
Abstract
For the past two decades, agricultural workers in regions of Central America have reported an epidemic of chronic kidney disease of undetermined etiology (CKDu) that is not associated with established risk factors of chronic kidney disease. Several hypotheses have emerged, but the etiology of CKDu remains elusive and controversial. The aim of this literature review was to describe the potential risk factors of CKDu in Mesoamerica and implications for the U.S. agricultural worker population. PubMed and CINAHL databases were searched for articles published between 2000 and 2018 that examined CKDu in Mesoamerica; 29 original studies were included in this review. CKDu is a multifactorial disease that is often asymptomatic with hallmark characteristics of elevated serum creatinine and blood urea nitrogen (BUN), low glomerular filtration rate, electrolyte abnormalities, and non-nephrotic proteinuria. Reducing the global prevalence of CKDu will require more robust studies on causal mechanisms and on interventions that can reduce morbidity and mortality in vulnerable populations.
Keywords
Introduction
Chronic kidney disease of unknown etiology (CKDu) presents as chronic kidney disease (CKD) without traditional risk factors such as diabetes, hypertension, cardiovascular disease, or older age at onset (Crowe et al., 2013). During the past 40 years, a global epidemic of CKDu has emerged among young male agricultural workers in regions of Mesoamerica (central Mexico, Belize, Guatemala, El Salvador, Honduras, Nicaragua, and northern Costa Rica), South Asia, and Eastern Europe (F. Gifford et al., 2016; Wesseling et al., 2015). With more than 20,000 documented deaths, the Pan American Health Organization (PAHO) called attention to this growing epidemic in 2013 (Pan American Health Organization, 2013).
There is a compelling, urgent need to investigate the factors associated with the development of CKDu, including biomarkers that might indicate early pathology, such as renal dysfunction. CKDu has not been reported in the United States (U.S.), but renal dysfunction in U.S. agricultural workers who have immigrated from Mesoamerica has been documented in studies of physiological responses to environmental heat (Horton, 2016; Mix et al., 2018; Moyce, Joseph, Tancredi, Mitchell, & Schenker, 2016). Renal dysfunction among agricultural workers in California’s Central Valley and in Florida suggests the potential of an emerging public health concern in the U.S. Agricultural workers in the U.S. and Mesoamerica have similar environmental and occupational exposures that are potentiated by social and economic factors, such as extreme poverty, which may obligate workers to labor in extreme and harsh conditions (Crowe et al., 2013; Horton, 2016; Jackson & Rosenberg, 2010; Wesseling, Aragon, Gonzalez, Weiss, Glaser, Bobadilla, et al., 2016). Workers are also vulnerable due to lack of regulations to protect workers from occupational heat exposure. In Costa Rica and the U.S. states (California and Washington) where regulations do exist, workers exhibit kidney dysfunction and heat-related illness symptoms (Crowe, Nilsson, Kjellstrom, & Wesseling, 2015; Moyce et al., 2016) which may suggest a lack of enforcement. This article reviews the CKDu epidemic in Mesoamerica, clinical characteristics of it, proposed hypotheses for the CKDu epidemic, and provides implications for occupational health nursing research and practice.
Method
The databases PubMed and CINAHL were searched for published studies from 2000 to 2018 conducted in Mesoamerica examining CKDu. Primary search terms were “chronic kidney disease of unknown etiology,” “Mesoamerican nephropathy,” “agricultural nephropathy,” “CKDu,” and “Mesoamerica.” Articles were considered relevant and included in the review if they (a) evaluated CKDu in agricultural workers, (b) were conducted in Mesoamerica, and (c) were published in English.
Results
Twenty-nine articles were found that met the inclusion criteria. The types of studies were classified as descriptive clinical features (n =4), data-based epidemiological studies (n = 4), a case–control study (n = 1), longitudinal studies (n = 5), cross-sectional studies (n = 12), a qualitative study (n = 1), and intervention studies (n = 2). The following sections describe the main topics in the papers located in this search.
Clinical Features of CKDu
A cross-sectional study in El Salvador of 205 patients was the first published study to observe 67% of the patients with end-stage renal disease (ESRD) who did not have the traditional known risk factors for developing CKD and ESRD and were predominately young male agricultural workers (Trabanino, Aguilar, Silva, Mercado, & Merino, 2002). Since then, multiple studies have been conducted, but there is still an uncertainty on the natural progression of CKDu. The majority of the studies examined workers or communities at risk and very few on the pathophysiology of CKDu. Currently, a consistent case definition for CKDu does not exist, but the review of the literature revealed that the following factors are being used to indicate renal dysfunction in study populations without traditional risk factors of CKD: serum creatinine (SCr) >1.2 mg/dL or an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 (Peraza et al., 2012; Raines et al., 2014; Sanoff et al., 2010; Torres et al., 2010) or an eGFR <60 mL/min/1.73 m2 after 3 months (Orantes et al., 2011; Orantes et al., 2014). Cross-shift and across harvest studies used the Kidney Disease Improving Global Outcomes (KDIGO) criteria for acute kidney injury (AKI), a risk factor for CKD: elevated SCr (development of AKI increased ≥0.3 mg/dL or ≥1.5-fold from baseline); eGFR below 60 mL/min/1.73 m2 at more than one time point showing chronicity (Garcia-Trabanino et al., 2015; F. J. Gifford, Gifford, Eddleston, & Dhaun, 2017; Khwaja, 2012). In addition to trace proteinuria, hypokalemia, hyponatremia, and hyperuricemia, no established risk factors of CKD presented prior to the onset of disease (Kupferman et al., 2016; Laws et al., 2016). Clinical diagnosis may include ultrasounds showing small echogenic kidneys (Herrera et al., 2014) and kidney biopsy samples indicate glomerular lesions and tubulointerstitial damage, suggesting chronic ischemia and mild vascular changes not consistent with other common renal diseases (Lopez-Marin et al., 2014; Wijkstrom et al., 2013). In one study, an increase in the renal biomarkers of tubular damage in AKI was also present in those with CKDu (Laws et al., 2016). Biomarkers observed in this study included albumin–creatinine ratio (ACR), neutrophil gelatinase-associated lipocalin (NGAL), N-acetyl-
Without a consistent case definition of CKDu, it was not possible to compare the incidence across different populations, and the ability to examine etiological factors was limited. Due to this limitation, recently, the Disadvantaged Populations eGFR Epidemiology (DEGREE) protocol initiative has called for standardization of SCr measurements, storage of cystatin C, body composition measurements, and self-reported meat consumption which fosters comparison of findings across studies conducted in different countries (Caplin et al., 2017).
Etiologic Hypotheses for CKDu
Although there is not a widely accepted case definition for CKDu, there are many etiologic hypotheses including heat stress and volume depletion, agrochemical exposure, nephrotoxicity, and infection, which may interact with host factors including genetics and socioeconomic status.
Heat Stress, Dehydration, and Volume Depletion
A mechanism for CKDu proposed by several researchers is that occupational heat stress leads to chronic dehydration, which disrupts kidney function (Carl-Gustaf, Wernerson, & Wijkstrom, 2015; Correa-Rotter, Wesseling, & Johnson, 2014). Strenuous occupational work in environments with high ambient temperatures has been commonly reported, where dehydration was common (Garcia-Trabanino et al., 2015; Wesseling, Aragon, Gonzalez, Weiss, Glaser, Bobadilla, et al., 2016; Wesseling, Aragon, Gonzalez, Weiss, Glaser, Rivard, et al., 2016). Studies observed that workers lost up to 2.5 kg during single work shifts with urine-specific gravity (USG) measurements at the end of work shifts that indicated dehydration (Garcia-Trabanino et al., 2015). Decreased kidney function was more often observed in regions with high ambient temperatures, such as coastal communities, than in high-altitude communities (Laux, Barnoya, Guerrero, & Rothstein, 2015; Peraza et al., 2012; Torres et al., 2010; Wesseling et al., 2015). Studies have observed, across a harvest season, a reduction in eGFR and SCr at the beginning and end of a harvest season, and an increase in acute renal injury biomarkers at the end of the season (Laws et al., 2015, 2016; Wesseling, Aragon, Gonzalez, Weiss, Glaser, Bobadilla, et al., 2016). These findings suggest that occupational heat stress and recurrent dehydration may be associated with the development of CKDu. There was consensus during the first and second International Research Workshops on CKDu that repeated episodes of dehydration during heavy work in hot climates, with loss of electrolytes accompanied by AKI, may be a significant contributing factor to the CKDu epidemic (Wesseling et al., 2014). However, it is noteworthy that chronic dehydration has not been recognized as a cause of CKD, but rather a known contributing factor to AKI. Consensus in the medical literature indicates that hospitalized patients who suffer from AKI due to dehydration fully recover renal function after an acute event (National Health Service, 2016). There is no strong evidence to date that repeated episodes of AKI are part of the natural history of CKDu and recovery from AKI episodes eventually diminishes and leads to permanent renal disease. Only one paper focused on patients diagnosed with CKDu and potential risk factors (VanDervort, Lopez, Orantes, & Rodriguez, 2014). In reviewing medical records and place of residence, this ecological study reported no association between patients hospitalized with CKDu and ESRD and ambient temperatures in areas of residence.
A study among 117 agricultural workers in Nicaragua hypothesized that consuming high-fructose drinks and chewing sugarcane during strenuous work activity were etiological risk factors for the development of CKDu (Raines et al., 2014). The researchers suggested that excessive intake of fructose may exacerbate kidney injury via the fructokinase pathway. However, there have been no human studies documenting a relationship between ingestion of high-fructose beverages and the development of CKDu. A rodent study has shown that repeated dehydration leads to fructokinase activity, which results in tubular injury from the generation of endogenous fructose via the polyol pathway (Roncal Jimenez et al., 2014). This suggests that excessive intake of fructose beverages may exacerbate kidney injury; however, further research is warranted to translate these findings to human populations.
Agrochemical Exposure
Agrochemicals such as pesticides and fertilizers have been postulated as risk factors for CKDu (Jayasumana et al., 2017; O’Donnell et al., 2011; Orantes et al., 2014; Raines et al., 2014). Agricultural workers are exposed to agrochemicals through ingestion, inhalation, and dermal contact of pesticides and fertilizers that are applied at the worksite. However, in a longitudinal cohort study in Nicaragua, agrochemical applicators did not have a significant increase in renal injury biomarkers (Laws et al., 2016). A cross-sectional study in Nicaragua among small-scale farmers, construction workers, and sugarcane cutters did not observe an association between pesticides and biomarkers of kidney function (Wesseling, Aragon, Gonzalez, Weiss, Glaser, Rivard, et al., 2016). An ecological study of patients in El Salvador with CKDu conducted by VanDervort et al. (2014) postulated that the disease might arise from proximity to agricultural fields to which agrochemicals had been applied. However, a systematic review found no significant association between pesticides and CKDu (Gonzalez-Quiroz, Pearce, Caplin, & Nitsch, 2018). To date, there have been no studies in Mesoamerica examining biomarkers of agrochemical exposure; only self-reports of work practices and history have been obtained through questionnaires.
While pesticide exposure has been frequently reported in agricultural workers, kidney damage has also been reported in case studies of females and adolescents who had no prior agricultural work history (Ramirez-Rubio et al., 2016). If agrochemicals contribute to CKDu, nonworker exposure to agrochemicals through ingestion, inhalation, or dermal contact within the same living environment as workers may also contribute to kidney damage.
Nephrotoxin Exposure
Exposure to heavy metals and certain medications can be toxic to the kidneys. A study in Western Nicaragua found lead, cadmium, arsenic, and uranium in soil and water, but at nontoxic levels and not specifically in the areas where CKDu is prevalent (McClean et al., 2012). Other studies from Nicaragua reported that a locally produced form of alcohol was prepared and stored in industrial metal containers and that this may have exposed agricultural workers who drank the alcohol to lead, cadmium, or other heavy metals that are nephrotoxic; however, the study did not identify specific nephrotoxic agents that were present (Lebov et al., 2015; Sanoff et al., 2010).
Chronic consumption of nonsteroidal anti-inflammatory drugs (NSAIDs) and aminoglycoside antibiotics has also been shown to be a risk factor of CKDu (Wesseling et al., 2014). Agricultural workers are engaged in strenuous work that can cause workplace injuries, musculoskeletal disorders, and resulting pain. These workers may alleviate their symptoms with NSAIDs (Herrera et al., 2014; Orantes et al., 2011). Another common symptom of CKDu is dysuria, and workers may self-prescribe aminoglycoside antibiotics which are poorly regulated in Mesoamerica (Ramirez-Rubio et al., 2013).
Leptospira Infection
Leptospirosis is a widespread zoonotic disease that can be transmitted to humans through soil or water contaminated by infected animal urine. Agricultural workers may be exposed to Leptospira bacteria in soil and water during cultivation and harvesting tasks. Surveillance data from a Nicaraguan hospital reported an outbreak of leptospirosis in 1998, a peak in 2001, and an endemic cycle consistent with El Niño–Southern Oscillation weather patterns (Murray et al., 2015). In a longitudinal study in Nicaragua, seropositive sugarcane workers had higher NGAL concentrations (relative mean= 1.28; 95% confidence interval [CI] = [0.94, 1.75]) (Riefkohl et al., 2017). Leptospirosis is an asymptomatic infection, and those with severe Leptospira infection sometimes present with AKI. Although it has not been established that acute Leptospira infection leads to CKDu, it may be a factor that increases susceptibility to CKDu (Yang, 2018).
Genetic Factors
Advances in genetic research have shown that the prevalence and risk of developing traditional CKD can vary according to ethnicity, so genetics may also play a role in the development of CKDu. A study conducted among 200 nonworking Nicaragua adolescents (ages 12-18 years) from four different school locations (Ramirez-Rubio et al., 2016) assessed biomarkers of kidney injury including the ACR, NGAL, NAG, and IL-18. Elevated renal biomarker levels were observed in adolescents in regions with higher comparative CKDu mortality rates (Ramirez-Rubio et al., 2016). Familial clustering suggested possible genetic susceptibility and/or hazardous environmental exposure; however, the study did not assess these factors. Furthermore, renal biomarkers assessed do not have established normal values for adolescents, making comparison with adult populations difficult.
Socioeconomic Risk Factors
Risk factors for CKDu are potentiated by social and economic factors such as extreme poverty, which obligates workers to work in extreme and harsh conditions (Bodin et al., 2016; Crowe et al., 2013; Wesseling et al., 2014; Wesseling, Aragon, Gonzalez, Weiss, Glaser, Bobadilla, et al., 2016). Studies in Nicaragua found agricultural fieldworkers to be at greater risk of decline in kidney function as compared with nonfieldworkers (Laws et al., 2015; Torres et al., 2010; Wesseling, Aragon, Gonzalez, Weiss, Glaser, Rivard, et al., 2016). Factors such as poor hydration, lack of rest breaks, lack of heat-related illness prevention training, use of clothing or equipment that increases body heat or decreases the efficiency of sweat evaporation, low wages, and lack of sufficient workplace regulation can further complicate heat stress.
Intervention Studies
To date, the only intervention study that has been conducted in the Mesoamerican region has been an adapted protocol from the Occupational Safety and Health Administration’s (OSHA) “Water. Rest. Shade.” (WRS) program in El Salvador (Bodin et al., 2016; Wegman et al., 2018). Sugarcane workers were given Camelback™ water backpacks, mobile shade structures, scheduled rest periods, and ergonomically improved machetes. The results were an increase in quantity of sugarcane harvested, a reduction in symptoms associated with heat stress and dehydration, and an increase in water consumption (Bodin et al., 2016). Although the decrease in eGFR was less for the intervention group (−3.4 mL/min/1.73 m2) compared with the control group (−5.3 mL/min/1.73 m2), additional research is necessary to assess whether the intervention can reduce the risk of developing CKDu (Wegman et al., 2018). Furthermore, it is important to note that this intervention study was developed under the hypothesis that heat stress was an etiological factor of CKDu.
U.S. Studies
Despite no clear pattern of risk factors associated with CKDu, recent reports have suggested that workers from Mesoamerica who are employed in the U.S. also exhibit signs of kidney injury. In Central Valley, California, there were anecdotal reports of AKI and CKD among migrant agricultural workers (Horton, 2016). A study conducted in Central Valley, California, with 295 agricultural workers found that 12% had pre- to postwork shift increases in SCr of at least 0.3 mg/dL or 1.5 times the preshift value, AKI according to the KDIGO criteria (Moyce et al., 2016).
Findings from a Florida study showed that agricultural workers lived in a state of chronic dehydration and experience elevated core body temperature while working (Mac et al., 2017). Of the 192 agricultural workers, 53% started their workday in a dehydrated state (USG ≥1.020), and 78% were dehydrated by the end of the workday (Mix et al., 2018). On at least one of three workdays, 33% of workers experienced pre- to postwork shift SCr increases of at least 0.3 mg/dL or 1.5 times the preshift value, AKI using the KDIGO criteria, and for each 5°F increase in heat index, the odds of AKI increased 37% (Mix et al., 2018).
Discussion
This literature review describes published evidence regarding the clinical manifestation and possible etiological factors associated with CKDu in Mesoamerican populations. These results demonstrate that there is no consistent definition or gold standard for CKDu; nevertheless, the epidemiological evidence of an increase in mortality from a type of kidney disease that does not fit the usual pattern of CKD is compelling. Possible etiological factors include heat stress, pesticide exposure, genetic susceptibility, heavy metals, and medications.
Further research is needed to provide valid and reliable assessment of biomarkers of agrochemicals, hydration, and renal injury among diverse communities in occupational settings. Although existing CKDu studies provide useful data on risk factors, further longitudinal epidemiological studies are needed to address reverse causality. In addition, a consistent case definition of CKDu and methodology are needed to conduct better research studies where measures are comparable across different populations. Joint studies of the prevalence and incidence of AKI and CKDu among agricultural workers in the U.S. and the Mesoamerican region are also needed to monitor the disease at a global level.
Implications for Occupational Health Nursing
Reports of AKI and CKD in the U.S.-based agricultural worker population and studies showing chronic dehydration in agricultural workers call for careful vigilance. Occupational health nurses can play important roles in recognizing kidney disease among agricultural workers, advocating for heat stress prevention strategies and conducting research on etiological factors and interventions to decrease heat stress in workers.
Occupational and community health nurses should assess work histories to identify patient occupation, provide guidance in the management of musculoskeletal pain to prevent overuse of NSAIDs, educate patients on the potential risks of self-treatment with antibiotics for urinary symptoms, and encourage patients to seek professional care for urinary symptoms to decrease the risk of AKI. Examination should include assessing SCr and eGFR for patients identified as high risk based on their medical and occupational history and presenting symptoms. Strategies to combat an epidemic of CKDu include instructions to drink 8 oz of water every 15 to 20 minutes for work periods of moderate exertion, with the incorporation of a sports drink containing electrolytes and low sugar for prolonged work periods with excessive sweating (Jacklitsch, Musolin, Coca, Kim, & Turner, 2016) (Table 1).
Studies Pertaining to Acute Kidney Injury and Chronic Kidney Disease of Unknown Etiology (CKDu) Among Mesoamerican Workers
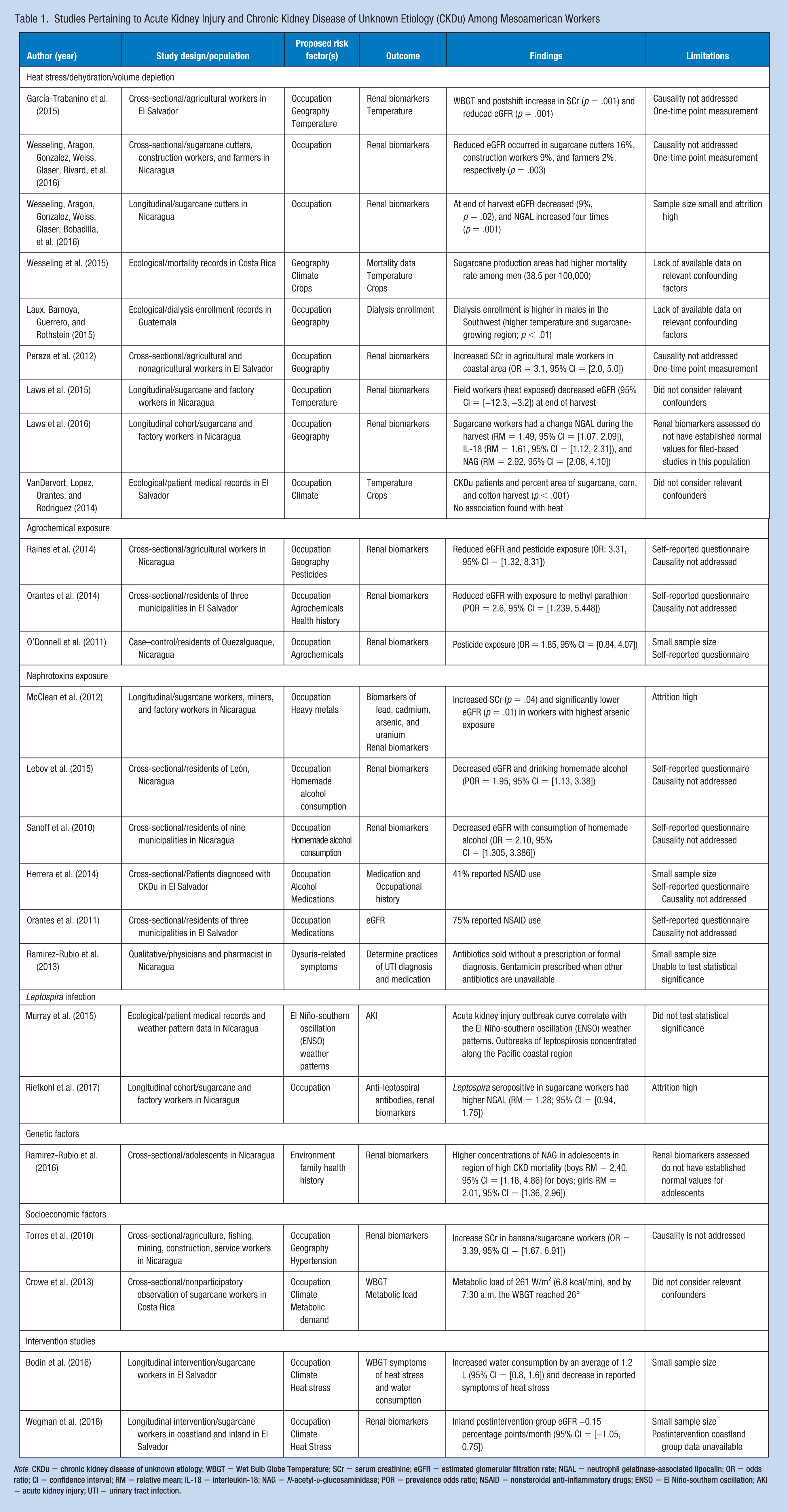
Note. CKDu = chronic kidney disease of unknown etiology; WBGT = Wet Bulb Globe Temperature; SCr = serum creatinine; eGFR = estimated glomerular filtration rate; NGAL = neutrophil gelatinase-associated lipocalin; OR = odds ratio; CI = confidence interval; RM = relative mean; IL-18 = interleukin-18; NAG = N-acetyl-
Conclusion
Evidence suggests that CKDu is a multifactorial disease. Preventive approaches are key to reducing the morbidity and mortality associated with CKDu and to relieving the global burden on disadvantaged populations, such as agricultural workers. Many of the proposed hypotheses about the cause of CKDu relate to behaviors that can be changed via occupational health and safety training and public health policies that protect agricultural workers. More research is needed to understand the complexity in the interactions between global exposures and local factors and behavior practices. Reducing the global prevalence of CKDu will require more robust studies on causal mechanisms and on interventions that can reduce morbidity and mortality in vulnerable populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Roxana Chicas, BSN, RN, is a PhD candidate at Nell Hodgson Woodruff School of Nursing. Her research focuses on occupational and environmental heath, and work safety interventions.
Jacqueline Mix is an adjunct professor at Nell Hodgson Woodruff School of Nursing. Her research is primarily focused in the areas of environmental and cancer epidemiology.
Valerie Mac, PhD, FNP-C is an assistant professor at Nell Hodgson Woodruff School of Nursing. Her research focuses on biomonitoring and the health effects of heat in vulnerable and occupational populations.
Joan Flocks is the Director of the Social Policy Division at the Center for Governmental Responsibility (CGR), University of Florida Levin College of Law. She teaches courses and publishes in the areas of social and environmental justice.
Nathan Eric Dickman is an associate professor of philosophy and religious studies at Young Harris College. He researches and teaches about global social justice issues in ethic and religions.
Vicki Hertzberg is a professor and the Director of the Center for Data Science in the Nell Hodgson Woodruff School of Nursing. Her research focuses on developing and applying statistical methods for the analysis of network data.
Linda McCauley is dean and professor at Nell Hodgson Woodruff School of Nursing. Her research focuses on occupational and environmental studies of working populations and children.