate is identified in the Canadian Human Rights Act (Government of Canada, 1985). This legislation mandates employers to adjust working conditions to promote inclusion of people with disabilities in the workplace (Government of Canada, 1985). Despite legislation, health professionals have reported difficulty accessing accommodations in their professional practice (Lindsay et al., 2023; Neal-Boylan & Miller, 2015; Thomson & Winsor Murray, 2023).
Misinformation regarding workplace accommodations is frequently noted in the literature. First and foremost, accommodations are often viewed as a form of favoritism that places employees at an unfair advantage to that of their colleagues (Syma, 2019). This misconception leads to a sense of mistrust from managers and colleagues towards those who receive accommodations (Bosma et al., 2021). Accommodations provide employees opportunities to complete the essential duties required of the job, rather than place them at an unfair advantage (De Asís Roig, 2016). In addition, accommodations should not cause undue hardship on the employer such as implementing shared positions or resulting in unreasonable financial burdens (De Asís Roig, 2016; Neal-Boylan & Miller, 2015).
Accessing accommodations requires a collaborative approach, though the employee is responsible for initiating the process (Neal-Boylan & Miller, 2015). However, due to experiences of stigma and discrimination (also known as ableism), many individuals hesitate to disclose a disability, which prevents them from receiving necessary accommodations required to perform their job (Bogart & Dunn, 2019; McKinney & Swartz, 2021). In a review of legal cases involving nurses with disabilities in the United States, 84% of the cases examined involved allegations of workplace discrimination (Neal-Boylan & Miller, 2015). Therefore, many individuals wait until the situation is urgent prior to engaging in self-disclosure and seeking support (Bogart & Dunn, 2019). Delaying disclosure leads to negative effects on well-being, issues with work performance, and increased rates of absenteeism for nurses and midwives with disabilities (Baker et al., 2023; Santuzzi et al., 2019).
Misconceptions and misinformation surrounding nurses and midwives with disabilities and accommodation practices contribute to the persistence of ableist attitudes in healthcare. One way to address ableism is by enhancing information and education surrounding disabilities (Calloway & Copeland, 2021) and associated legislation. Therefore, a greater understanding of workplace accommodations for nurses and midwives is needed to dispel misconceptions and better support their continued employment (Baker et al., 2023; Lindsay et al., 2023).
A comprehensive understanding of the situation is the first step required to enhance workplace accessibility and inclusion. Therefore, a scoping review was conducted to better understand workplace accommodation practices for nurses and midwives with disabilities. No reviews specific to accommodations in nursing and/or midwifery practice were found in CINAHL, PubMed, Open Science Framework, and the JBI Systematic Review Register. Many available reviews focused on student and faculty experiences within nursing education (Epstein et al., 2021; Horkey, 2019; L’Ecuyer, 2019; Pezaro et al., 2020). Furthermore, Baker et al. (2023) completed a scoping review focused on the experiences of nurses and midwives with disabilities and found that little is known regarding accommodations in the workplace. A comprehensive understanding of workplace accommodation practices for nurses and midwives with disabilities is lacking, both nationally and internationally, as no reviews were located on this topic, indicating a research gap.
This review aimed to map the existing knowledge and identify gaps in literature regarding workplace accommodations for nurses and midwives with disabilities. A scoping review was conducted to answer: What literature exists regarding workplace accommodations for nurses and midwives who experience disabilities? For the study, disability was defined as an interaction between individuals with a temporary or permanent health condition and personal and environmental factors such as inaccessible structures and negative attitudes (World Health Organization, 2025).
Methods and Procedures
Since the breadth and scope of current evidence on this topic is unknown, a scoping review was selected over a systematic review for this project. The scoping review adhered to JBI methodology and ethical standards outlined by Peters et al. (2015, 2020). The objectives of the study were to: 1) To map the literature on workplace accommodations for nurses and midwives with disabilities, 2) examine organizational processes related to workplace accommodation, and 3) identify knowledge gaps to inform future research.
Eligibility Criteria
The population of interest was nurses, specifically licensed practical nurses, registered nurses, psychiatric/mental health nurses, nurse practitioners, and other advanced practice nurses, and midwives who experience disabilities employed in healthcare settings. Personal support workers and other unregulated care providers were not included, as they do not align with the scope of nursing/midwifery practice.
The concept of interest was workplace accommodations. For this study, accommodations were defined as “any change in the work environment or the terms and conditions of employment that allows a person with limitations in their abilities, or who faces barriers from the standard rules and conditions of work, to perform their job (Canadian Association for Supported Employment, 2024, para. 4). This definition encompasses modifications to both work activities, such as reduced lifting requirements, as well as work expectations such as scheduling changes. Assistive devices (such as use of an amplified stethoscope) may be provided as a type of accommodations to help a person to perform a particular task (Canadian Institutes of Health Research, 2023; World Health Organization, 2010). Therefore, assistive devices required as an accommodation in nursing and midwifery practice were also included.
All healthcare settings that employ nurses and midwives were eligible for inclusion. This encompassed hospitals, long-term care homes, primary care clinics, community health centers, public health units, and home care services.
The scoping review included published sources of evidence such as qualitative, quantitative, and mixed method studies (including dissertations and theses), and reviews. When published sources provided information on a variety of populations and concepts, the article was included if at least 50% of the content focused on accommodations in nursing and/or midwifery. Articles that described programs that were used as an alternative to disciplinary action related to substance use disorders were excluded from the review. Studies focused entirely on gradual return to work programs and workplace injury prevention were also excluded from the review. No time limit was set given that this is the first scoping review on this topic. Translation software (DeepL Translator) was used to review full-text articles written in languages other than English. The protocol was registered with Open Science Framework (https://osf.io/ygpn4/overview).
Search Strategy
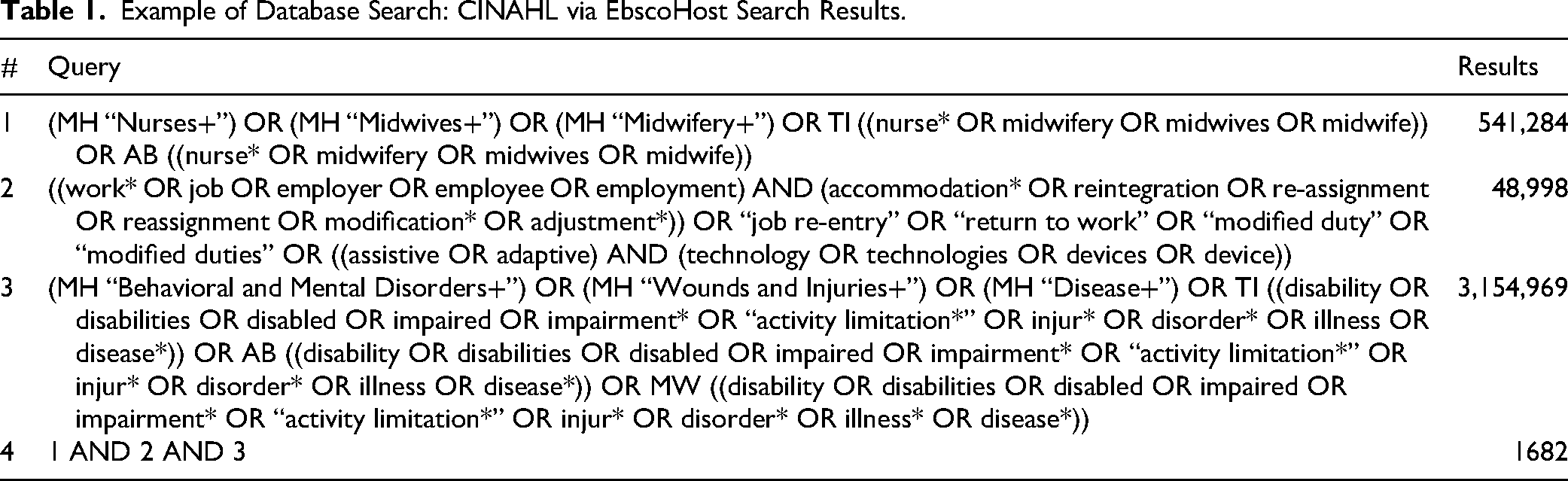
Two academic librarians collaborated with the review team to conduct an extensive literature search to locate relevant published sources of evidence regarding the population, concept, and contexts identified following a three-step strategy (Aromataris et al., 2024; Peters et al., 2020). First, a preliminary keyword search was conducted in CINAHL and PubMed to identify articles on the topic. Search results were used to identify potential synonyms for each key concept. Then all keywords were compared to the controlled vocabulary in each database. Next, search strings were tailored to each database using both keywords and controlled vocabulary, where appropriate. In some cases, subject headings were exploded to include as many related topics as possible. Table 1 provides an overview of search terms used. Second, the full search was conducted in CINAHL, PubMed, SocINDEX, PsychInfo, Embase, Web of Science, and ProQuest Dissertation and Theses Global between February 28 and March 5, 2025. These databases were selected to provide comprehensive coverage of available sources related to the population, concept, and context of the review. Finally, citations and reference list of all included studies were screened for additional sources that met the criteria.
Example of Database Search: CINAHL via EbscoHost Search Results.
Review Strategy and Data Extraction
To ensure that all team members had a clear understanding of the review criteria, a pilot of the review strategy was conducted with 15 sample articles. The full search was conducted following the pilot. The search identified 5598 articles which were collated and uploaded into literature review software (Covidence), with 1438 duplicate records removed. Two independent reviewers screened all sources identified for titles and abstracts (n = 4160), followed by the full text review (n = 108). Disagreements that arose between the reviewers at any stage of the process were resolved by a third reviewer. The principal investigator served as the consistent reviewer and was involved in all stages of the review to enhance validity and reliability.
During the full-text review, several articles were excluded because they did not address accommodations (wrong concept; n = 47), did not focus on nursing or midwifery (wrong population; n = 8), were unrelated to healthcare settings (wrong context; n = 1), or were commentary pieces or conference abstracts (wrong source; n = 33). The results of the search have been presented in the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) flow diagram (Figure 1).
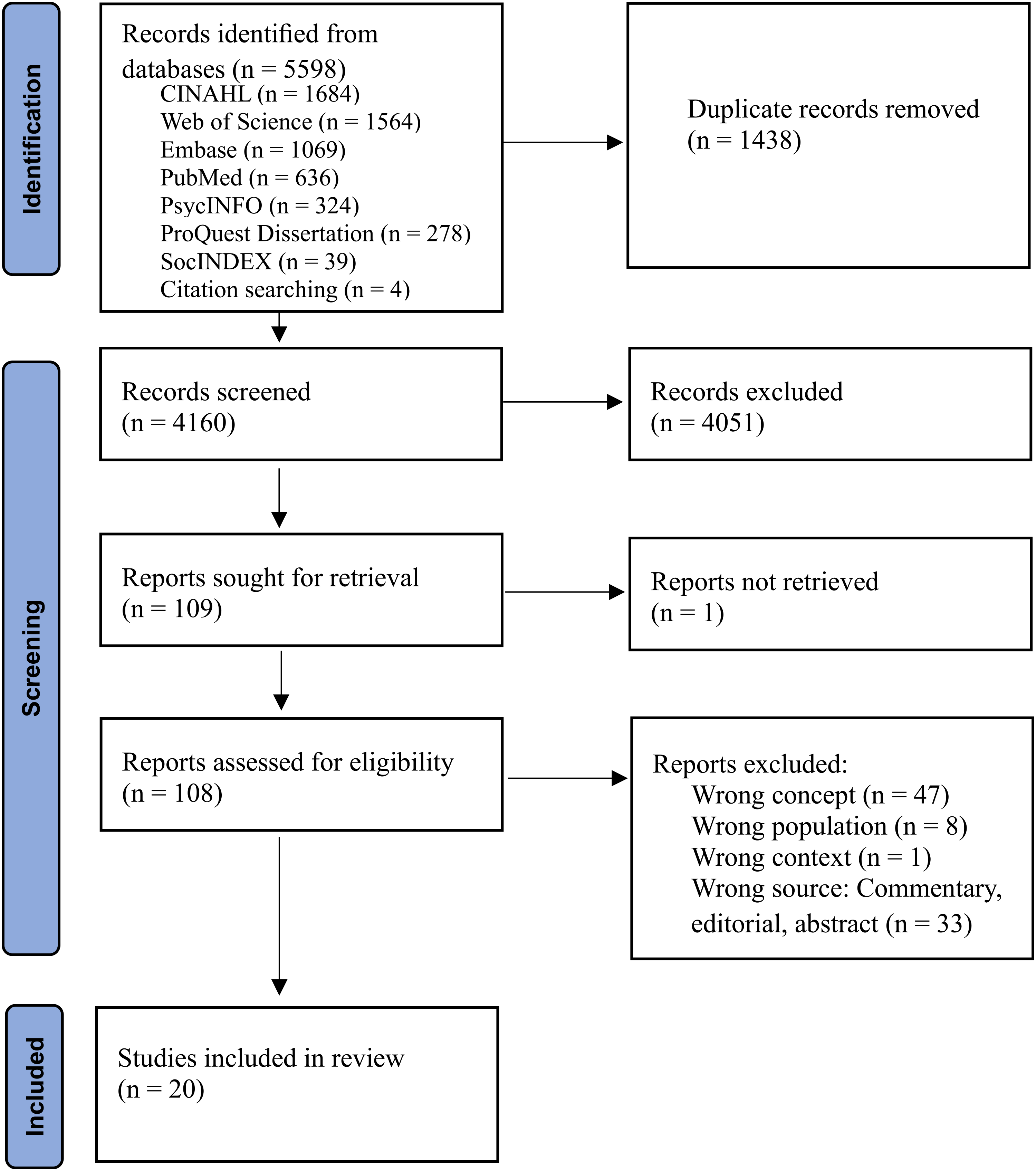
PRISMA-ScR flow chart.
Twenty published sources were included for data extraction. The data extraction instrument was created based on the JBI methodology guidelines outlined by Aromataris et al., (2024) and was piloted prior to finalizing. The data extracted included specific details about the population, concept, context, and research design to align with the research objectives. Two independent reviewers engaged in data extraction of the sources included and any disagreements were resolved by a third reviewer. Data were analyzed using descriptive analysis by quantifying text and conducting frequency counts (percentages) of extracted information (Peters et al., 2015, 2020) to summarize the findings, highlight common themes, identify knowledge gaps, and suggest areas for further research.
Results
Study Characteristics
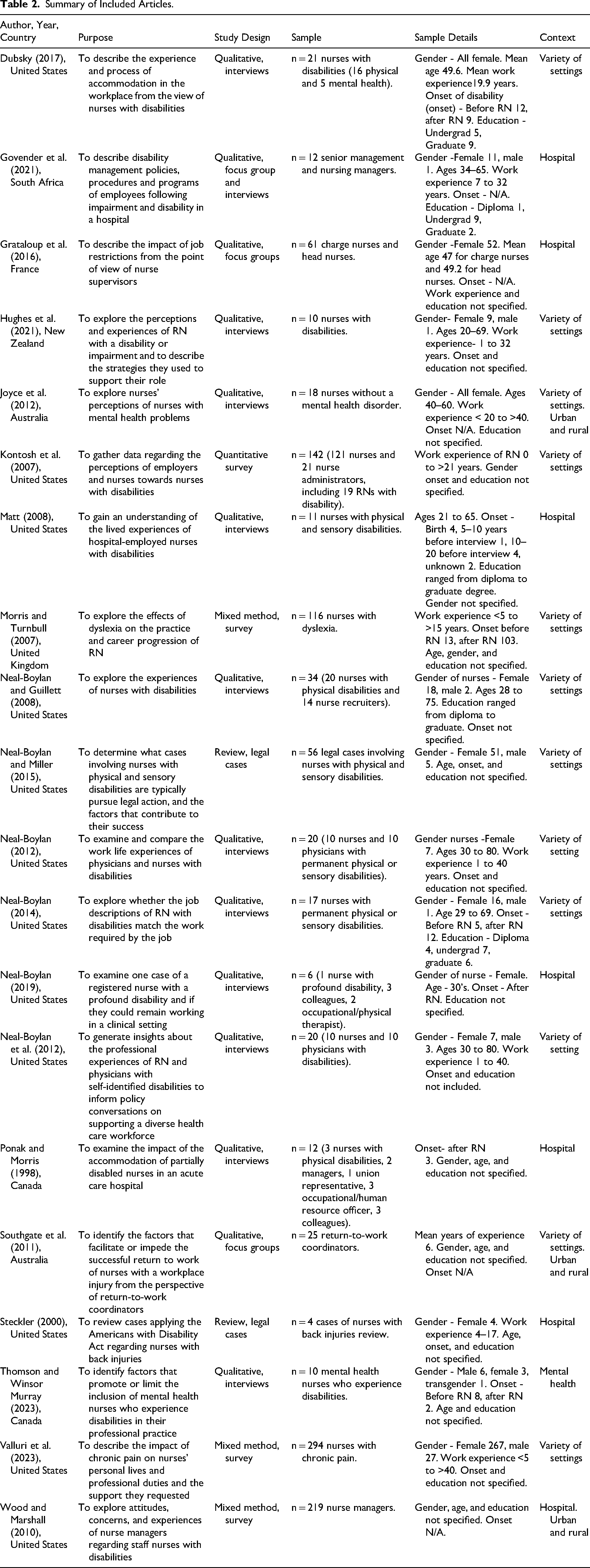
Data from 20 sources meeting the eligibility criteria were mapped, charted, and summarized. Publication dates of included articles ranged from 1998 to 2023 with most studies published between 2006 and 2015 (n = 11, 55%). The most common method used was qualitative (n = 14, 70%), followed by mixed method (n = 3, 15%), legal case reviews (n = 2, 10%), and quantitative studies (n = 1, 5%). Over half of the studies used individual interviews for data collection (n = 11, 55%). In addition, surveys (n = 4, 20%), focus groups (n = 2, 10%), legal case review (n = 2, 10%), and a combination of focus groups and interviews (n = 1, 5%) were employed as data collection strategies. The majority of articles originated in the United States (n = 12, 60%), after that Australia (n = 2, 10%), Canada (n = 2, 10%), France (n = 1, 5%), New Zealand (n = 1, 5%), South Africa (n = 1, 5%), and the United Kingdom (n = 1, 5%). One included source was a dissertation (Dubsky, 2017). The remaining 19 sources were peer reviewed studies.
A few studies identified a conceptual framework in the study design. The Integrative Model of Health Care Working Conditions on Organizational Climate and Safety (IMHCWCO) (Neal-Boylan, 2012, 2014) and Constructivist foundation (Neal-Boylan, 2019) were utilized. The IMHCWCO approach centered on improving organizational conditions for employees and patients in healthcare (Neal-Boylan, 2012, 2014). Whereas the Constructivist approach centers on the unique experiences and perspectives of participants, rather than relying solely on generalized interpretations, it emphasizes understanding meaning within the context of individuals lived experiences (Cleland & Durning, 2015; Neal-Boylan, 2019). In addition, Matt (2008) derived the Nurse First Model from the results of a grounded theory study to describe work experiences of nurses with disabilities.
Seventy percent of the studies focused solely on Registered Nurses (n = 14, 70%). In addition to Registered Nurses, Advanced Practice Nurses (n = 3, 15%), Mental Health Nurses (n = 2, 10%), and Nursing Assistants (n = 1, 5%) were also included as the focus of various studies. Nurses with disabilities comprised the most common sample group (n = 11, 55%), with two of these studies also including physicians with disabilities. Managers and return-to-work coordinators made up the sample of four studies (20%). Additionally, two studies included both nurses with disabilities and managers (10%). Another two encompassed a variety of participants such as nurses with disabilities, colleagues, managers, and occupational health professionals (10%). One study was from the perspective of nurse colleagues (5%). Notably, none of the studies included in the review explored workplace accommodations in midwifery practice.
Over half of the studies focused on a variety of settings such as hospital, long-term care, and community-based healthcare (n = 12, 60%). Seven studies focused solely on hospitals (35%), and one was specific to mental health care (5%). In addition, three studies included both rural and urban locations (15%). See Table 2 for additional details on the study characteristics.
Summary of Included Articles.
Definitions and Descriptions of Disability
Overall, there was consistency in the definition of disability used within the studies. Disability was often described as activity limitations, functional impairments (Dubsky, 2017; Grataloup et al., 2016; Matt, 2008; Neal-Boylan, 2012, 2014, 2019; Neal-Boylan & Guillett, 2008; Neal-Boylan & Miller, 2015; Ponak & Morris, 1998; Southgate et al., 2011; Steckler, 2000; Thomson & Winsor Murray, 2023; Valluri et al., 2023), or changes in behavior (Joyce et al., 2012). Additionally, authors noted that disability was formally documented or recorded (Dubsky, 2017; Neal-Boylan & Miller, 2015; Wood & Marshall, 2010). Disability was also described as chronic or reoccurring (Neal-Boylan, 2012, 2014; Neal-Boylan et al., 2012; Valluri et al., 2023), however, Thomson and Winsor Murray (2023) noted that a disability may also be temporary or episodic in nature.
In the case that authors did not provide a definition of disability, five authors listed the diagnoses of the participants included in the sample (Hughes et al., 2021; Matt, 2008; Neal-Boylan, 2014; Neal-Boylan & Guillett, 2008; Ponak & Morris, 1998) or provided a description of the disabilities experienced (Morris & Turnbull, 2007; Neal-Boylan, 2019). The most common type of disability researched was physical in nature (n = 13, 65%) (Dubsky, 2017; Grataloup et al., 2016; Matt, 2008; Neal-Boylan, 2012, 2019; Neal-Boylan & Guillett, 2008; Neal-Boylan & Miller, 2015; Ponak & Morris, 1998; Southgate et al., 2011; Steckler, 2000; Thomson & Winsor Murray, 2023; Valluri et al., 2023), followed by mental health (n = 3, 15%) (Dubsky, 2017; Joyce et al., 2012; Thomson & Winsor Murray, 2023), sensory disabilities (n = 3, 15%) (Matt, 2008; Neal-Boylan, 2012, 2014; Neal-Boylan & Miller, 2015), and dyslexia (n = 1, 5%) (Morris & Turnbull, 2007). Other authors addressed disability in nursing practice more broadly, without identifying or specifying diagnoses or conditions (Govender et al., 2021; Hughes et al., 2021; Neal-Boylan et al., 2021; Wood & Marshall, 2010).
Definitions and Descriptions of Accommodations
Most studies did not include a definition of workplace accommodations. Of the seven studies that provided definitions, common descriptions included workplace modification, adjustments, or assistance such as modified environments and duties, access to equipment and technology, and adjusted work schedules (Dubsky, 2017; Govender et al., 2021; Grataloup et al., 2016; Hughes et al., 2021; Thomson & Winsor Murray, 2023; Valluri et al., 2023; Wood & Marshall, 2010). The purpose of accommodations was described as providing individuals with disabilities opportunities to perform the essential workplace duties and benefit from ongoing employment (Dubsky, 2017; Govender et al., 2021; Valluri et al., 2023). Wood and Marshall (2010) noted that accommodations may be temporary or permanent modifications. The concept of undue hardship was used to explain when accommodations are deemed unreasonable (Dubsky, 2017; Neal-Boylan & Miller, 2015; Steckler, 2000). In one study, the Americans with Disabilities Act was utilized for the basis of the accommodation definition (Dubsky, 2017).
Summary of Workplace Accommodations
The formal workplace accommodations described by the studies included being reassigned to alternative positions (n = 8, 40%) (Dubsky, 2017; Grataloup et al., 2016; Neal-Boylan, 2019; Neal-Boylan & Guillett, 2008; Neal-Boylan & Miller, 2015; Ponak & Morris, 1998; Thomson & Winsor Murray, 2023; Wood & Marshall, 2010), scheduling changes (reduced hours or reduced night shifts) (n = 6, 30%) (Grataloup et al., 2016; Neal-Boylan & Guillett, 2008; Ponak & Morris, 1998; Southgate et al., 2011; Valluri et al., 2023; Wood & Marshall, 2010), modified duties and/or adjusted job descriptions (n = 4, 20%) (Neal-Boylan & Guillett, 2008; Ponak & Morris, 1998; Southgate et al., 2011; Wood & Marshall, 2010), ergonomic workstations (sit-stand desks and/or stationary chairs) (n = 3, 15%) (Matt, 2008; Thomson & Winsor Murray, 2023; Valluri et al., 2023), reduced lifting requirements (n = 3, 15%) (Dubsky, 2017; Southgate et al., 2011; Wood & Marshall, 2010), protected time to attend medical appointments (n = 2, 10%) (Joyce et al., 2012; Thomson & Winsor Murray, 2023), increased or regular breaks (n = 2, 10%) (Thomson & Winsor Murray, 2023; Valluri et al., 2023), the ability to audio record reports and document in a private location (n = 1, 5%) (Dubsky, 2017), travel restrictions (n = 1, 5%), and no overtime hours (n = 1, 5%) (Thomson & Winsor Murray, 2023). Assistive devices provided by the employer were discussed in three distinct categories including audiology devices/technology (amplified stethoscopes, amplified phones, microphones, vibrating beepers, captioning) (n = 3, 15%) (Dubsky, 2017; Matt, 2008; Wood & Marshall, 2010), visual devices/technology (magnifying devices, larger computer monitors) (n = 3, 15%) (Dubsky, 2017; Govender et al., 2021; Wood & Marshall, 2010), along with devices for lifting patients and moving equipment (n = 2, 10%) (Valluri et al., 2023; Wood & Marshall, 2010).
Engaging self-accommodation was the most common type of accommodation uncovered, as half of all studies included descriptions of this concept (n = 10, 50%) (Dubsky, 2017; Hughes et al., 2021; Matt, 2008; Morris & Turnbull, 2007; Neal-Boylan, 2012, 2014; Neal-Boylan et al., 2012; Neal-Boylan & Guillett, 2008; Thomson & Winsor Murray, 2023; Wood & Marshall, 2010). Self-accommodation was described as an informal process where there was no written or verbal consent from employers to implement changes to their practice and/or the environment (Dubsky, 2017). Examples of self-accommodation included learning new ways to complete tasks, modifying the environment on their own, and purchasing own assistive devices (Dubsky, 2017; Hughes et al., 2021; Matt, 2008; Morris & Turnbull, 2007).
In addition, authors noted types of accommodations that some employers were unable or unwilling to provide. Four studies (20%) found that reduced lifting requirements or an inability to perform cardiopulmonary resuscitation impinged on the essential requirements of the job and, therefore, were deemed unreasonable based on legislation (Dubsky, 2017; Neal-Boylan, 2014; Steckler, 2000; Thomson & Winsor Murray, 2023). Modifications to environments to promote wheelchair accessibility for nurses with disabilities such as increased space at the patient bedside were deemed not possible in three studies (15%) (Dubsky, 2017; Govender et al., 2021; Neal-Boylan et al., 2012). Figure 2 provides a summary of accommodations identified in the scoping review.
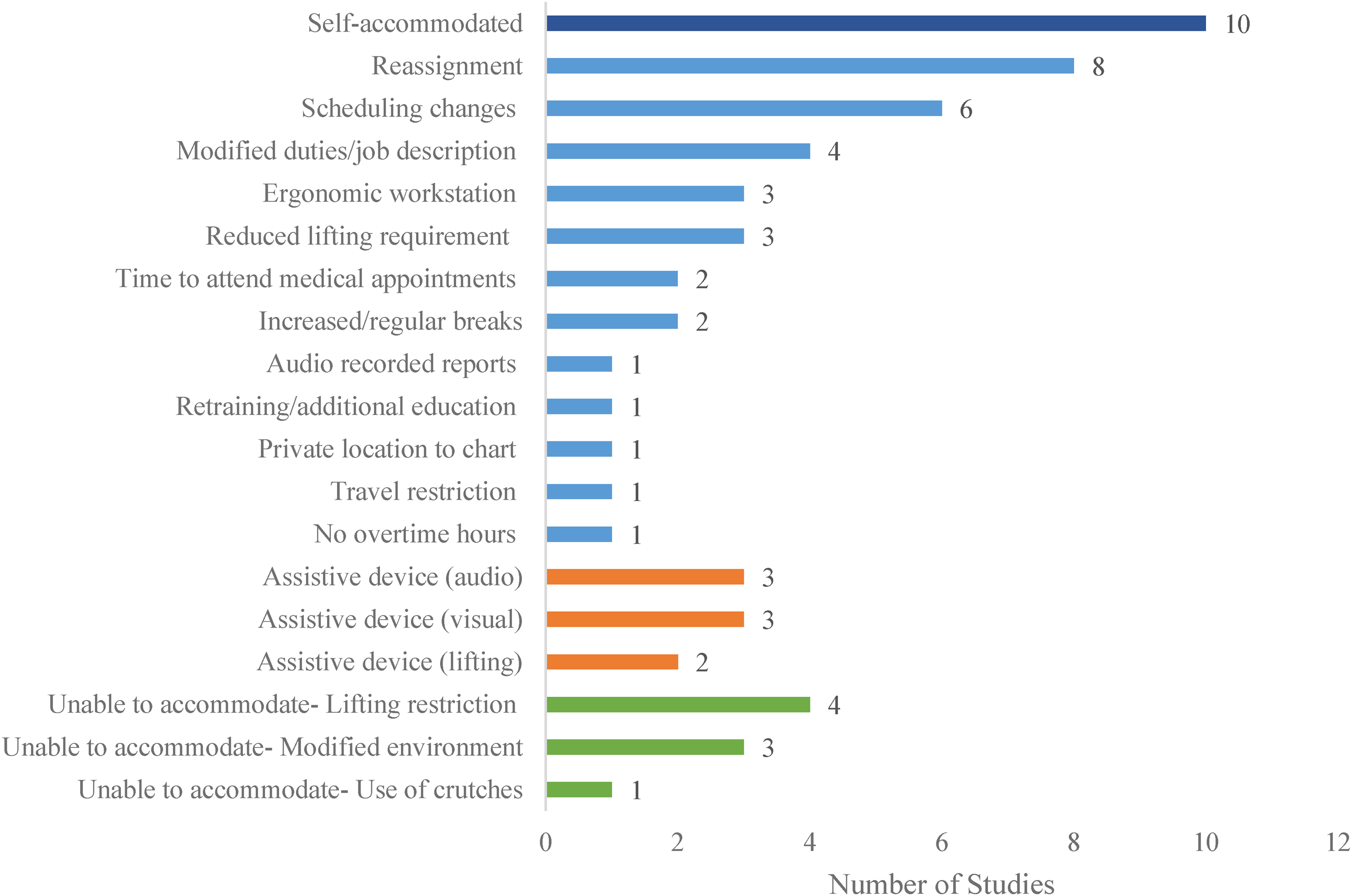
Accommodations and assistive device summary.
Barriers and Facilitators to Workplace Accommodations
There were six categories recognized as barriers to accessing workplace accommodations. The barriers noted by nurses with disabilities, as well as nurse managers, to accessing workplace accommodations were unclear processes to request and receive accommodations (n = 9, 45%) (Dubsky, 2017; Govender et al., 2021; Hughes et al., 2021; Kontosh et al., 2007; Neal-Boylan, 2014; Neal-Boylan et al., 2012; Neal-Boylan & Guillett, 2008; Ponak & Morris, 1998; Thomson & Winsor Murray, 2023), limited availability of accommodations and resources (n = 8, 40%) (Govender et al., 2021; Grataloup et al., 2016; Hughes et al., 2021; Joyce et al., 2012; Morris & Turnbull, 2007; Neal-Boylan, 2012; Neal-Boylan & Guillett, 2008; Thomson & Winsor Murray, 2023), and experiences of ableism or fear of ableism (n = 8, 40%) (Dubsky, 2017; Govender et al., 2021; Hughes et al., 2021; Matt, 2008; Morris & Turnbull, 2007; Neal-Boylan, 2014; Neal-Boylan & Guillett, 2008; Neal-Boylan & Miller, 2015). Additionally, reluctance to engage in disability self-disclosure to access accommodations (n = 7, 25%) (Dubsky, 2017; Hughes et al., 2021; Matt, 2008; Morris & Turnbull, 2007; Neal-Boylan, 2012; Neal-Boylan et al., 2012; Thomson & Winsor Murray, 2023) and a lack of awareness of workplace accommodations and disability rights (n = 3, 15%) (Dubsky, 2017; Neal-Boylan & Miller, 2015; Thomson & Winsor Murray, 2023) were noted.
Management also acted as a barrier as several studies highlighted that an unsupportive manager created challenges in accessing supports (n = 6, 30%) (Dubsky, 2017; Morris & Turnbull, 2007; Neal-Boylan, 2012; Neal-Boylan et al., 2012; Thomson & Winsor Murray, 2023; Valluri et al., 2023). Alternatively, access to accommodations was facilitated by supportive and collaborative managers and colleagues (n = 10, 50%) (Dubsky, 2017; Matt, 2008; Morris & Turnbull, 2007; Neal-Boylan, 2012, 2014, 2019; Neal-Boylan et al., 2012; Ponak & Morris, 1998; Thomson & Winsor Murray, 2023; Valluri et al., 2023).
The Effect of Setting and Education
As most studies were conducted across a variety of healthcare settings (n = 12, 60%) it was difficult to analyze how the setting affected provision of workplace accommodations. However, Thomson and Winsor Murray (2023) found that community-based mental health settings were more accommodating than acute care settings. Yet Wood and Marshall (2010) noted that community-based care in rural settings was difficult to accommodate due to travel requirements. Conversely, compared to urban settings, rural locations were more likely to be creative with accommodations to retain nurses (Wood & Marshall, 2010).
Of interest is the findings of one study where the nurses’ level of education affected the employer's ability to provide accommodations. Southgate et al. (2011) found that nurses prepared with bachelor's degrees were more likely to be accommodated than those with diplomas or nursing assistants due to lifting requirements commonly associated with these roles. Similarly, authors noted that accommodating nurses without fixed schedules (casual nurses) and those temporarily assigned to multiple healthcare facilities (agency nurses) can be difficult as they frequently work across various locations with different employers (Wood & Marshall, 2010).
Discussion
Findings from the review offer insight into workplace accommodations provided and not provided in nursing practice and associated barriers. Unfortunately, no authors reported on accommodations in midwifery practice suggesting a significant gap in literature.
The need to self-accommodate was related to the multiple barriers identified in this review. Many nurses with disabilities modified tasks or environments without formal permission and waited until they experienced performance issues to initiate the process of requesting accommodations (Dubsky, 2017). In addition, the decision to delay disclosure is often related to unclear processes as well as ableist attitudes regarding health professionals with disabilities rather than a lack of awareness of disability related legislation (Baker et al., 2023; Bogart & Dunn, 2019; Hughes et al., 2021; Jain, 2020; Lindsay et al., 2023). Furthermore, authors noted that nurses with disabilities were reluctant to seek accommodations due to misconceptions that accommodations were unfair or represented favoritism (Hughes et al., 2021; Neal-Boylan, 2014; Neal-Boylan & Guillett, 2008).
Self-accommodation emerged as a response to multiple systemic barriers and was often viewed as the path of least resistance for nurses with disabilities to meet their immediate needs. This approach failed to address the underlying issues required to improve accessibility, which is problematic as the provision of workplace accommodations had a positive effect on nurses’ ability to provide care (Hughes et al., 2021; Neal-Boylan, 2019; Thomson & Winsor Murray, 2023) and may serve to improve retention (Govender et al., 2021; Matt et al., 2015; Neal-Boylan, 2012, 2014; Southgate et al., 2011). Findings indicated that delaying accommodation requests increased absenteeism rates among nurses by contributing to fatigue, job stress, and burnout, which impaired their ability to attend work consistently (Baker et al., 2023; Covell et al., 2020).
While workplace accommodations such as reassignment to an alternative position were commonly reported, their implementation was sometimes challenging. For example, reassignment to an alternative position was a commonly reported accommodation. However, reassignment may cause conflict between managers especially in areas with low staffing levels (Govender et al., 2021; Grataloup et al., 2016). In addition, reassignment may override a collective agreement, where a nurse with disability is provided with a position over a nurse with more seniority or experience, which may inadvertently reinforce false perspectives of favoritism and special treatment towards those accessing accommodations.
Light or modified duties were also noted as difficult to accommodate in nursing given the complex care needs of patients (Govender et al., 2021). Due to a strained healthcare system, nurses are often expected to work above and beyond their strengths and push their endurance (Dubsky, 2017; Jones et al., 2023; Neal-Boylan, 2014), therefore positions that allow for light duties are likely in short supply. In addition, Neal-Boylan (2014) found that nurses are often required to complete tasks outside of their job description making it difficult for the employer to offer accommodations.
The most frequently cited barrier uncovered centered on confusion regarding accommodation related processes and policies. This barrier was identified by nurses with disabilities and nurse managers (Dubsky, 2017; Govender et al., 2021; Hughes et al., 2021; Kontosh et al., 2007; Neal-Boylan, 2014; Neal-Boylan et al., 2012; Neal-Boylan & Guillett, 2008; Ponak & Morris, 1998; Thomson & Winsor Murray, 2023). Long waits, challenges with documentation requirements, unclear points of contact, and a lack of policy were reported (Dubsky, 2017; Govender et al., 2021; Hughes et al., 2021). Similarly, a scoping review by Jones et al. (2024) regarding nurses returning to work following an injury or substance use disorder also noted inadequate policies and processes. Therefore, a streamlined approach should be developed and made readily available to employees and managers (Dubsky, 2017).
Workplace policies and processes that outline roles and responsibilities of employees and employers are instrumental in delivering successful provision of workplace accommodations (Jones et al., 2024). Transparent communication and a willingness to collaborate among the employer, employee, human resource professionals, as well as the occupational health physician/nurse is also vital (Govender et al., 2021). Existing policies should be revised to make disability disclosure and accommodation requests straightforward and safe for employees (Santuzzi et al., 2019). Additionally, education on the legislative right to access workplace accommodations is needed (Baker et al., 2023; Neal-Boylan, 2012, 2014; Neal-Boylan & Miller, 2015). A streamlined approach would be cost effective at reducing absenteeism and staff shortages (Govender et al., 2021).
Supportive managers were recognized as key facilitators in ensuring the provision of accommodations (Baker et al., 2023; Thomson & Winsor Murray, 2023). Yet many managers were unaware or unprepared to support nurses with disabilities (Dubsky, 2017). Still, nurse managers reported that the performances of nurses with disabilities were exceptional (Kontosh et al., 2007) and greater exposure to employing nurses with disabilities increased managers’ willingness to hire them (Wood & Marshall, 2010).
Improving Accessibility
Workforce barriers must be addressed to improve accessibility and inclusion in nursing practice. Inaccessible workplace practices that lead to missing breaks and working overtime were described (Dubsky, 2017; Thomson & Winsor Murray, 2023). In addition, some environments had structural barriers that were inaccessible to nurses with disabilities (Dubsky, 2017; Govender et al., 2021; Neal-Boylan et al., 2012). Due to challenges encountered and a lack of accessibility nurses and midwives with disabilities often leave their jobs (Baker et al., 2023; Kontosh et al., 2007; Neal-Boylan, 2014) while others pursue additional education to find jobs that are less demanding (Dubsky, 2017; Govender et al., 2021; Neal-Boylan, 2012, 2014). Ultimately, unsupportive work environments contribute to experience of burnout, job dissatisfaction, and the desire to leave nursing (Levi et al., 2021).
Given the barriers encountered, reliance on workplace accommodations to support nurses with disabilities is problematic. Accommodation is a reactive approach to meeting an individual's needs, and once that individual leaves the position the accommodation is no longer in place to potentially support others (Bogart & Dunn, 2019). A proactive approach that promotes accessibility for all is required to decrease the need for individual accommodations (Marks & Sisirak, 2022; McDermott-Levy et al., 2018; Thomson & Winsor Murray, 2023). Universal design principles can be applied to workplaces by creating environments that are accessible, flexible, and inclusive for all workers (Doussard et al., 2024). In practice, this entails the proactive design of workspaces, equipment, and processes to address diverse needs and abilities, improving overall accessibility. Implementing universal principles creates environments that consider a wide range of individual needs and abilities, thereby lessening the need for accommodations while promoting equitable access (Doussard et al., 2024).
Examining the accommodations that are commonly required, as well as those that cannot be provided, offers insight into system barriers that should be universally addressed to improve access (Thomson & Winsor Murray, 2023). Modifications that can be made available to all nurses includes amplified phones, larger computer monitors, ergonomic workstations, recording devices, microphones, increased space in patient care areas, strategic placement of ramps, and the adjustment of difficult work schedules (Matt et al., 2015; Neal-Boylan et al., 2012; Neal-Boylan & Guillett, 2008). These modifications will provide benefits to nurses by creating more accessible and supportive work environments, which can ultimately lead to improved patient care outcomes (Marks & Sisirak, 2022; Matt et al., 2015). Health professionals with disabilities have the potential to improve patient care (Ailey et al., 2016; Jain, 2020; Lindsay et al., 2023; Thomson & Winsor Murray, 2023). Nurses with disabilities noted enhanced nursing skills including heightened awareness of patient safety (Hughes et al., 2021) and improved ability to provide empathetic care (Neal-Boylan, 2019; Neal-Boylan et al., 2012; Thomson & Winsor Murray, 2023).
Implications for Research
There is a significant gap in research on workplace accommodations specific to midwifery practice. Given this gap, research is needed to develop effective accommodation policies and procedures tailored to this specialty. Most of the literature focused on the perspectives of nurses with disabilities, therefore there is a need for increased research from the perspective of nurse managers. This is especially important given that managers’ roles and perspectives were described as both barriers and facilitators to workplace accommodations. In addition, research on those who experience mental health and sensory challenges is required as many studies focused on physical disabilities. Quantitative research should be employed to determine if implementation of accommodation policies and streamlined processes improves retention of nursing and midwives with disabilities with comparisons made based on practice setting. And finally, further research on strategies to promote accessibility for all in nursing and midwifery practice internationally is needed, with focus on Canada where existing studies are limited.
Limitations and Strengths
This is the first scoping review on this topic, filling a major gap in disability research. For this reason, there were no time and jurisdictional restrictions on the articles to be included in the review, which allowed for a comprehensive account of existing literature on an international scale. Piloting the search strategy, eligibility criteria, and data extraction tool enhanced reliability. In addition, having two team members screen sources and a third independent member resolve discrepancies at all stages improved inter-rater reliability. However, this review has several limitations. Although a comprehensive three-stage search strategy was undertaken, there is a possibility that some relevant articles were not included. Additionally, commentaries and editorials were excluded from the study, resulting in the exclusion of 33 sources. Therefore, certain perspectives may not be captured given this exclusion criterion. Furthermore, scoping reviews typically do not assess the quality of method or risk of bias of included studies, therefore, conclusions regarding the effectiveness of workplace accommodations for nurses and midwives with disabilities cannot be made.
Conclusion
Although workplaces should be universally accessible, this is not always the case, making accommodations essential, yet difficult to obtain (Bogart & Dunn, 2019). System transformation is needed to create accessible and inclusive workplaces that meet the needs of nurses and midwives (Ailey et al., 2016; Marks & Sisirak, 2022; Shen Hsiao et al., 2022; Thomson & Winsor Murray, 2023). Effective provision of workplace accommodations requires clear policies, processes, and communication, which are currently lacking. Offering a streamlined process would help to reduce absenteeism and retain nurses and midwives with disabilities.
Footnotes
Acknowledgments
None
Ethical Approval
Not applicable.
Author Contributions
Andrea Thomson was the principal investigator and served as the consistent reviewer in all stages of the review including data extraction. She led data analysis. Laura Van Mulligen, Joanne Winsor Murray, Jennifer Adair, and Savannah Torres-Salbach served as the second or third reviewer during all stages of the review and assisted with data extraction. Rainer Schira and Marian Ramage developed the search strategy and conducted the search. They also assisted with retrieving sources for full text review. Andrea Thomson drafted the manuscript, and all team members assisted with revisions.
Funding
The research was funded by the Faculty of Health Studies (FHS) & Centre for Critical Studies of Rural Mental Health (CCSRMH) Grant [#2611].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable.