
Abstract
Call centers in Korea have been found to be operated mainly by women, and they experience high levels of job-related stress. Compared with the general population, the prevalence of smoking among women in Korea’s call centers is strikingly high. Little attention has been paid to the associations between smoking behavior and their emotional labor, occupational stress, and health-promotion behaviors. For this cross-sectional study, a paper-based survey was conducted in a sample of female employees in a credit card call center (N = 309). Among the participants, about 20% (n = 62) were current smokers. Smokers were less engaged in health-promotion behaviors than nonsmokers, and occupational stress was negatively associated with health-promoting behaviors in nonsmokers, but not in smokers. Smokers may use cigarettes as a way of alleviating the emotional burden of their work.
Introduction
Smoking is considered to be the most modifiable cause of morbidity and mortality (U.S. Department of Health and Human Services, 2014). Several negative health outcomes are attributable to smoking cigarettes, including cancer and cardiovascular disease. In addition, some women who smoke during pregnancy experience premature birth and infant mortality (U.S. Department of Health and Human Services, 2014). The prevalence of smoking among Korean women (5.5% in 2015) is relatively low compared with Korean men (39.3%) or with women in other countries (Korea National Statistical Office, 2016). However, a study reported that 37% of the women working in call centers smoked cigarettes when the prevalence of smoking among women was considered based on their occupations (K. Kim, 2015).
Studies have observed that psychological stress may lead to unhealthy behaviors, such as cigarette smoking (Fidler & West, 2009; Meule, Reichenberger, & Blechert, 2018). Acute stress is associated with greater cigarette use and a reduced likelihood of cessation. The link between stress and cigarette smoking has been observed to be stronger in women than in men. Men have been found to be more likely to smoke in social situations, whereas women are more likely to smoke as a psychological coping mechanism when they experience stress, anger, or depression (Ferguson, Frandsen, Dunbar, & Shiffman, 2015; Y.-W. Tsai, Tsai, Yang, & Kuo, 2008). In previous studies, female smokers were aware of the disadvantages of smoking, and many of them wanted to quit (Smith et al., 2015; Y.-W. Tsai et al., 2008); however, few were able to do so because of concerns about dealing with stress after they quit (Doran, 2014; Pang & Leventhal, 2013; Smith et al., 2015). However, prolonged cigarette smoking, irrespective of the rationale for doing so, can lead to a range of adverse health outcomes. Healthy behaviors, such as regular exercise, could also reduce psychological stress but it takes time to be effective (Hamer, 2012). As a result, many smokers may view these healthy behaviors as ineffective in dealing with their immediate stresses. Evidence has shown that stress has a negative relationship with behaviors that promote health (Han et al., 2015), so smokers are even less likely to engage in such behaviors (Thanavaro, 2005; Thanavaro, Moore, Anthony, Narsavage, & Delicath, 2006).
Call Center Work
Call centers, which provide customer services via telephone, have a very specific and unique work environment. In South Korea, call centers have been found to be operated mainly by women, and they experience high levels of job-related stress (Seoul Labor Center, 2018). Thus, the high smoking rates among the female employees of call centers in Korea may be attributed, at least partially, to the stress associated with the nature and culture of their work. Most call center operations in Korea are outsourced to specialized companies, and most of the employees are not full-time workers (Park, 2015). In addition to receiving low rates of pay and lacking job security, these workers often are exposed to customers’ hostility and verbal abuse (Croidieu et al., 2008; Kwon & Yang, 2015; Park, 2015). They are instructed to maintain a friendly manner because their performance ratings are directly related to customers’ satisfaction with their responses and demeanor. When they receive calls, the calls are monitored to evaluate their performance and to ensure that they follow the guidelines provided. Thus, while they are on the phone, they must tolerate angry, unfriendly, and abusive customers while suppressing their own feelings (M. Lee, 2017). Hochschild (1983) described this as emotional labor, which has been found to have a negative psychological effect that may create stress, anger, and/or depression (Jeong, Choi, Park, & Li, 2015; Shin, Cho, Kim, & Kim, 2015).
Given the massive expansion of telecommunications technology in Korea (Choi, 2018), call centers have become an increasingly important part of modern business, and they have generated thousands of jobs. However, the health of the employees of the call centers, who are predominately women, has been given very little consideration. In prior studies, researchers evaluated the relationships between occupational stressors including emotional labor and health behaviors only in select professional occupations, such as nursing (Liu & Liu, 2009; Y.-C. Tsai & Liu, 2012). However, a recent report indicated that even higher levels of psychological distress exist among call center employees than among clinical nurses (Oh, Park, & Boo, 2017). Even though the prevalence of smoking among the female employees of call centers is the highest among Korean working women (K. Kim, 2015), little attention has been paid to their smoking behaviors as a function of emotional labor or stress. Therefore, the purpose of this study was to evaluate the levels of emotional labor, occupational stress, and health-promotion behaviors as well as the associations among these three variables by smoking status among female call center employees.
Method
We conducted a cross-sectional study using anonymous survey methods. A sample of female call center employees was recruited from a call center of a leading credit card company in South Korea. The operation of the call center was outsourced to specialized service providers, and the center managed both inbound and outbound customer services. Inbound services focused on taking requests or complaints from customers about credit cards. Most outbound activities consisted of making calls to customers to try to persuade them to pay their past-due bills.
The data were collected in March 2016 (Oh et al., 2017). We visited the call center to explain the purpose of the research, the procedures, and the voluntary nature of the study to potential participants. After doing so, we distributed questionnaires to the female employees who had worked in the call center for at least 6 months. Once they had completed the consent form, they were asked to complete the questionnaire, which they deposited in a sealed box through a slot in the lid. The box remained in the facility for 1 week, which allowed the participants the option of completing the survey at home or at work. A coupon for free coffee was provided as compensation for their time and effort.
Measures
Participants’ characteristics
All information concerning the participants in the study was self-reported, and the information included age, education level, marital status, household income level, time worked in the call center, perceived health status, and smoking status.
Emotional labor
Emotional labor was measured with nine items in three subscales, including surface acting (three items), deep acting (three items), and emotional dissonance (three items), which were developed based on a review of the literature related to emotional labor (Brotheridge & Grandey, 2002; Jeong et al., 2015; Morris & Feldman, 1996). Surface acting and deep acting represent the different ways the participants managed their emotions to fulfill the demands of the job (Brotheridge & Grandey, 2002). Specifically, surface acting refers to faking or suppressing emotional expressions. For example, call center employees may reply to customers’ difficult complaints with a nice, friendly voice (even though they are in a bad mood) to increase the customers’ satisfaction. An example of a surface acting item is, “Hide my true feelings about a situation.” Deep acting refers to subjects’ internal efforts to control their thoughts and try to actually feel as the rules mandate that they perform—for example, “Make an effort to actually feel the emotions that I need to display to others.” Emotional dissonance is the extent to which the participant feels apart from the emotions she expresses to her customers on the phone (Morris & Feldman, 1996). Responses to each item were scored on a 5-point Likert-type scale from 1 (not at all) to 5 (a lot). Possible scores ranged from 3 to 15 for each subscale with higher scores indicating greater emotional labor. In a prior study, internal consistencies ranged from 0.85 (emotional dissonance) to 0.90 (deep acting) for call center employees (Jeong et al., 2015). In this study, the values ranged from 0.82 (emotional dissonance) to 0.88 (deep acting).
Occupational stress
Occupational stress was measured with the culture-specific Korean Occupational Stress Scale, which was developed and validated with a nationwide random sample of Korean employees (Chang et al., 2005). The scale is comprised of 24 items with the following seven subscales: Job Demands (four items), Insufficient Job Control (four items), Inadequate Social Support (three items), Job Insecurity (two items), Organizational Injustice (four items), Lack of Rewards (three items), and Occupational Climate (four items). Each item was measured on a 4-point Likert-type scale from 1 (not at all) to 4 (very much). Scores for each subscale were calculated based on the scoring method provided by the developers. The possible range for each subscale was 0 to 100 with higher scores representing higher levels of occupational stress. The values of Cronbach’s alpha ranged from .51 (occupational climate) to .82 (organizational injustice; Chang et al., 2005), and the value was .75 for clinical nurses (J. Lee, Joo, & Choi, 2013). In this study, the values of Cronbach’s alpha for the subscales ranged from .62 (insufficient job control) to .86 (organizational injustice).
Health-promotion behavior
In this study, the participants’ levels of health-promotion behavior were measured using the Health Promoting Lifestyle Profile II (Walker, Sechrist, & Pender, 1987). The scale consists of 52 items distributed among the following six subscales as indicated: Health Responsibility (nine items), Physical Activity (eight items), Nutrition (nine items), Spiritual Growth (nine items), Interpersonal Relations (nine items), and Stress Management (eight items). Responses range from 1 (never) to 4 (routinely) for each item on the profile, and the total possible subscale and overall scores are calculated by summing the scores of each item, which could range from 52 (all 1s) to 208 (all 4s). This scale has been used extensively in research with high internal consistencies for both the overall scale and the subscales (Hwang, Hong, & Rankin, 2015; H. Kim, Choi-Kwon, Kim, Park, & Koh, 2015). In this study, Cronbach’s alpha values were from .78 (nutrition) to .92 (health responsibility).
Data Analysis
Statistical analyses were conducted with SPSS 22.0. Chi-square tests, t tests, and one-way ANOVA were used to examine any differences between smoking status and levels of emotional labor, occupational stress, health-promotion behavior, and characteristics of the participants. Differences in the levels of emotional labor, occupational stress, and health-promotion behavior with the characteristics of the participants were examined with t tests. Partial correlations were conducted to examine the relationships of emotional labor, occupational stress, and health-promotion behavior with smoking status. This study was approved by the Ethics Committee of the Gachon University’s research institution.
Results
Of the 350 questionnaires distributed, 343 were returned (98%). Twenty-nine of the questionnaires were completed by men, and five others had missing data for the main study variables. Thus, 34 of the questionnaires returned were excluded leaving 309 questionnaires completed by female call center employees that had no missing data for analysis.
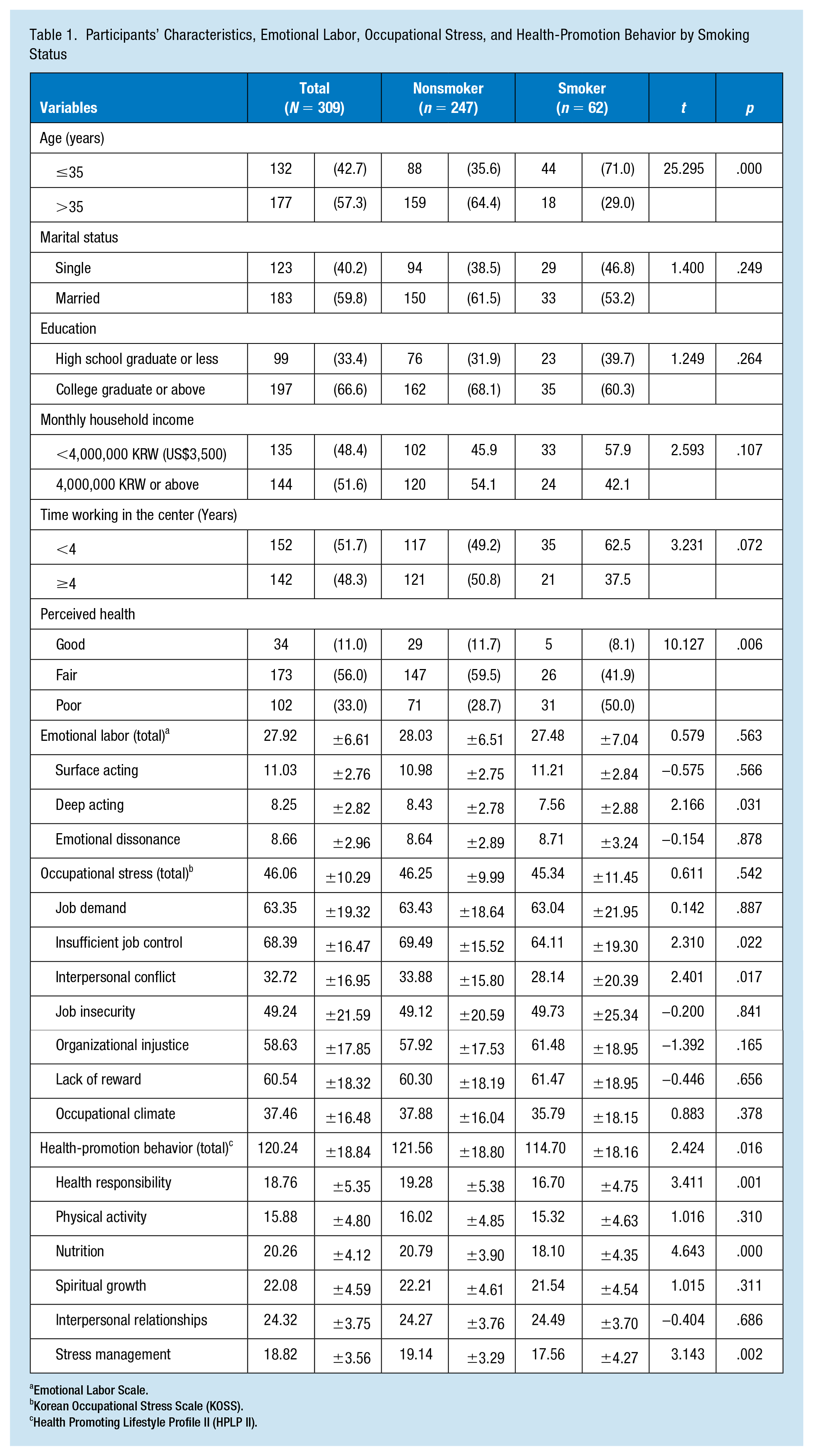
Demographic characteristics, levels of emotional labor, occupational stress, and health-promotion behavior, as well as these factors stratified by smoking status are presented in Table 1. The average age of the participants was 36.9 years (±7.7), and 57.3% were older than 35 years. About 60% of the participants were married, and 66.6% had earned college degrees.
Participants’ Characteristics, Emotional Labor, Occupational Stress, and Health-Promotion Behavior by Smoking Status
Emotional Labor Scale.
Korean Occupational Stress Scale (KOSS).
Health Promoting Lifestyle Profile II (HPLP II).
About 20% of the 309 women (n = 62) were current smokers, and they smoked an average of 9.5 cigarettes per day. The smokers were younger than the nonsmokers, and the proportion of those who perceived themselves to be poor was higher among those who smoked cigarettes (50%). Smokers had lower levels of deep acting and health-promotion behaviors in the fields of health responsibility, nutrition, and stress management than nonsmokers. Nonsmokers had higher levels of insufficient job control and interpersonal conflict than smokers.
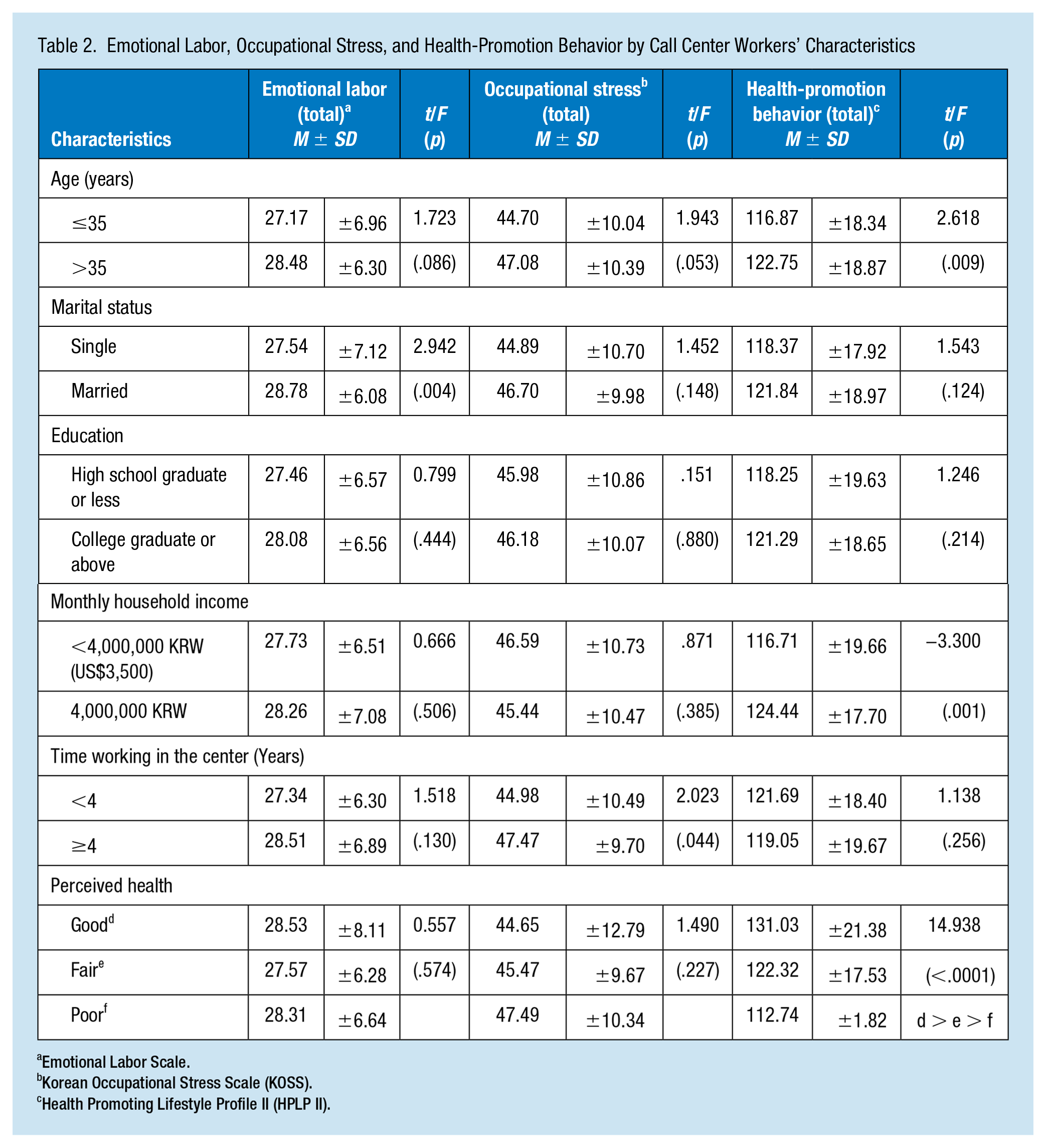
Table 2 indicates emotional labor, occupational stress, and health-promotion behavior according to participants’ characteristics. Occupational stress was higher in those working in the center for 4 or more years (t = 2.023, p = .044). Levels of health-promotion behavior were statistically different by age (t = 2.618, p = .009), monthly household income (t = −3.300, p = .001), and perceived health status (t = 14.938, p < .0001). Certain women showed higher levels of health-promotion behaviors (those who were older, had higher household incomes, and perceived their health to be good). Married women showed higher levels of emotional labor (t = 2.942, p = .044).
Emotional Labor, Occupational Stress, and Health-Promotion Behavior by Call Center Workers’ Characteristics
Emotional Labor Scale.
Korean Occupational Stress Scale (KOSS).
Health Promoting Lifestyle Profile II (HPLP II).
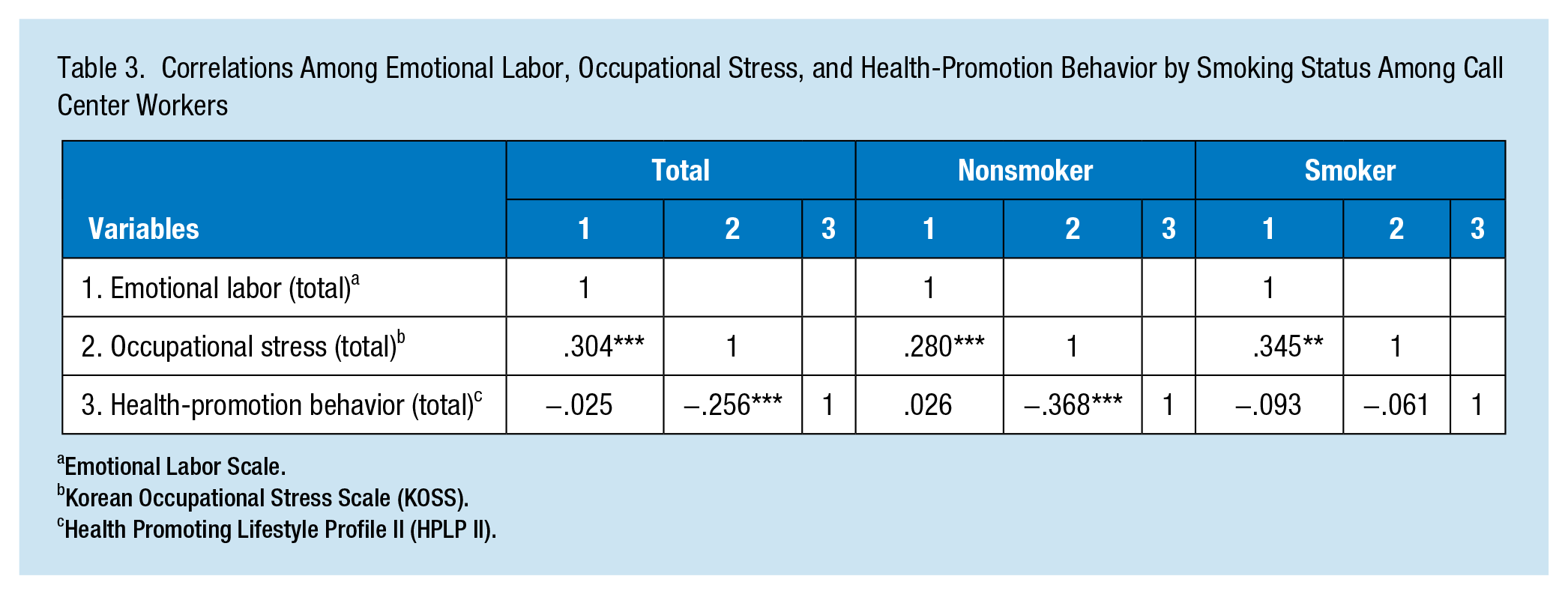
Results of the correlation analyses are summarized in Table 3. Overall, positive relationships between emotional labor and occupational stress and negative correlations between occupational stress and health-promotion behaviors were identified. When the results were stratified by smoking status, the positive relationship between emotional labor and occupational stress became stronger in smokers (r = .345) than in nonsmokers (r = .280). The negative relationship between occupational stress and health-promotion behaviors became stronger (r = −.368) in nonsmokers. Nonsmokers with higher levels of health-promotion behaviors seemed to control occupational stress through a healthy lifestyle.
Correlations Among Emotional Labor, Occupational Stress, and Health-Promotion Behavior by Smoking Status Among Call Center Workers
Emotional Labor Scale.
Korean Occupational Stress Scale (KOSS).
Health Promoting Lifestyle Profile II (HPLP II).
Discussion
Given the significant expansion of telecommunications technology, call centers, which provide customer services via telephone, have become an increasingly important part of modern business and have generated thousands of jobs. However, little attention has been paid to the effects of working in a call center on the employees’ health. Given the high prevalence of smoking among women who work in call centers in Korea, we evaluated the relationships between the women’s smoking status and their emotional labor, occupational stress, and health-promotion behaviors.
In this sample of women, about 20% were currently smokers, and the percentage was high in those who were 35 years or younger. Compared with Korean women in general, the prevalence of smoking in this sample was relatively high. Women’s trajectory of cigarette smoking with a nationally representative sample of Korean women showed that women in the age range of 20 to 30 years had the highest prevalence of smokers, that is, 12.1%; the prevalence of smoking decreased with advancing age, but the rate increased again in women older than 60 years (4.4%; Boo & Froelicher, 2012). It is suggested that this pattern of smoking prevalence in Korea is associated with the Korean culture. There is a strong social taboo against women smoking in Korea where the Confucian norm and patriarchy are prevalent (Chung, Lim, & Lee, 2010). Confucian gender norms advocating gender differences in smoking also exist in Korean culture; that is, women’s smoking, especially among women of childbearing age, has long been considered inappropriate in Korea (Chun, Doyal, Payne, Cho, & Kim, 2006). Thus, the substantial rates of cigarette smoking in this sample of 62 women working in the call center, some of whom were of childbearing age, may be attributable, at least in part, to the nature of the job.
Korea has implemented a national effort to reduce the high smoking rate by designating most workplaces as smoke-free zones. However, in most call centers, there are rooms designated for smokers. Female smokers describe call centers as “paradise” for smokers (K. Kim, 2015). When they smoke outside of their workplaces, they feel like the public views them as dirty, lower class people, but they can smoke cigarettes freely and comfortably in the smoking rooms of the call centers without feeling that there is any stigma associated with their habit (K. Kim, 2015). Thus, their work environment may cause these female smokers to smoke more cigarettes and to be reluctant to quit smoking. Female smokers are more likely to choose a call center job where smoking areas are provided and their smoking is tolerated. In addition, there may be a few women who begin to smoke cigarettes just to fit in with the culture of their workplace, thereby increasing the number of smokers in the call centers. In this study, about 16% of the smokers started smoking after they went to work for the call center (data not shown).
The prevalence of smoking in women is associated with socioeconomic status. Women who smoke are generally poor and less educated (Hiscock, Bauld, Amos, Fidler, & Munafò, 2012; Y. Kim et al., 2012). In this sample, educational status and household income were lower in smokers than nonsmokers, but the differences were not statistically significant. This may have been due, at least in part, to the fact that they were a relatively homogeneous sample and worked in the same area. Additional research may be required with larger samples to identify more accurately the association between socioeconomics and smoking behaviors in female call center employees.
The average score for deep acting was lower in smokers than in nonsmokers. Deep acting refers to the employees’ internal efforts to regulate their thoughts during their interactions with customers and to actually feel the desired emotions. Thus, deep acting may generate positive emotions. Conversely, surface acting refers to the process of just faking or suppressing emotions, thereby modifying outward expressions of emotions while leaving internal emotions unchanged (Hochschild, 1983). The scores for surface acting and emotional dissonance were higher in smokers, although the difference was not significant. This suggests that smokers may tend to temporarily fake their emotions to satisfy their customers rather trying to reappraise their feelings to align with the desired emotions. Evidence shows that surface acting, as opposed to deep acting, is strongly associated with cortisol levels that indicate stress responses (Qi et al., 2017). A recent qualitative study of female call center employees reported that they often use cigarettes as a way of alleviating the acute stress or anger they feel when dealing with aggressive customers. Sometimes, their managers, as a way of promoting productivity, even suggest that they smoke cigarettes to promptly take their mind off the stress, so they can go back to work and deal with another customer (K. Kim, 2015). Female smokers should be made aware of the adverse effects of smoking on their health, and more practical ways of reducing the negative effects of their work should be developed and made available to them.
Among the seven subscales of occupational stress, this sample reported higher scores on insufficient job control, job insecurity, and lack of reward than was observed in a nationwide random sample of general Korean employees (Chang et al., 2005). Higher scores on insufficient job control indicate that the participants do not perceive that they have enough opportunities to deal with their tasks. High scores on job insecurity and lack of reward may be because most call center employees in Korea are not regular, full-time employees who are paid based on their performance. However, their scores on interpersonal conflict and occupational climate were the lowest, even lower than among general Korean employees (Chang et al., 2005). This may be because they interact mainly with customers rather than colleagues or supervisors. An earlier study showed that approximately 88% of call center employees felt tension, and 76% experienced verbal abuse by customers while 61% indicated they had never experienced any tension with their colleagues (Croidieu et al., 2008).
Interestingly, the scores for insufficient job control and interpersonal conflict were lower for smokers than for nonsmokers. The call center where the data were collected had no places where employees could take breaks together other than the smoking room. Smokers may go there to take a break or to cultivate friendships while smoking. Additional qualitative and quantitative studies with larger samples are warranted to better understand the perspectives of female employees concerning how their job stress relates to their smoking behavior. In addition, those who had worked at the call center for more than 4 years reported higher levels of occupational stress, and this finding was consistent with the findings of previous studies (Chevalier et al., 2011; Croidieu et al., 2008). This may be because of imbalances in rewards, their seniority, and the limited career path that makes it difficult to move to other jobs.
Overall, the average score for health-promotion behaviors in this sample was 120 out of 208. Younger age, lower level of household income, being a smoker, and perceiving oneself to be in poor health were related to the lower levels of health-promotion behaviors, which was consistent with the findings of previous studies (Beşer, Bahar, & Büyükkaya, 2007; Hwang et al., 2015). The overall levels of health-promotion behavior were higher than for blue-collar workers in Korea (Hwang et al., 2015), but they were lower than for middle-aged Korean women (E. Lee, So, & Lee, 2010) or clinical nurses in Korea (H. Kim et al., 2015). Most nurses are women, and they are considered to be emotional workers as well, but nurses have been shown to be better at engaging in health-promoting behaviors than this sample of call center employees. This sample showed lower scores for all six subscales of health-promoting behaviors than clinical nurses of similar ages (H. Kim et al., 2015). Specifically, the score for spiritual growth in this sample was far lower than that for clinical nurses. Examples of items included in the spiritual growth subscale are “I expose myself to new experiences and challenges” and “I look forward to the future.” Compared with this sample, nurses may be more aware of the effects of health-promoting behaviors on positive health outcomes; thus, it seems necessary to provide educational programs to advise this sample about the importance of engaging in health-promotion behaviors.
Among the six health-promoting lifestyles, the score for physical activity was the lowest in this sample. Call center employees sit behind a desk all day, so they are generally considered to be the most sedentary at work, and sedentary lifestyles are related to adverse health outcomes, such as musculoskeletal discomfort. In fact, a previous study reported that about 78% of female call center employees complained about musculoskeletal discomfort (Lin, Chen, & Lu, 2009). Specifically, smokers had lower scores than nonsmokers on health responsibility, nutrition, and stress management, which was consistent with the findings of previous studies (Thanavaro, 2005; Thanavaro et al., 2006). As mentioned earlier, smokers may use cigarettes as a way of promptly reducing their feelings of stress or anger rather than engaging in health-promoting behaviors. In this study, smokers were more likely to perceive their health to be poor. This suggested that the smokers in this sample did not seek health advice even though they perceived that their nutrition and stress management were not sufficient and that their health was not good. Health educational programs, including stress management, should be developed and made available for call center employees in their workplaces.
Overall, positive relationships between emotional labor and occupational stress and negative correlations between occupational stress and health-promotion behaviors were identified in this sample, both of which were consistent with a previous report (Ng & Jeffery, 2003). However, when the results were stratified by smoking status, the positive relationship between emotional labor and occupational stress was stronger in smokers than in nonsmokers. The negative relationship between occupational stress and health-promotion behaviors was stronger in nonsmokers. In smokers, the relationship between occupational stress and health promotion was not statistically significant. This finding suggested that the relationships among emotional labor, occupational stress, and health-promoting behaviors may depend on smoking status. Additional studies, including multivariate or path analyses with a larger sample of call center men and women, would provide an opportunity for a more systematic evaluation of the role of smoking status in the relationships among the variables.
Study Limitations
There are several limitations that must be acknowledged to interpret the results of this study appropriately. First, the data were collected in a specific credit card call center, but the environment of call centers and the job descriptions of the employees may differ from center to center. The number of smokers was too small to conduct multivariate analyses, so further studies including larger samples would produce more generalizable results. Second, smoking status was self-reported, and, given the social taboo against smoking by women in Korea, it may not reflect the true prevalence of smoking among the women. One study showed that the smoking prevalence of Korean women measured with the objective analysis of their urine for cotinine, a metabolite of nicotine, was 5 to 6 times higher than the self-reported data (Jung-Choi, Khang, & Cho, 2012). Third, this was a cross-sectional study, so causality cannot be implied. For example, this study demonstrated that high occupational stress is related to decreased likelihood of engaging in health-promotion behaviors. Reasonably, perceived stress could discourage individuals from engaging in healthy behaviors, but it is also possible that those engaging in healthy behaviors might perceive their stress as tolerable.
Conclusion
Compared with the general population, the prevalence of smoking was strikingly high among the female employees of a call center in Korea. Such high smoking rates in the female employees of the call center may be attributable, at least in part, to the job culture of the call center. Smokers were less engaged in health-promotion behaviors than nonsmokers, especially with regard to health responsibility, nutrition, and stress management. Occupational stress is negatively associated with health-promoting behaviors in nonsmokers, but this was not the case for smokers. Smokers may use cigarettes as a way of alleviating negative emotions. Furthermore, studies with larger samples are warranted to better understand the relationship between female employees’ smoking behaviors and their job cultures.
Implications for Occupational Health Nursing Practice
National health initiatives and company policies should prioritize a nonsmoking work environment. Occupational health nurses are usually present at the place of work and have easy access to workers at the moment that they have a problem. Therefore, assessing emotional stress and providing stress management and psychosocial consultation should be the first priority for those who work with call center employees. At the same time, effort and support are required to encourage companies to implement a health education program including stress management and regular health check-ups for call center employees.
Applying Research to Practice
Applying Research to PracticeCompared to the general population (5.5% in 2015), the prevalence of smoking was strikingly high among the female employees (37%) of a call center in Korea. Those rates may be attributed, at least in part, to the job culture of the call center. Korea has implemented a national effort to reduce the high smoking rate by designating most work places as smoke-free zones. However, in most call centers in Korea, there are rooms designated for smokers. In this study, we found that call center employees who smoke were less engaged in health promotion behaviors than nonsmokers. Occupational stress was associated negatively with health-promoting behaviors in nonsmokers but not in smokers. Smokers may use cigarettes as a way of alleviating negative affections. National health initiatives and company policies should prioritize a nonsmoking work environment. At the same time, effort and support are required to encourage companies to implement a health education program including stress management and regular health checkups for call center employees.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Sunjoo Boo is an associate professor at the Ajou University. Her research focuses on emotional labor and community and occupational health.
Hyunjin Oh is an associate professor at the Gachon University. Her research interests are in workplace bullying, emotional labor, and psychosocial responses.