
Abstract
Registered nurses and midwives are in short supply and have among the highest rates of sick leave in the global workforce. The aim of this study was therefore to explore and gain a deeper understanding of how nurses and midwives experience their everyday work, with a view toward promoting and sustaining their work-related health. Nine registered nurses and four registered midwives working in hospitals and community healthcare facilities in Sweden were interviewed. The interviews were analyzed using content analysis. This study is reported in accordance with COREQ. One main category emerged: ‘Quality of organizational and collegial support and opportunities to facilitate recovery, health, and patient care’. From this category, four generic categories describing the overall experiences of registered nurses and midwives could be discerned. Based on these results, it is recommended that employers adopt a systematic health-promotive approach to foster and maintain the workplace health of registered nurses and midwives.
Introduction
Work-related health and psychosocial health problems, such as stress, are global and complex issues. 1 The challenges associated with these problems, including sick leave in the workplace, have increased in recent years. 2 This is particularly the case in Sweden, which has the highest rate of sick leave due to work-related stress among Nordic and European countries. 3 Globally speaking, gender appears to be an important indicator of work-related health status, with nurses4–6 and midwives7–9 experiencing a higher prevalence of stress and burnout. In Europe, for instance, women account for a larger proportion of sick leave, 10 and the same pattern is evident in Sweden as well. 11
Nursing is a profession devoted to providing proper care and promoting health. 12 Alongside their caring responsibilities, nurses face many types of ethical dilemmas in complex healthcare situations. 13 Globally, the number of older adults is increasing, resulting in an increasing need for long-term care. 14 This trend, however, has also been accompanied by a worsening shortage of nurses and midwives worldwide 15 , 16 and an increased rate of nurse turnover; a problem with adverse impacts on the health outcomes of both staff and patients. 17 Indeed, the World Health Organization (WHO) has estimated that by 2030, the global shortage of nurses and midwives would be 5.9 million, when compared to the staff level needed to achieve sustainable development goals. 18 Therefore, long-term strategies are needed to both improve the health of nurses and midwives and decrease their turnover rate.
Stressors may be unavoidable and can have protective effects, however, their adverse effects on human health are important to be aware of. 19 Despite such stressors, important health strategies should also be considered to counteract the nursing shortage and improve the health of nurses and midwives. These strategies include manageable workloads, small working groups, and strong leadership. 20 Similarly, manageability, comprehensibility, and meaningfulness are beneficial, perhaps even essential, factors in retaining nurses and midwives in the workplace. 21
Long-term negative stress can lead to illness and disease. 22 In the healthcare workplace, several factors (i.e. stressors) can worsen nurses’ health and exacerbate negative stress, specifically limited resources, lack of support from employers, and multiple responsibilities. 23 Similarly, occupational stress and high job demands associate with nurses’ burnout symptoms. 24 Collectively, these stressors can exert long-term, adverse effects on nurses’ physical, emotional, and psychosocial well-being. Ultimately, when these stressors are coupled with moral and emotional distress, nurses are at heightened risk of experiencing burnout,25–27 which is often associated with poor self-rated health and sleep disturbances. 28 , 29 Altogether, burnout, 27 poor working conditions, and lack of resources 30 put nurses at increased risk of leaving the profession.
A healthy workforce and decent working conditions are highlighted in United Nations Sustainable Development Goal 8: ‘Decent work and economic growth’. 31 The workplace constitutes a setting in which the support and maintenance of health should be a key consideration. 32 As mentioned above, nurses and midwives are at heightened risk of experiencing ill health and burnout in the workplace, which can often result in an increased incidence of sick leave. Despite the detrimental impacts of this phenomenon on both nurses and society at large, research on how nurses and midwives experience their health in relation to their workplace has thus far been limited. Thus, in the present study, accounts by nurses and midwives with respect to their workplace health were examined to elicit a deeper understanding of the connections between working conditions and health, with the primary goal of developing useful strategies to promote and sustain their health indefinitely.
Aim
The aim of this study was to explore and gain a deeper understanding of how nurses and midwives experience their everyday work, with a view toward promoting and sustaining their work-related health.
Method
Design
We applied a qualitative descriptive design with semi-structured interviews 33 to elicit an in-depth understanding of the workplace health of nurses and midwives via their own experiences and accounts. Qualitative designs are especially productive in this regard, as they are based on the collection and analysis of subjective or narrative data for the purpose of generating rich descriptions of complex, multi-faceted phenomena. 33 , 34 The consolidated criteria for reporting qualitative research (COREQ) were used to enhance the transparency and quality 35 of this study. In addition, the COREQ were used by the authors to reflexively account for their preconceptions and preexisting ideas about the phenomenon within the context of nurses’ and midwives’ workplace health, as well as to direct the research process from beginning to end.
Study setting and recruitment process
Data collection was performed in Sweden during spring 2018. A call for participants was announced in the professional nursing magazine of the Swedish Association of Health Professionals (Vårdfokus). Those who were interested in participating in the study contacted the first author via email for further information about the study and to schedule interviews. The data collection period ended when the interviewer (first author) determined that data saturation had been reached. All interested participants were enrolled.
Participants
In total, 13 participants were recruited and interviewed: 11 women and two men. Among them, nine were registered nurses (four of whom had a specialist education) and four were both registered nurses and registered midwives. For the sake of brevity, the simpler terms nurses and midwives will be used for the remainder of the article. Participants ranged in age from 32 to 59 years, with a mean age of 44 years. The residences of the participants varied, as did their departmental assignments, which included general and specialized hospital wards, antenatal departments, and youth clinics in hospitals and community health services. Participants’ work experience ranged from 2–31 years, with a mean of 20.5 years. To be included in the study, participants had to meet the following criteria: 1) to be employed as a nurse or midwife; 2) not to be on sick leave; 3) to work a minimum of 75 percent of full time as defined for the nursing or midwifery profession; and 4) to have a minimum of one year of work experience.
Data collection
The first author conducted the interviews between April 17 and July 13, 2018. The interviews lasted anywhere between 42 and 74 minutes. Four interviews were conducted face to face, five were conducted by telephone, and four were completed via Skype. Time and place of interview was chosen by the participants themselves and only interviewer and participant were presented. All interviews were transcribed verbatim.
Based on collaboration and consensus by the authors, an interview guide comprising open-ended questions and guided by knowledge generated from previous research and reports on the relative health status of nurses and midwives was developed. Prior clinical experiences relevant to the research focus were also incorporated into the interview guide to help fulfill the aim of the study. The first two interviews served as pilots to test the efficacy of the interview guide. The results of these interviews indicated that only minor changes needed to be made to the interview questions to facilitate more in-depth depictions of the work-related health experiences of nurses and midwives. Accordingly, these two initial interviews and their findings were included in the final analysis.
After opening questions were asked, follow-up questions were directed in such a way as to encourage nurses and midwives to freely share their workplace experiences. One example of an opening question was ‘Could you please tell me about a situation in your workplace that you experienced as having had an impact on your health?’ One example of a follow-up question was ‘Could you please describe/explain your situation/feelings in more detail as well as your reaction to them?’
Data analysis
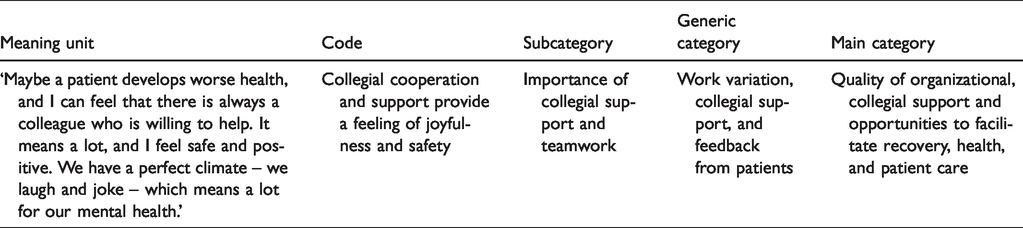
The data were inductively analyzed via qualitative content analysis 36 and consisted of three phases: preparation, organization, and reporting. In the preparation phase, the transcribed interviews were repeatedly read and reviewed in an iterative fashion with the purpose of eliciting a deeper understanding of the workplace experiences of the nurses and midwives. This phase was also used to assess the strength of the essential interview structure. In the organization phase, all statements and associated meanings with any bearing on the overall research aim were marked as analytical material. In the reporting phase, selected statements and meanings were coded and thereby described, with the code names designating the actual content of the text. The codes were subsequently grouped and then abstracted into subcategories based on similarities and differences between their content, after which they were abstracted into four generic categories. In the final abstraction stage, one main category emerged based on the underlying meanings of the subcategories. Whereas the formation of codes, subcategories, and generic categories was achieved based on clear content characteristics (i.e. the manifest level of analysis), the abstraction of the main category was based in large part on interpretation – hence, the latent level of analysis. The first author created the codes and then collaborated with the remaining authors to complete the categorization process. The created codes were first discussed among all the authors and then further developed in relation to the original text, if needed. The generation of the subcategories, generic categories, and main category was accomplished cooperatively by all authors. An example overview of the analytical process is detailed in Table 1.
Example overview of the analytical process.
Ethical considerations
The Regional Ethical Review Board in Gothenburg, Sweden, approved the study (Dnr: 1057-17). All participants gave verbal consent via telephone (recorded) and were verbally informed about the research and study process before the study began. Ethical principles were followed in accordance with the Helsinki Declaration.
Results
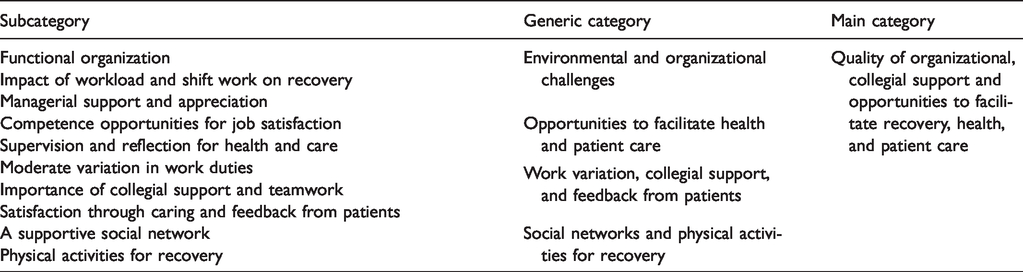
The analysis resulted in one main category with four generic categories. An overview of the categories and subcategories is presented in Table 2.
Overview of categories and subcategories.
Quality of organizational, collegial support and opportunities to facilitate recovery, health, and patient care
The main category, ‘Quality of organizational, collegial support and opportunities to facilitate recovery, health, and patient care’, represents the overall health-related experiences of nurses and midwives in their everyday work. In more detail, nurses and midwives assess their health-related experiences in terms of the quality of the organization and support they receive to address daily work-related issues and to facilitate recovery. When nurses and midwives perceived their work environment to be supportive – that is, an environment in which opportunities are available to strengthen work qualifications, social and collegial teamwork are encouraged, and strategies for recovery are effectively developed and implemented – they viewed this environment as health-promotive. In contrast, when organizational changes were detrimental, workload was overwhelming, shift work was excessive or unfulfilling, and managers (heads of department) were less supportive, nurses and midwives perceived this work environment as hindering recovery, degrading patient care, and contributing to negative stress and other adverse health effects.
Environmental and organizational challenges
The category ‘Environmental and organizational challenges’ emerged through subcategories involving the environmental and organizational health-related experiences of nurses and midwives.
Functional organization
A stable organizational structure and a present and responsive manager were viewed positively by nurses and midwives with regard to their health. Likewise, nurses and midwives experienced greater job satisfaction when personal support and valuable work-related information were available. Conversely, absent or distant managers, as well as lack of access to information critical to job performance, were perceived as detrimental to health: We have not had the same manager; this creates concern in the group. We do not have someone who looks after us, and we do not have anyone considering this issue. This problem creates a lot of dissatisfaction; you get no information, fewer social activities, fewer education days, and so on. (Nurse 2)
Impact of workload and shift work on recovery
The participants experienced high workloads, which they defined as an imbalance between the number of patients and the number of personnel, as challenging for maintaining their health. Such an imbalance was often associated with feelings of irritation, frustration, and tiredness. Lack of sufficient time, due to high workloads, to provide patients with quality care also imposed a severe psychological burden on nurses and midwives. This in turn made them less motivated to work. Excessive workload also compelled them to assume additional administrative responsibilities, such as finding a colleague to cover a shift, which was not only difficult and stressful but also obstructive in terms of patient-related work. Other deleterious effects of increased workload included multi-tasking, which frequently required prioritizing some tasks over others – no easy decision when all work tasks were perceived as equally important. Work overload was also noted by nurses and midwives as adversely impacting their health, as it often involved excessive work hours and little or no time to rest and recover between shifts. Work overload also reduced opportunities for substantive communication among colleagues, which in turn degraded collegial relationships and consequently decreased job satisfaction and damaged health: It is very stressful with a high workload … and it is like this throughout the ward. So, no one can relieve the work to help and support. Or if there have been certain tough situations with patients, for example, that you have difficulties leaving behind – then you take work home with you. It is a psychological burden. (Nurse 7) Eh … sometimes I may work an evening shift, and then I have to take the morning shift the next day. I finish working at 10 pm and start at 6:45 am. … It is challenging to come home, calm down, sleep, and then wake up again. There will not be many hours of sleep. (Nurse 7)
Managerial support and appreciation
Support and appreciation from managers were considered essential resources by nurses and midwives, as they felt they and their work were valued and acknowledged. Managerial support was considered especially important when nurses and midwives were sick or burdened with a high workload.
The participants expressed the desire for their managers to show interest in their work, provide them with feedback, and be more appreciative. They also expected to receive accurate and timely information from their managers, the absence of which was implicated in conflicts between colleagues. However, the participants often did not receive such support or guidance from their managers, which prompted feelings of frustration, disappointment, insecurity, and unimportance. Some participants also reported feeling undervalued and misjudged regarding their capacity to handle various work tasks: If the manager comes and says, ‘I see that you have had a tough day today and I just wanted to say that you are doing a fantastic job and I do what I can from my side’. Then we could feel supported … But the manager we have right now, she is uninterested. We have the feeling that we are not seen and acknowledged for the work that we have done. (Nurse 12)
Opportunities to facilitate health and patient care
The category ‘Opportunities to facilitate health and patient care’ emerged from subcategories describing experiences with respect to opportunities in the workplace that affected the participants’ health.
Competence opportunities for job satisfaction
Participants expressed the need to be competently trained in daily tasks and skills, and to be updated about the latest treatment methods. Doing so would ensure patient safety because such training would equip nurses and midwives with the proficiencies needed to manage acute and difficult situations. This was especially underscored with regard to cases in which nurses felt unsure about their capacity to assist patients safely and effectively: To make correct judgments, it is sometimes very hard. We … make mistakes, and those who work here have no formal training in telephone counseling, something that we have raised with our superiors; we need to have formal training in this to know how to handle things. And then … our colleagues actually need support between all phone calls. (Nurse 13)
Supervision and reflection for health and care
Supervision by professionals and multi-professional teams was regarded as a positive experience as well as an essential source of knowledge. It contributed to feelings of safety in the workplace and incorporated new professional perspectives. Being permitted to share their feelings during supervision allowed the participants to gather valuable insights and reflect on various patient-related events and experiences. However, there was a notable lack of professional supervision, including structured reflection, which was experienced by participants as frustrating. There were, however, opportunities for formal reflection on different work situations, which gave the participants more in-depth insights into their colleagues’ perspectives. This in turn contributed to improved health-related experiences as well as increased potential to offer better care: We need this type of learning environment to learn from each other despite the different professions we have. (Nurse 12)
Work variation, collegial support, and feedback from patients
The category ‘work variation, collegial support, and feedback from patients’ emerged from subcategories describing experiences with workplace-related factors that facilitated enhanced health and care.
Moderate variation in work duties
The participants agreed that moderate work variation, in contrast to monotonous, repetitive work routines, benefited their health. Work variation was described as working with different patient categories and completing diverse work assignments, which cultivated a greater sense of satisfaction and improved motivation to accomplish work tasks: My current job is … focused on one area with only one patient category and the same work content Monday through Friday. … When we are on call, we have the whole municipality. You have responsibility for both … psychiatric facilities and home health care, so it is extensive. One gets to do more. More work variation, and that is, I find, fun. One gets to learn and be able to apply the knowledge. (Nurse 11)
Importance of collegial support and teamwork
Participants considered colleagues’ support to be inspiring, promoting happiness and strengthening both their health and quality of care. Examples of colleague support included providing feedback and assistance when required. Positive relationships with colleagues encouraged beneficial feelings and a greater sense of safety during work, thereby cultivating a more harmonious work atmosphere; poor communication between colleagues and lack of support, on the other hand, led to feelings of weakness, sadness, and low energy. Interestingly, multi-professional teams also contributed the knowledge necessary to handle multi-dimensional problems of caring: Where I work now … teamwork has been developed very much, and they are actively focusing on this issue. Like, we have both medical doctors and paramedics on our team … on site, with the patients, on the ward all the time, which I think creates strong solidarity and fellowship and power. (Nurse 6)
Satisfaction through caring and feedback from patients
The participants described how caring for patients, particularly minimizing their pain and suffering, was greatly meaningful for them and consequently helped strengthen and promote their overall health. It was essential to them to have the capacity to provide appropriate and comprehensive care to patients, which would in turn heighten their satisfaction with their work. The participants also highlighted the fulfillment they experienced when making their patients feel safe and listening to their stories.
Social networks and physical activities for recovery
The ‘Social networks and physical activities for recovery’ category emerged from subcategories describing experiences with the factors that facilitate recovery and health.
A supportive social network
Participants regarded social support as an experience and resource crucial to their health and job satisfaction. As discussed above, they considered it important for colleagues to be open about their private and professional lives, including being forthcoming about a full range of experiences, positive or negative. Social activities both within and outside the workplace were appreciated as opportunities to become better acquainted with one another, thereby strengthening relationships between colleagues. Stable and fulfilling relationships with family and friends also helped participants to recover and improve their health: There is always someone who tries to bake something and sees a silver lining in everyday life, and yes, we treat ourselves well. We try to help each other. There is a nearby pizzeria, and we get food and eat together every Saturday, like twenty minutes, half an hour, and socialize a little and laugh, and I think that is probably the best thing. … It is so important to have a good laugh. (Nurse 3)
Physical activities for recovery
Physical activity was considered essential both in the workplace and during leisure time. Physical pursuits, such as walking and exercising, contributed to recovery from work. Some nurses expressed the need for physical activities during working hours and hoped that their employers would consider accommodating this need in support of their health. Most employers, however, did not offer such benefits in the workplace: I think it would have been very favorable [to] leave an hour earlier now and then to … do some physical exercise. The physical activity would also support mental health and make you stop thinking about work a little. … It is easier for me to relax after work when I leave earlier and go swimming and … clear my head. (Nurse 7)
Discussion
This study highlighted the work-related health experiences of nurses and midwives in order to generate a deeper understanding of which experiences best benefited their health in everyday work. Assessing these experiences may be indispensable for promoting good health and preventing poor health among nurses and midwives. The findings showed that a stable organizational structure, present and responsive managers, and a manageable workload comprising a variety of tasks all promoted and sustained the health of nurses and midwives. Furthermore, competent training in relevant care situations, as well as appropriate supervision and reflection, were considered crucial to the health of these practitioners. Additionally, collegial support and productive feedback from patients were experiences that encouraged these practitioners to continue to provide a high quality of care, while supportive social networks and opportunities to engage in physical activities accelerated their recovery from work and, consequently, improved their overall health.
The capacity of nurses and midwives to provide high-quality care depended at least in part on the support they received in their everyday work. Notably, organizations that offer competent and comprehensive training opportunities, adequate and responsive supervision, and room for reflection improve the care of patients in direct correspondence to the level of job satisfaction nurses and midwives gain from such organizational initiatives. Importantly, these results are in line with those of other research. 37 , 38 Conversely, the absence of such initiatives cultivates uncertainty, decreased motivation, and ultimately lowered job satisfaction. 39 Education opportunities and training in relevant areas is a stimulating factor that creates trust and improves the quality of care, 40 thereby ameliorating or mitigating stress among a range of health practitioners. 41 Furthermore, opportunities for adequate reflection improve clinical decision making, facilitate better understanding of patient situations, 42 and enhance the capacity to properly assess the requirements of diverse care situations. 43 That said, our results revealed that such organizational programs and associated opportunities are decidedly lacking in healthcare settings. Addressing this problem via the provision of such programs could be critical not only to improving the health of nurses and midwives but also to reducing turnover rates in accordance with the WHO’s Sustainable Development Goals for 2030. 15
Our study also showed that colleague support and effective teamwork positively impact workplace health. Indeed, earlier research has shown that teamwork and collegial support are meaningful health resources during work, especially for increasing job motivation. 44 , 45 Their absence, on the other hand, is associated with poor communication, which in turn adversely effects both health practitioners and patient care. 46 Collegial support and relaxation have positive effects on emotional regulation in the workplace. 47 Similarly, educational program results have demonstrated that high-quality teamwork improves outcomes in acute care situations. 48 Therefore, adequate collegial support, effective teamwork, and well-developed educational programs are essential health resources, as described by the WHO, 49 that can improve the health and care capabilities of nurses, midwives, and other health practitioners.
In our study, the participants regarded detrimental organizational changes, high workload, and excessive shift work as adversely impacting their health. As previous research has shown, such working conditions can culminate in high turnover rates, 50 chronic stress, sleep deprivation, poor recovery, and burnout among nurses and midwives. 51 , 52 It is therefore essential to improve work conditions in order to ensure patient care53,54 and strengthen commitment to work. 55 Resilience training programs could also be helpful in promoting recovery. 56 Intervention programs incorporating yoga, mindfulness-based stress reduction, and meditation have been shown to reduce stress levels among midwives. 57 Similarly, physical activities are associated with improved workplace health. 58 Thus, employers should consider implementing such programs.
Effective strategies are needed to reduce the adverse effects of work-related stress and provide nurses and midwives with sufficient organizational and social support, as per United Nations Sustainable Development Goal 8: ‘Decent work and economic growth’, which also includes strengthening, protecting, and promoting workers’ health. 59 Therefore, promoting and sustaining work-related health among nurses, midwives, and other health practitioners is crucial. Needless to say, health practitioners are integral to a sustainable and prosperous society. Contemporary crises, such as the current COVID-19 pandemic, not only exemplify the critical role nurses and other practitioners play in the survival of society at large but also foreground the substantial psychosocial burdens, trauma, and stress they routinely experience. 60
Methodological considerations
Qualitative content analysis was used to inductively analyze the research data, which comprised interview transcriptions. 36 The validity of content analysis is derived from repeated reflections on the data and on the author’s own subjective position during the three primary analytical phases: preparation, organization, and reporting. 61 The authors of the present study followed this protocol in tandem with guidelines set forth in the COREQ. 35
In the preparation phase, the authors collectively reflected on the design and appropriateness of the research methodology. In the organization phase, the transcribed texts were repeatedly, iteratively reviewed by the first author. The interpretations that emerged following this review were then discussed with the other authors during the creation of categories. In the reporting phase, the results were analytically presented. 61 Categories were introduced systematically and corresponded with themes as presented by the research participants. Quotations were included in this work primarily to illustrate and clarify the results. An overview of the analytical process was provided in Table 1 and was determined to be well suited for increasing transferability. 61 The credibility and reliability of the study were reinforced via the accurate presentation of the studied phenomenon. 34
The study results may be transferable to similar contexts. The demographic variations among the participants, including age differences, distinct cultural identities, various levels of education, diverse work experiences, and multiple locations nationwide, helped eliminate the potential for bias in the findings by deliberately assembling a variety of divergent experiences for analytical purposes. Including younger participants with correspondingly briefer work experience may have further enhanced such variation but would have come at the expense of representativeness, as our sample of nurses and midwives was an approximate microcosm of gender distribution (88% are women), age range (60% are between 40 and 59 years old), and mean experience (13 years) in Sweden. 62 To avoid bias based on younger age and less work experience, only participants with a minimum of one year of work experience were included. The intention here was to assess whether older participants with more extensive work experiences indeed experienced a lower incidence of burnout. 63 , 64 This notion is based on the assumption that older and more experienced nurses and midwives often possess more developed and resilient coping strategies. In this respect, then, the experiences and views of the participants as described in this study may be useful for implementing such coping strategies more widely among both younger and older health practitioners.
Conclusion
Employers should provide effective support systems and well-informed strategies to promote and sustain the health and job satisfaction of nurses and midwives. Moreover, a systematic health-promotive approach should be adopted, one which offers competence and skills training, productive supervision and reflection, a supportive and personable work environment, and a more balanced workload.
Footnotes
Acknowledgments
The authors are grateful to all the participants for their valuable contributions to this study. We acknowledge Dr. Rune Svanström at the University of Skövde for his support during the ethical application process, as well as the support of Dr. Karin Axelsson at the University of Skövde. Additionally, we acknowledge the support of Scribendi Inc. (Chatham ON, Canada) for the professional language editing and proofreading of this work. We are also grateful to the Swedish Association of Health Professionals for publishing our call for participant recruitment in their magazine.
Author contributions
The first author collected the data, transcribed the interviews, and was largely responsible for the analysis. All authors contributed equally to the analytical process, as well as to writing and finalizing the manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was funded by internal research grants from the School of Health Sciences, University of Skövde, Sweden.