
Abstract
Physical activity readiness of front-line employees caring for adults with disabilities (N = 381) improved during a two-phase project based on stages of change (SOC) theory. In Phase 1, we assessed barriers to, and readiness for, participation in an employee wellness program. We collected data from workers using focus groups and a preintervention physical activity readiness survey. Focus groups (N = 14) identified barriers, including lack of communication about the employee wellness program. With respect to their SOC (N = 82), 7% were in precontemplation, 16% in contemplation, 52% preparation, 5% in action, and 20% in maintenance SOC. In Phase 2, we aimed to improve readiness for participation in the program. We used SOC-based employee Facebook group messages, a health education fair, and measurement through a postintervention physical activity readiness survey. The mean number of “views” in which the workers saw the 16 theory-based messages was 12.2 (range = 0-27). Fourteen adults and 17 children attended the fair. Postintervention survey results (N = 125) indicated physical activity readiness improvement with 1% in precontemplation, 21% in contemplation, 33% in preparation, 33% in action, and 12% in maintenance SOC.
Keywords
Introduction
Physical inactivity, defined as less than 150 minutes of moderate intensity and 60 minutes of vigorous-intensity physical activity per week (Harris, Huang, Hannon, & Williams, 2011), contributes to an estimated 6% to 10% of coronary artery disease, type II diabetes, breast cancer, and colon cancer (Lee et al., 2012). Of the 36% to 54% of employees who are physically inactive, higher levels of physical inactivity are observed among low-income, less-educated workers (Goetzel et al., 2012; Harris et al., 2011). On average, physically inactive employees cost employers 15% more than physically active employees (Goetzel et al., 2012). In fact, physical inactivity costs employers an estimated US$9.1 billion per year due to absenteeism (Asay, Roy, Lang, Payne, & Howard, 2016).
Employee wellness programs consist of health promotion policies, procedures, programs, and system designs implemented at the worksite with the goal of improving the health and safety of employees (Centers for Disease Control and Prevention, 2016). One role of an occupational and environmental health nurse is to promote health by developing an employee wellness program (American Association of Occupational Health Nurses, 2018). Design of programs that support healthy lifestyle changes and create opportunities for individual employees to lower risks of disease and injury and to promote physical activity is within the scope of practice for an occupational and environmental health nurse. Successful programs include clear designs and goals set in a strong organizational culture (Goetzel et al., 2012). Moreover, successful programs incorporate multiple activities and clearly communicate program expectations to upper management (Goetzel et al., 2012; Mitchell, Ozminkowski, & Serxner, 2013).
Overview and Context of the Quality Improvement (QI) Project
A committee oversaw the employee wellness program in a Midwestern company that employed Direct Support Person (DSP) employees. This program previously provided free and reduced-cost Fitbits to employees through a grant that expired. It previously provided discounted or free group fitness classes. Employee wellness and physical activity were assessed annually among all employees in a wellness survey. An employee Facebook group with 37 DSP employees and 200 additional executive, administrative, technical, and health care workers existed for informational communication regarding committee activities, special employee recognition, social communication, and legislative lobbying. When this QI project began, the committee was inactive and did not have a chair or a DSP member, causing the program to decline. The middle- and upper level employees identified the problem of a lack of participation in the employee wellness program among DSPs, while upper- and middle-level employees participated in the program. In addition, the employee wellness program was partially suspended in 2016. Therefore, the purpose of this QI project was to improve participation among DSP employees whose participation in the employee wellness program lagged behind that of upper- and middle-level employees. The three aims of this QI project were to (a) improve readiness for participation in an employee wellness program of DSPs using the transtheoretical model’s stages of change (SOC), (b) improve employee wellness program communication, and (c) assess and make recommendations to improve physical activity (e.g., walking).
Framework
The transtheoretical model provided a planning and conceptual framework for this QI project (Prochaska, 2008; Prochaska & DiClemente, 1982). More specifically, it provided guidance on tailoring interventions to a population’s level of physical activity based on its assessed Stages of Change (SOC). The SOC is one of the four basic constructs in the transtheoretical model and includes precontemplation (not ready for change), contemplation (thinking of changing), preparation (intending to begin changes based on action plan), action (achieving positive behavior change), maintenance (continues behavioral change), and termination (discontinuing change processes as unhealthy behaviors have ceased; Prochaska, 2008; Prochaska & DiClemente, 1982). We used this model to predict physical activity levels by assessing a baseline SOC. From there, we created a goal of how many people should be in the action or maintenance stages, which would reflect achieving and continuing a positive health behavioral change. After the intervention, we reassessed the SOC to see how much improvement in physical activity actually occurred. In addition, each SOC requires different techniques to improve the health behavior. As many of our target population started in the preparation stage, we created an intervention that used social support systems, which are especially important in this stage.
Review of Relevant Literature to Guide Our Program
We began this QI project by reviewing the literature as a means to guide our work. Literature searches were conducted in CINAHL, PUBMED, MEDLINE, and Google Scholar databases using the following keywords: physical activity, employee wellness program, worksite health program, African American, low socioeconomic women or females, Fitbit, social media, social networking, the Transtheoretical Model, and Stages of Change. Search terms were chosen based on their pertinence to the target population’s demographics, the theoretical model chosen, the employee wellness program, and the programs focusing on Fitbits. One hundred and fifty articles were identified and 27 were kept due to their relevance. Feasibility studies, studies not published in English, and articles greater than 10 years old (unless an older article significant to the subject development) were eliminated. Sources retained included three systemic reviews and/or meta-analyses, nine quantitative studies, 13 qualitative studies, one book, and one clinical review article. The six older articles retained provided background information on the logic model or the transtheoretical model’s SOC in regard to physical activity.
An employee wellness program using multiple activities with telephone calls with nurses, health coaches, and health advocates found that participants had fewer days of work missed due to illness and higher productivity (Mitchell et al., 2013). Another study found that employee wellness programs reduced the health care costs by an average of US$358 per employee per year (Baicker, Cutler, & Song, 2010). Eighty-three percent of employers reported employee wellness programs positively affected worker performance and productivity (McCleary et al., 2017), as well as cost savings (Baicker et al., 2010; Mitchell et al., 2013). Successful comprehensive wellness programs included health education, a supportive social and physical environment, organizational integration, links between the wellness program and similar programs, and health screenings followed by education and counseling (Goetzel et al., 2012; Mitchell et al., 2013). Some included physical activity components using Fitbits (Giddens, Leidner, & Gonzalez, 2017). Fitbits, wearable pedometers, were found to be effective tools for improving physical activity in employee wellness programs, including the optional features that were found to improve step count (Giddens et al., 2017). Features in the Fitbit included a calorie counter; a virtual community, which connects friends to compete with virtual walking challenges; and sleep monitor. Fitbit’s optional features were found to positively affect employee lifestyle choices, with significant improvements measured in walking distance and well-being (Giddens et al., 2017).
Walking is considered a moderate-intensity physical activity; however, adults only average 5,117 steps per day, consistent with physical inactivity (Bassett, Wyatt, Thompson, Peters, & Hill, 2010; Tudor-Locke et al., 2011). An evaluation of walking distance recommendations found that walking 7,000 to 8,000 steps per day is a reasonable goal consistent with public health guidelines (Tudor-Locke et al., 2011).
Women with low socioeconomic status (SES) reported a lack of encouragement as a perceived barrier to physical activity; social support was useful for low-SES women to achieve objectives (Chang, Nitke, Guilford, Adair, & Hazard, 2008; Hoebke, 2008). Both online and in-person social support may be able to fill this need. Low-SES mothers also reported lack of child care as a perceived barrier to physical activity (Hoebke, 2008). African American and Latina women were often reluctant to engage in physical activity (Hoebke, 2008). African American women may consider exercise to be superfluous, and some view work and household chores as physically demanding enough (Hoebke, 2008). In addition, child care created time barriers for younger African American women; therefore, they may benefit from online surveys or communications (Buchholz et al., 2016).
A systemic review of 10 studies on social networking sites and health behavior change found that using Facebook for communication promoted participant retention in wellness programs (Maher et al., 2014). Social networks, like Facebook, significantly improved health behavior. An individually tailored, website-delivered intervention determined that physical activity increased and weekday sitting time decreased relative to the control group (Spittaels, De Bourdeaudhuij, & Vandelanotte, 2007). Therefore, tailoring interventions to the individual physical activity level helps achieve plausible goals and can be implemented through the social support of online group networks.
An employee’s stage of readiness to change has been found to predict physical activity levels (Bezyak, Berven, & Chan, 2011; Horiuchi, Tsuda, Watanabe, Fukamachi, & Samejima, 2012; Rosenkranz et al., 2015). For example, the likelihood of employees signing up for a workplace physical activity challenge was 1.64 times higher for those in the preparation stage versus the precontemplation and contemplation stages and 1.98 times higher for those in the action/maintenance stages (Walker, Tullar, Taylor, Roman, & Amick, 2016).
Tailoring interventions requires effective communication strategies, and theory-based strategies are more effective than strategies not rooted in theory (Korda & Itani, 2013). Helping relationships (also called social support) from family, health care workers, and friends are especially important in the preparation stages when starting an exercise program (Gibbison & Johnson, 2012; Substance Abuse and Mental Health Services Administration [SAMHSA], 1999). Organized social support can provide critical support for people in the preparation stage to advance to action (Singer, 2006). Furthermore, communication strategies should be culturally appropriate for the specific population (Korda & Itani, 2013).
Successful employee wellness programs have many different activities and clear program goals that are supported by the organizational culture. Employee wellness programs that use Fitbits should focus on optional features. Social support is important in the preparation stage and for low-SES mothers. Facebook can be a useful communication tool for employee wellness programs. When using Facebook, writing theory-based messages is more effective. A lack of literature exists for physical activity among low-SES and African American mothers. This QI project focused on employees where the majority low SES, African American, and valued motherhood. It hopes to address this gap in the literature.
Method
Setting and Sample
The target population was DSPs, who provided care to adults with disabilities, recruited from a population of DSPs working in a single suburban county (N = 381). The DSPs aged 18 to 65 years were eligible for the program.
The agency was a social service agency in the Midwest providing client services, including day programs, residential programs, and supportive employment programs, to people with intellectual and developmental disabilities. The agency employed more than 900 people and has several locations in two states. The target population differed from the overall agency population.
Program Design and Planned Activities
This two-phase QI project was conducted from September 2016 to July 2017. After review of the project by Rush University’s institutional review board, it was determined to be a QI project and did not require informed consent. Recruitment was broad and included workplace flyers, emails to middle management encouraging recruitment of DSP employees, Facebook advertisements, and word of mouth.
Initial Program Assessment
The Kellogg Logic Model (W.K. Kellogg Foundation, 2004) guided us in this program to initially assess our program setting, identify the problem, and determine resources and needs. Furthermore, the model emphasized evidence-based strategies and assumptions, which then defined the activities needed to create the desired change.
Key informant interviews were conducted with employees representing all levels throughout the QI project. First, we sought to identify the problem. Key informants gave opinions on the program and problems with participation of DSP employees. Then, we determined what financial and agency resources were available, such as a tent for the employee wellness fair (Figure 1). Using the literature review, we created activities in our intervention (Phase 2) that create the desired change of improving readiness for employee participation in the employee wellness program. Next, based on the logic model, we then delineated resources and program activities that led to the intended results. These results include outputs (direct products resulting from the activities), outcomes (short-term changes in behavior, functioning, or skills), and impacts (long-term changes in behavior, functioning, or skills). For example, an output, or direct result of the activity, was a family wellness event that occurred and included inexpensive physical activities. An outcome goal, or short-term change, included 35% of the target population should be in the action or maintenance SOC by the end of the intervention (Figure 1). An impact, or long-term change goal was that 50% of the target population should be in the action or maintenance SOC by 2020.
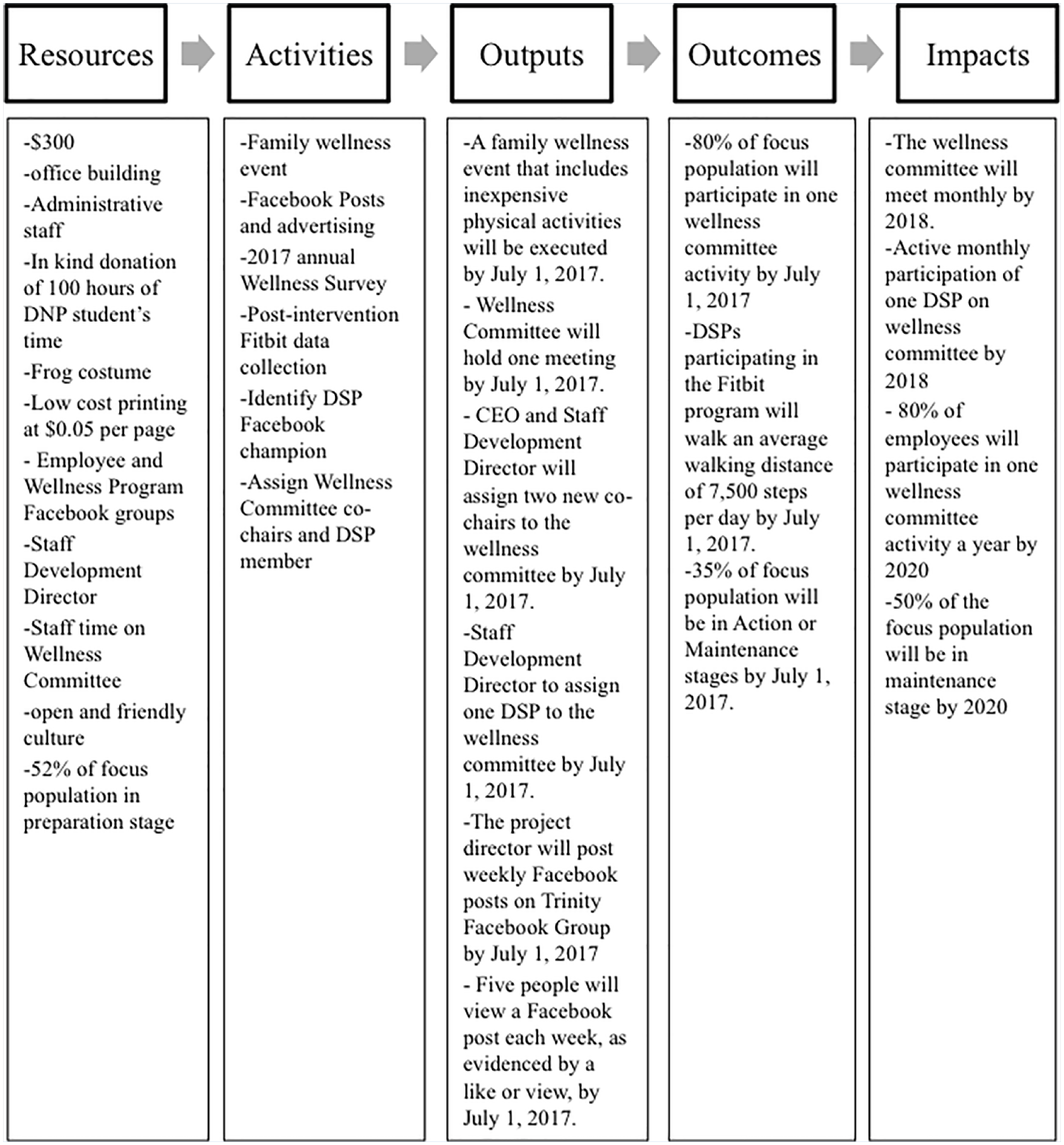
Kellogg logic model applied to worksite quality improvement program.
Phase 1
Focus groups
The purpose of Phase 1 was to assess barriers to and readiness for participation in an employee wellness program (Table 1). In Phase 1, the Kellogg Logic Model was used to guide the assessment of the existing employee wellness program. Two focus groups were conducted to determine resources and barriers to the physical activity component of the employee wellness program; a survey assessed preintervention SOC; and a Fitbit assessment evaluated baseline physical activity of employees. After identifying resources and barriers, QI activities related to the employee wellness program were developed. Measurable outputs, outcomes, and impacts were created congruent with the project aims and from key informant interviews. Phase 1 measures included focus group responses that addressed the existing employee wellness program; a 16-item preintervention survey evaluating the employee wellness program, physical activity tracker usage, and physical activity; and specific physical activity assessment using a Fitbit physical activity tracker and companion software.
Measures Obtained From DSP Workers by Project Phase
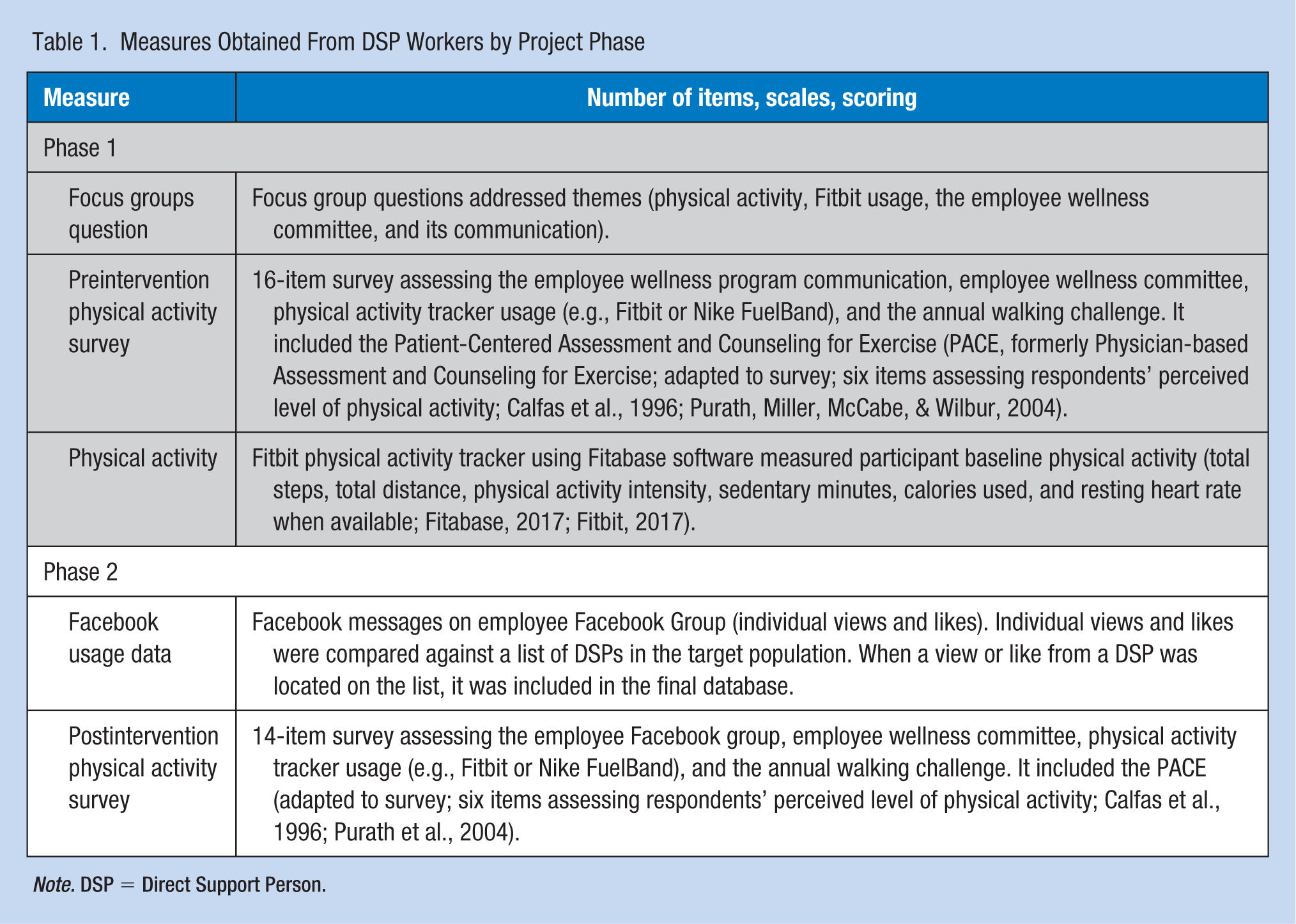
Note. DSP = Direct Support Person.
Three experienced facilitators led the focus groups. Narrative data from the focus groups were collected through audio recording. These data were then transcribed verbatim. Focus group participants were compensated for their time with US$30 per participant, with funds provided by a university grant.
Preintervention physical activity readiness survey
The committee administered an annual wellness survey to which additional questions were added as part of the QI project in 2016 with input from key informant interviews to assess SOC for physical activity (Calfas et al., 1996; Purath, Miller, McCabe, & Wilbur, 2004), employee wellness program communication, and physical activity tracker usage. All agency employees (the larger population) were anonymously asked to participate. Surveys were administered via pencil and paper, and online using SurveyMonkey. Paper results were later manually entered into SurveyMonkey. Employees with work-provided email addresses were emailed links to the survey. Employees without work-provided email addresses were given paper surveys, and completed surveys were faxed to the QI project. Participation was incentivized with the opportunity to win one US$10 gift card to a local store.
Physical activity
To determine the activity level of already active DSPs and make activity recommendations, DSPs participated in a Fitbit activity assessment. The DSPs could either provide their own Fitbits or use a loaned Fitbit from the agency. Each participant was followed for 90 days, with rolling admission to the assessment from December 2016 to March 2017 to recruit the goal number of participants. Participants were emailed a link from the companion database software, Fitabase, to synchronize their Fitbit account to Fitabase. Every time the participant uploaded or synchronized their Fitbit to a phone, computer, or tablet, their data automatically went to Fitabase. We reviewed participant data weekly and reminded participants to wear their devices and synchronize data regularly. Delinquent participants were reminded to participate via email to middle management, who then promoted participation.
Phase 2
The purpose of Phase 2 was to improve readiness for participation in an employee wellness program. Phase 2 activities targeted predetermined goals communicated via an existing employee Facebook group. The purpose of this group was to improve communication of program events, activities, and goals. A health education fair took place to educate employees on family-friendly physical activities, and a survey was used to reassess SOC. Phase 2 measures included subjective individual views, including “likes” on Facebook messages and a 14-item postintervention physical activity survey evaluating the employee Facebook group and the employee wellness program. The employee Facebook Group had 37 DSP employees and 200 additional executive, administrative, technical, and health care workers.
Facebook usage
Due to Phase 1 focus group interest in electronic forms of employee wellness communication, the QI principal investigator spoke to an employee working in information technology about ways to disseminate information electronically with DSPs and decided to use an existing workplace Facebook group to improve communication about the employee wellness program.
Sixteen theory-based messages were posted on the existing employee Facebook group from April 2016 to June 2016. Messages included images and text. Messages were designed to improve the target population’s SOC using the processes of change and motivational messages, focusing on consciousness raising, self-liberation, short-term goals, helping relationships, and stimulus control. Additional messages focused on existing employee wellness program activities and the health education fair. Facebook advertisements promoted the health education fair and were posted weekly for 1 month leading up to the fair. Based on our population’s demographics, these messages targeted women aged 18 to 65 years in the agency’s county using the key words family, motherhood (due to a focus group finding of the importance of family), and the agency’s name. Individual and new or first-time views of each Facebook message were counted to determine Facebook participation of DSPs.
Health education fair
Because the focus groups in Phase 1 indicated interest in participating in physical activity with their families, a health education fair open to all agency employees focusing on family-friendly physical activities was organized and staffed by the QI project director, agency staff, and three volunteers. Inexpensive physical activities were highlighted based on focus group and survey data. These activities included jump rope, hopscotch, ball games, skip-it, and chasing bubbles. The agency provided the materials. Children who participated received a free prize.
Postintervention physical activity readiness survey
The committee administered an annual wellness survey, to which additional questions were added again as part of the QI project in 2017 with input from key informant interviews. The QI project developed additional specific questions to reassess SOC (Calfas et al., 1996; Purath et al., 2004) for physical activity and to assess the Facebook group communication. All agency employees (the larger population) were anonymously asked to participate. Specific statistics were calculated for DSP employees only. Surveys were administered identically as in the preintervention physical activity readiness survey.
Quantitative data analysis
We used SPSS 19 to analyze quantitative data. Physical activity readiness results were described with percentages. Physical activity results were examined via means and standard deviations. Facebook results were examined with means and range statistics. Health education fair results were described using frequencies. We used contingency table analysis to assess changes in SOC.
Qualitative data analysis
For focus group data, thematic and subthematic coding was used. Coding took place independently between two raters and was then reconciled if differences were found. Coding used semantic utterance classification (Dauphin, Tur, Hakkani-Tur, & Heck, 2014), which counted every time a theme was uttered, whether positive or negative, to enumerate the level of interest in the theme.
Results
Phase 1
Qualitative data from the focus groups (N = 14 participants) revealed that most participants self-reported being physically inactive and very few walked for exercise or transportation (Table 2). Participants identified physical inactivity as a problem, but were not aware of the employee wellness program or its activities. Most did not know about the Fitbit program. Participants reported that their worksites lacked Internet access and that DSPs did not receive work email addresses and therefore could not communicate with agency employees via email. As a result, communication occurred by word of mouth or printed information given by direct supervisors. Several suggestions were made to improve communication, including receiving wellness program information in their personal email or a text message with a link to the online calendar.
Focus Group Discussion Points Regarding Resources and Barriers to the Physical Activity Components of the Employee Wellness Program
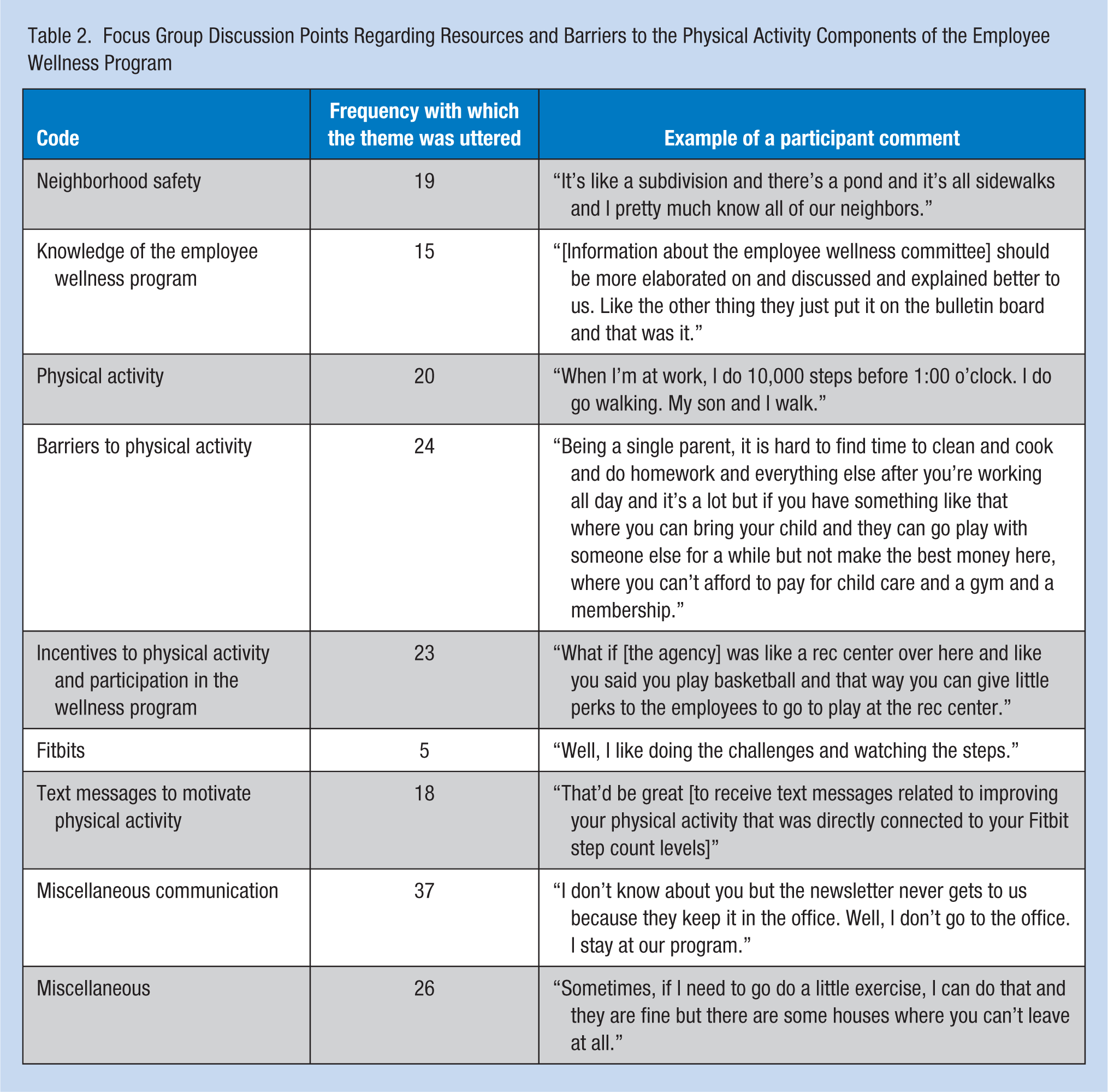
Focus group participants reported interest in becoming more physically active and participating in the employee wellness program. However, they reported barriers to participating in the employee wellness program including: poor communication about wellness program activities, as well as lack of time, money, or child care. Recommendations for program improvement included family wellness activities, such as exercising as a family or playing basketball with their children. Participants noted that they wanted employee wellness program activities to include family interaction and children in physical activity. They also discussed the importance of spending time with their families.
The 2016 survey had a 21.5% response rate among DSPs (82/381). Seven percent reported being in the precontemplation, 16% in contemplation, 52% in preparation, 5% in action, and 20% in maintenance SOC (Figure 2). Sixty-four percent of DSP respondents did not know about the Fitbit program, and 84% did not know about the virtual walking challenge. Suggestions for communication improvement included wellness program information sent to personal email addresses (56%) and cell phone text messages (53%). Twenty-six percent reported interest in a family-oriented wellness event. Fifty-three percent of survey respondents reported interest in a walking wellness activity. Twenty-three percent of respondents had used a Fitbit or other wearable pedometer and found that the information motivated them to exercise. Respondents recommended a wellness program activity be conducted on Monday between 12:00 p.m. and 1:30 p.m.
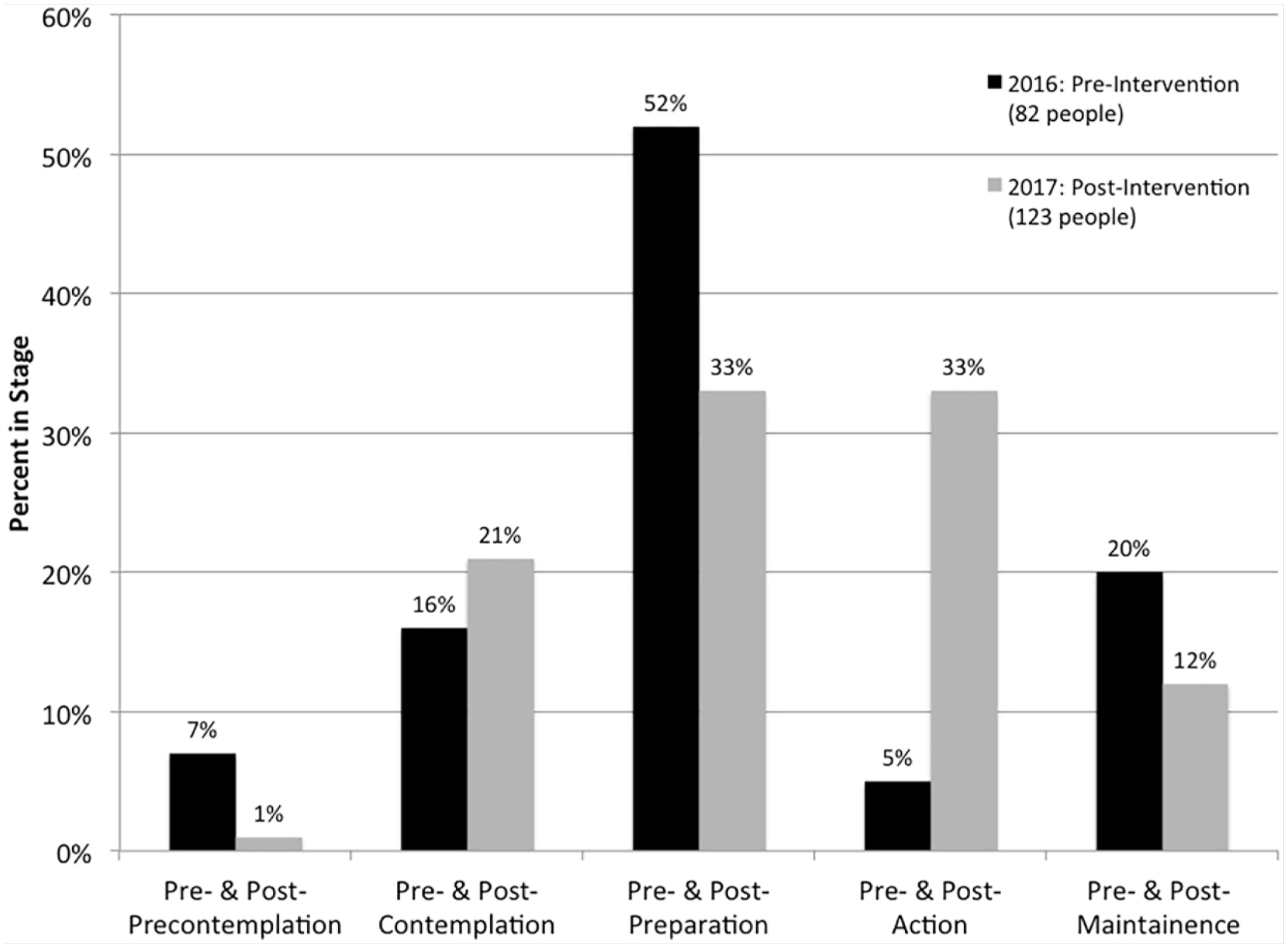
Stages of change: Pre- and postquality improvement project.
There were 24 participants in the Fitbit assessment. The baseline Fitbit assessment showed an average steps per day of 7,245 (SD = 4,030); average time of Fitbit use was 63% of days tracked (SD = 24%).
Phase 2
Thirty-seven DSPs participated in the Facebook interaction. Mean views per theory-based message was 12.2 (range = 0-27) and average total new views per theory-based message was 2.9 (range = 0-11). Attendees at the health education fair included two DSPs, 17 children, and 12 non-DSP adults.
In Phase 2, the postintervention 2017 survey had a 32% response rate among DSPs (n = 123/381). One percent reported being in the precontemplation, 21% in contemplation, 33% in preparation, 33% in action, and 12% in maintenance SOC (Figure 2). Seventy percent did not know about the Fitbit program, and 54% did not know about the virtual walking challenge. However, 21 (17%) respondents participated in the virtual walking challenge, and twenty-three percent belonged to the employee Facebook group. Of those who did belong to the Facebook group, 75% enjoyed getting information about general health through the group. Of those who did not belong, 46% said they did not want to join a work-related Facebook group.
Organizational change
This committee was nonexistent prior to this QI project. The committee was restarted with one chair and four members. The chair assisted in the 2017 virtual walking challenge. The four members included administrative staff with an interest in leadership and/or physical activity. All were recruited through the QI project’s agency facilitator based on key knowledge of the agency. Although no DSP members were recruited, the committee continues to focus on improving participation in physical activity by DSPs and provides infrastructure support to do so. The existing employee Facebook group expanded to include employee wellness program information. In addition, a health education fair was developed to incentivize DSP participation in the employee wellness program based on their interest in family activities.
Recommendations to Improve Physical Activity
Recommendations to the agency to improve physical activity among DSP employees included the following: (a) maintain committee to provide ongoing infrastructure support for improving physical activity and continue recruitment of DSP members; (b) continue Facebook messages based on the transtheoretical model; (c) continue to promote low-cost forms of physical activity that can also involve family; and (d) set 7,500 steps as a reasonable beginning goal for walking per day for employees. In addition, we recommended continuing communication of employee wellness program information on the employee Facebook group and by purchasing Facebook advertisements for the annual walking challenge.
This QI project showed that readiness for participation in an employee wellness program was successfully improved by using the SOC theory–based Facebook messages. In addition, employee wellness program communication was improved by using an easily implemented and inexpensive employee Facebook group. Occupational health nurses can act as Facebook group administrators and disseminate program information. When designing an employee wellness program, occupational health nurses should include employee opinion by establishing a committee to oversee the employee wellness program, which we recommended to our agency to improve physical activity. Occupational health nurses should include families in the program design, which can increase participation in a population of low-SES, minority, and female workers. Finally, the logic model was a useful tool for occupational health nursing students to guide their assessment, goals, and intervention of an employee wellness program. Assessing resources for a not-for-profit agency significantly affected the size and scope of the intervention a student could do.
Limitations
A budget and staffing crisis limited the number of DSPs who participated in the employee wellness program. The salary for DSPs is determined by the state and had not been increased in several years (Garcia, 2016). In addition, the agency was funded by state money, which was limited during a state budget crisis. Both the lack of salary increases and limited agency funds led to DSPs leaving and the agency being unable to hire new DSPs. Both DSPs and management were overworked. The agency’s focus changed from the committee to ensuring that group homes were safely staffed (T.Sieling., personal communication, June 1, 2017). Therefore, only two DSPs were able to attend the health education fair. Despite a budget crisis, this program was successful; therefore, it could be disseminated to other companies.
A follow-up Fitbit assessment was limited by attrition of participants; therefore, it was not completed. Five participants left the agency, and five others lost their Fitbits. In addition, funding for the Fitabase software did not include follow-up assessment data collection. The alternative option of participations using written logs was not possible because of lack of direct communication due to agency policy.
Discussion
This QI project was successful in improving SOC among a target population of low-SES, minority, female DSP workers. Little is known of this target population. Employees viewed the employee Facebook group, which improved wellness program communication in a large, distributed agency. The percentages of participants in the action and maintenance stages increased, while the percentage in the preparation stage decreased. It can be posited that the decrease in percentage in the preparation stage was due to movement from the preparation stage to the action or maintenance stages.
Our finding of increased percentages in the action or maintenance stages in this QI project using the social network Facebook was consistent with the literature that helping relationships (also called social support) are important in the preparation stages and for low-SES mothers (Chang et al., 2008; Gibbison & Johnson, 2012; Singer, 2006; SAMHSA, 1999). Our use of theory-based Facebook groups and messaging to improve readiness to participate in an employee wellness program reinforced a finding that Facebook communication promotes participant retention in wellness programs (Maher et al., 2014), although participation and retention are different. Our development of a family-friendly health education fair was consistent with the literature showing that lack of child care is a perceived barrier to physical activity among low-SES and African American women (Hoebke, 2008). Including children eliminated this perceived barrier. Including family members in employee wellness program activities could incentivize DSPs due to their focus on family time.
Footnotes
Acknowledgements
The authors acknowledge the following people: Debra Batchelor, Bridget Chidsey, Roberta Fugate, Nancy Samardzic, and Trina Sieling.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Alissa S. Miller, DNP, APN, AGPCNP-BC is a nurse practitioner in Anesthesia Perioperative Medicine at the University of Chicago Medicine. She graduated from Rush University with a DNP in population health.
Sarah H. Ailey, PhD, RN, CDDN, PHNA-BC is a professor at Rush University’s College of Nursing, with a research focus in community health and intellectual disabilities. She is currently investigating the effect of the Steps to Effective Problem-solving (STEPS) program in group homes, funded by an R01 grant from the Eunice Kennedy Shriver Institute.
Susan Weber Buchholz, PhD, RN, FAANP is a professor at Rush University’s College of Nursing with a research focus in adult primary care, physical activity, health promotion, and mHealth. Her long-term research program goal is to develop cost-effective strategies to increase physical activity among sedentary adults. Globally, she is one of the first researchers to use a Sequential Multiple Assignment Randomized Trial design to explore how to optimize adaptive interventions to improve physical activity.
Louis Fogg, PhD is an expert in clinical research methodology who studied with Donald Fiske, the renowned authority in research design and measurement. He received his PhD in behavioral research methodology from the University of Chicago in 1987 and has been on faculty at Rush University Medical Center since that time.
Diana Ingram, PhD, MPH is a researcher and professor at Rush University with a research focus in public health. She is an expert in designing, implementing, and coding focus groups.