
Abstract
In the nursing context, structural empowerment has proved to be an organizational tool leading to the prevention of stress and burnout. Structural empowerment is defined as the perception of the presence or absence of empowering conditions in the workplace. However, few studies have explored the particular relationships between power in organizations, structural empowerment, and burnout. The aim of this study was to examine the mediator role of structural empowerment (access to opportunities, information, support, and resources) in the relationship between formal and informal power, and core burnout among Portuguese nurses. We administered a questionnaire among a convenience sample of 304 nurses employed in public hospitals. Model fit and mediation analysis were conducted using path analysis and bootstrapping methods. Formal power, informal power, access to opportunities, and access to resources were significant and negative predictors of core burnout. Opportunities, resources, and informal power had a direct influence on core burnout. Formal power and informal power showed an indirect influence, mediated by opportunities and resources, on core burnout. These findings suggest that by providing nurses with high levels of formal and informal power, as well as access to resources and opportunities, their risk of core burnout can be lowered.
Introduction
In recent years, nurses have been identified as one of the health professions with the highest risk of burnout at work (Bilal & Ahmed, 2017; Fragoso et al., 2016). In many countries, nurses are facing higher job demands with fewer resources in the workplace (i.e., cuts in the hiring of new nurses), coupled by the characteristics of nursing work (i.e., night and shift works, frequent contact with disease and death), that make these professionals especially vulnerable to situations of high stress and professional burnout (Buchan, O’May, & Dussault, 2013; Nowrouzi et al., 2015).
Burnout is a psychological syndrome that involves a prolonged response to chronic stressors at work, characterized by three dimensions including exhaustion, depersonalization, and inefficacy (Maslach, Schaufeli, & Leiter, 2001). Exhaustion refers to feeling overloaded and lacking emotional and physical resources (e.g., “I am overloaded at work”). Depersonalization refers to a negative, insensitive, or excessively apathetic response to various aspects of work, especially in interpersonal relationships (e.g., “I do not care about my patients”). Inefficacy refers to the feelings of incompetence and lack of achievements and productivity at work (e.g., “Perhaps this profession is not for me”). High levels of burnout are associated with physical and psychological health problems (i.e., cardiac pathology, depression, anxiety) in nursing staff (Maslach et al., 2001; Nowrouzi et al., 2015).
The structural empowerment model, based on Kanter’s theory of power in organizations, is a useful framework for understanding and conceptualizing antecedents of burnout in nursing staff (Connolly, Jacobs, & Scott, 2018; Dinapoli, O’Flaherty, Musil, Clavelle, & Fitzpatrick, 2016; Laschinger, Wilk, Cho, & Greco, 2009; Li, Kuo, Huang, Lo, & Wang, 2013; Meng, Jin, & Guo, 2016; Zhang, Ye, & Li, 2018). Kanter (1993) indicates that work behaviors and attitudes are the result of the characteristics of the work environment and not of any type of predisposition or personality traits. Nurses feel empowered when their workplace offers them “power” to achieve goals and opportunities for personal and professional development. According to Kanter (1993), “power” is the “ability to mobilize resources to get things done” (p. 210), making a distinction between formal and informal power in organizations.
Formal power refers to the characteristics of work and the health organization related to visibility, discretion, or flexibility in how work is accomplished, and impact on the overall purpose of the health units. Informal power is related to positive relationships between colleagues, head nurses, and other health professionals (e.g., physicians). Both formal and informal power facilitate access to the conditions for work effectiveness or structural empowerment (Kanter, 1993; Laschinger, Finegan, Shamian, & Wilk, 2001): access to opportunities, information, support, and resources.
Access to opportunities refers to the possibility of professional growth and movement within the health organization as well as the opportunity to increase knowledge and skills. Access to information refers to the formal and informal knowledge necessary to be effective in the workplace (e.g., indicators of quality nursing care). Access to support consists of receiving feedback, guidance, and advice from colleagues, nursing managers, and other health professionals. Finally, access to resources refers to one’s ability to acquire the materials, time, means, and supplies required to do the work.
Several studies have shown positive relationships between structural empowerment and job satisfaction (Li et al., 2013), organizational commitment (Meng et al., 2015), and job performance and innovation (Laschinger et al., 2009), and negative relationships between structural empowerment and stress and burnout (Guo et al., 2016; Harwood, Ridley, Wilson, & Spence Laschinger, 2010; Laschinger et al., 2001; Meng et al., 2016; Meng et al., 2015; O’Brien, 2011; Zhang et al., 2018). When formal and informal power levels are low in health organizations, nurses cannot access to the opportunities, resources, information, and support necessary to face job demands. As a result, nurses are not psychologically empowered and cannot cope with work demands, experiencing higher levels of stress. If these levels of stress are maintained over time, nurses may experience professional burnout situations (Guo et al., 2016; Harwood et al., 2010; Meng et al., 2016; O’Brien, 2011; Zhang et al., 2018).
Numerous studies have analyzed the relationships between structural empowerment and burnout (Guo et al., 2016; Harwood et al., 2010; Meng et al., 2016; O’Brien, 2011; Zhang et al., 2018); however, most studies have used a general measure of structural empowerment, composed of the sum of the scores of access to opportunities, resources, information, and support. It is necessary to explore specifically which of the four dimensions of structural empowerment has greater influence on nurses’ burnout, because it will allow the design of interventions adapted to this professional group (Nowrouzi et al., 2015). On the contrary, few studies test Kanter’s power theory in health organizations as a whole, that is, the relationships between formal power, informal power, the four dimensions of structural empowerment and burnout. Finally, there were few studies with samples of nursing staff from Portugal that substantiate the relationships between power, structural empowerment, and burnout observed in samples from other countries. Therefore, the aim of this study was to analyze the mediator role of structural empowerment (access to opportunities, information, support, and resources) on the relationships between formal power and informal power, and core burnout among Portuguese’s nurses (Figure 1).
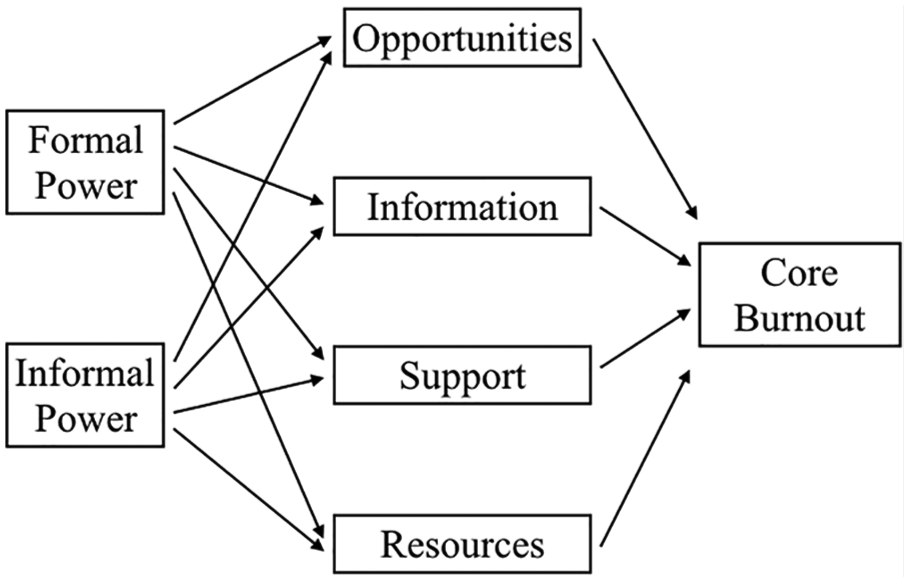
Hypothesized model of mediating factors of structural empowerment on the relationship between formal and informal power with core burnout.
Method
Study Design and Participants
A cross-sectional, descriptive study using questionnaires was conducted. A convenience sample of 492 nurses employed in two public hospitals from the south of Portugal were surveyed. Nurses were eligible for participation if they worked for at least one year in the same ward in a public hospital. The managers of the hospitals were contacted through the Regional Health Administration of the Algarve (Portugal). After a meeting with the directors and head nurses of each hospital where the objectives of the study were presented, an email was sent to the nurses of all the units of the hospitals requesting participation in the investigation.
The researchers visited the units of the public hospitals and requested the participation of nursing staff who met the inclusion criteria. The researchers explained the aim to the study and the questionnaires were given to the nurses who agreed to participate. The questionnaires were completed during their daily team meetings and in the presence of the researchers, to resolve any doubts that might arise. Confidentiality was assured. The completed questionnaires were returned in sealed envelopes. This study received human subjects from the board (Ethical Approval No. 257—Regional Health Administration of the Algarve—Portugal).
Instruments
Structural empowerment was measured using the Portuguese version (Orgambídez, Gonçalves, Santos, Mendoza, & Borrego, 2015) of the Conditions for Work Effectiveness Questionnaire-II (CWEQ-II; Laschinger et al., 2004). The 12-item scale was composed of four dimensions: access to opportunities (e.g., “The chance of gain new skills and knowledge on the job”), information (e.g., “The current state of the hospital”), support (e.g., “Specific information about things you do well”), and resources (e.g., “Time available to accomplish job requirements”). The items were rated on a 5-point Likert-type scale ranging from 1 (none) to 5 (a lot). The coefficients of reliability (Cronbach’s alpha) obtained in this study were .84, .88, .86, and .77 for access to opportunities, information, support, and resources, respectively.
Formal power was measured using three items from the Portuguese version (Orgambídez et al., 2015) of the Job Activities Scale (JAS; Laschinger, Finegan, Shamian, & Wilk, 2004). A sample item is “The amount of visibility of my work related activities within the institution.” Participants indicated their response using a 5-point Likert-type scale from 1 (none) to 5 (a lot). The Cronbach’s alpha reliability coefficient obtained in the present study was .78.
Informal power was assessed using four items from the Portuguese version (Orgambídez et al., 2015) of the Organizational Relationships Scale (ORS; Laschinger et al., 2004). A sample item is “Collaborating on patient care with physicians.” The items were rated on a 5-point scale from 1 (none) to 5 (a lot). The Cronbach’s alpha reliability coefficient observed in this study was .79.
Core burnout was measured using the Portuguese version (Melo, Gomes, & Cruz, 1999) of the Maslach Burnout Inventory (MBI; Maslach & Jackson, 1986), considering the means of emotional exhaustion (nine items, e.g., “I feel emotionally drained from my work”) and depersonalization (five items, e.g., “I don’t really care what happens to some patients”). According to Maslach et al. (2001), emotional exhaustion and depersonalization are considered as core aspects of burnout or core burnout. Participants indicated their response using a 7-point Likert-type scale from 0 (never) to 6 (always). The Cronbach’s alpha reliability coefficient in this study was .86.
Data Analysis
The statistical package STATA v.13 was utilized to check the proposed goal of the study. The possible influence of the common method variance (CMV) on the data was tested using Harman’s test (Podsakoff, MacKenzie, Lee, & Podsakoff, 2003). When all the data are collected by self-reports measures at the same time, the common variance related to the method may underestimate or overestimate the relations between variables (Podsakoff et al., 2003; Podsakoff, MacKenzie, & Podsakoff, 2012). To carry out Harman’s test, all items of structural empowerment, formal power, informal power, and core burnout were subjected to exploratory factor analysis (EFA), using the principal component method with varimax rotation and forcing the extraction of a single factor. Prior to the EFA, Bartlett’s test of sphericity produced a significant chi-square, χ2(595) = 5145.85, p < .01, and the measure of the sample adequacy (Kaiser–Meyer–Olkin measure) was equal to 0.91, indicating that the correlation matrix was appropriate for conducting EFA.
If there was an issue of CMV, the extracted factor should account for over 50% of the variance. The results showed a factor that explained 25.07% of the variance. Although the effect of CMV could not be discarded, it did not seem to significantly affect the relationships between the variables of the study (Podsakoff et al., 2003; Podsakoff et al., 2012).
Confirmatory factor analyses (CFA) were carried out to demonstrate the construct validity of the measures (Table 1). To test the distinctiveness of the measures, two CFAs were estimated: Model 1 (M1), composed of seven factors (formal power, informal power, opportunities, resources, information, support, and core burnout) and Model 2 (M2), in which all items shared only one factor. Model 1, which indicates the existence of seven different variables from each other, showed a better fit compared with Model 2, which indicates no distinctiveness of the measures, according to the recommendations of Kline (2016): comparative fit index (CFI) and Tucker–Lewis index (TLI) values close to 0.95, root mean square error of approximation (RMSEA) and standardized root mean square residual (SRMR) less than 0.08, and the smallest value of Akaike information criterion (AIC). In this sense, CFAs support the distinctiveness of the measures used in this study.
Discriminant Validity of the Constructs of Formal Power, Informal Power, and Structural Empowerment Related to Core Burnout
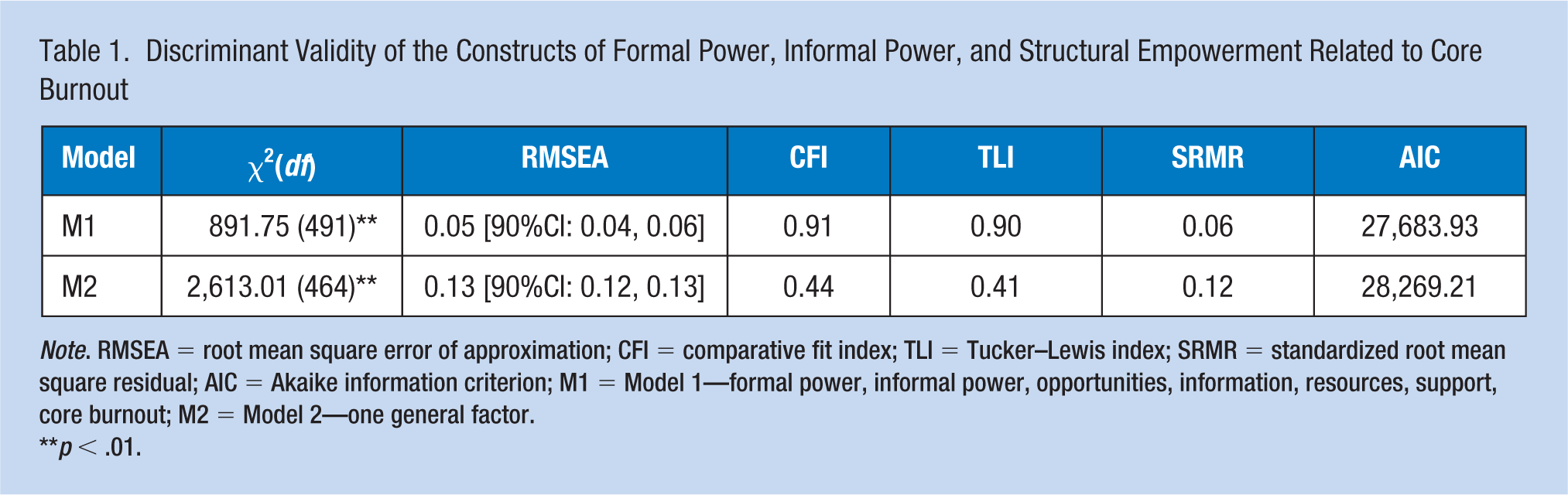
Note. RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker–Lewis index; SRMR = standardized root mean square residual; AIC = Akaike information criterion; M1 = Model 1—formal power, informal power, opportunities, information, resources, support, core burnout; M2 = Model 2—one general factor.
p < .01.
Descriptive analyses (mean, standard deviation, skewness, kurtosis) and the internal consistency (Cronbach’s alpha) of the scales were studied, in addition to the correlations (Pearson’s coefficient) between structural empowerment, formal power, informal power, and core burnout.
The relations shown in Figure 1 were assessed using the path analysis technique with the maximum likelihood method. The variables in the model were the scores obtained in the test and, therefore, fallible measurements that contained errors (Acock, 2013). According to Acock (2013), the analysis can be carried out following two steps: (a) the design of an overidentified model; and (b) the redesign of the model from the significant coefficients found in the previous step.
To test the mediator role of structural empowerment, we used the bootstrapping method to obtain bootstrap estimates of the indirect effects based on 10,000 samples. According to Hayes (2013), this method has more power than Sobel’s test and the Baron and Kenny approach. Bootstrapping provide a confidence interval (CI) for the indirect effect and make inferences based on this interval (Falk & Biesanz, 2016). If the resulting CI for the estimate does not include zero, it may be concluded that the indirect effect is significant at the α = .05 level. Because of its good performance and statistical power, bias-corrected (BC) bootstrap CIs (95%), based on 10,000 samples, were used to analyze the indirect effects.
Results
Sample Characteristics
The final sample consisted of 304 usable questionnaires (61.79% response rate). The age of the participants ranged from 21 to 56 years old with an average age of 34.23 (SD = 5.21). More than half of the nurses (n = 193, 63.49%) were women. In terms of marital status, 55.92% were married and 31.89% single. Most of the nurses were working shift work (60.25%), and the average years of professional experience of the sample was 11.34 (SD = 9.03).
Descriptive Statistics and Correlations
In general, the participants did not perceive their workplace to be particularly motivating in terms of structural empowerment. The nurses felt that they had more informal power (M = 3.60, SD = 0.71) than formal power (M = 2.66, SD = 0.79) in their organizations (Table 2). The means of structural empowerment ranged from 3.86 (access to opportunities) to 2.90 (access to resources). With respect to core burnout, the nurses exhibited low levels in this variable (M = 1.71, SD = 1.00).
Reliability Coefficients and Correlations of Formal and Informal Power, Structural Empowerment, and Core Burnout (N = 304)

Note. Alpha reliabilities are shown on the diagonal. All coefficients are significant (p < .01).
The two types of power were negatively and significantly (p < .01) related to core burnout: r = –.24 for formal power and r = –.36 for informal power (Table 2). All the dimensions of structural empowerment showed a negative and significant (p < .01) relationship with core burnout, with Pearson’s r coefficients ranging from –.19 (access to support) to –.49 (access to resources).
Mediation Analysis
Figure 2 illustrates the standardized coefficients and significance levels obtained, as well as the values of the explained variance (R2) in the dimensions of structural empowerment and core burnout. Path analysis revealed that the adjustment was good: χ2(2) = 1.44, p = .49, with CFI = TLI = 1.00, that is, over 0.95 as recommended by Kline (2016). The value of the SRMR coefficient was 0.01 and the value of the RMSEA coefficient was 0.00 [90% CI: 0.00, 0.10], that is, below the value of 0.08 as indicated by Kline (2016). The total of the core burnout variance explained by the final model was 21%.
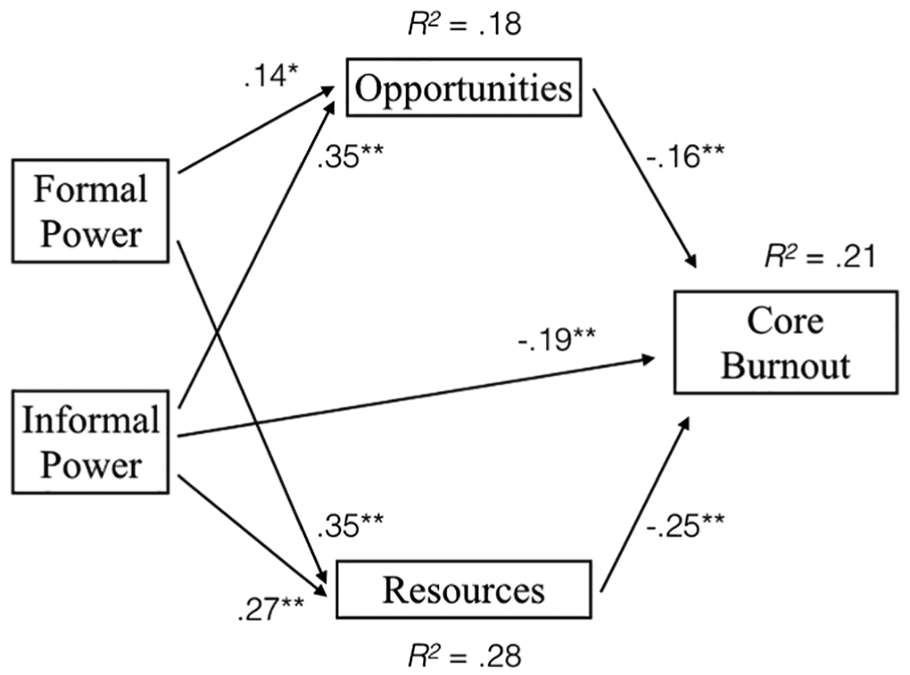
Standardized path estimates of the final model examining mediating factors of structural empowerment on the relationship between formal and informal power with core burnout (N = 304).
Table 3 shows the direct, indirect, and total effects of formal power, informal power, access to opportunities, and access to resources on core burnout. It is worth noting that, except for access to information and access to support, the rest of structural empowerment dimensions negatively and significantly predicted core burnout (p < .01) (Table 3). The influence of access to resources and access to opportunities was direct and negative on core burnout, with bootstrap coefficients of −0.16 and −0.25, respectively.
Direct, Indirect and Total Effects of Formal Power, Informal Power, Access to Resources and Access to Opportunities on Core Burnout Among Hospital Staff Nurses (N = 304)
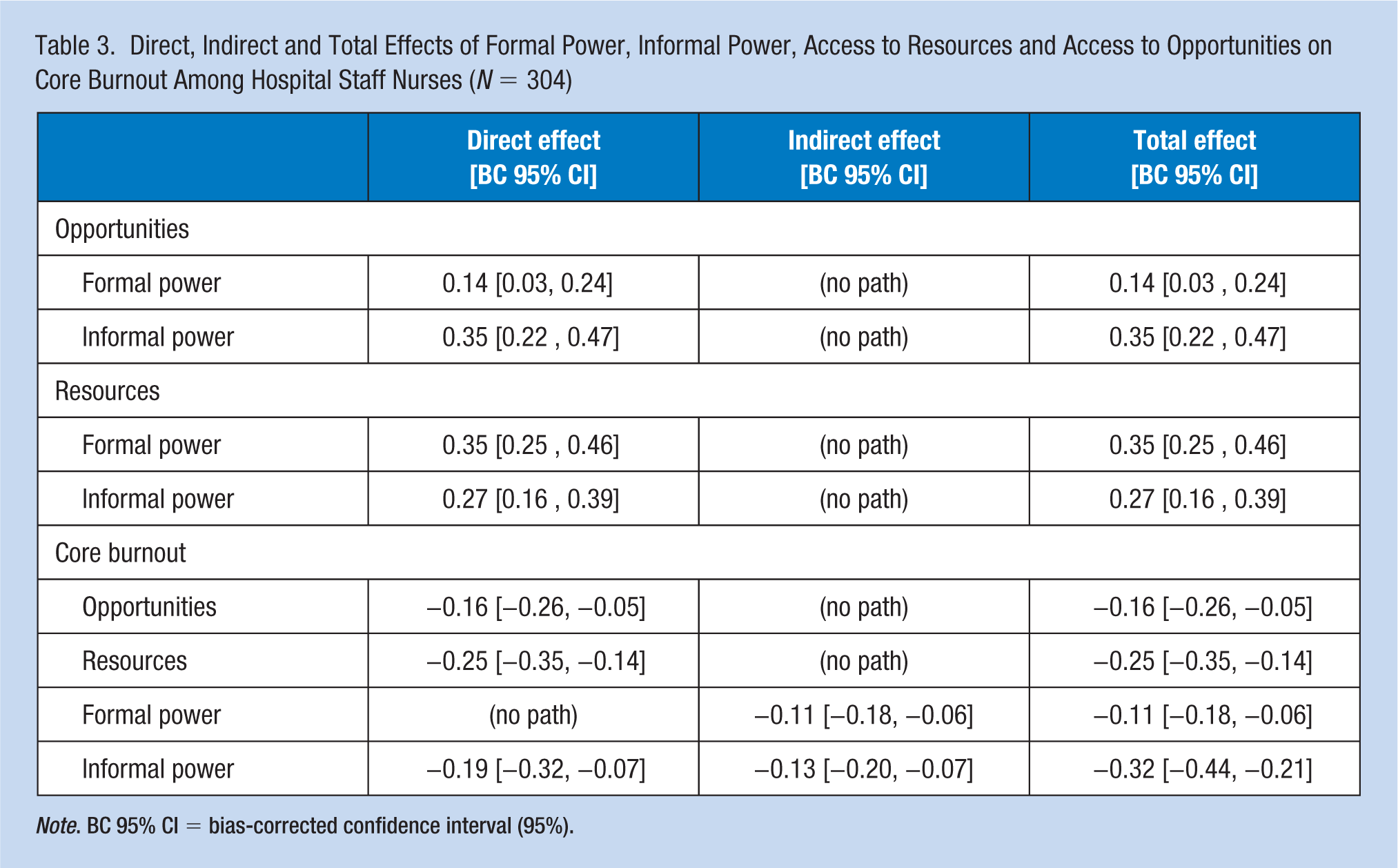
Note. BC 95% CI = bias-corrected confidence interval (95%).
Regarding formal power, its influence on core burnout was indirect, that is, formal power had a negative impact on core burnout through access to opportunities and resources. The observed bootstrap coefficient was negative (−0.11) and significant, because zero is not in the calculated interval [BC 95% CI: −0.18 – −0.06].
Informal power showed a direct and negative influence (−0.19) on core burnout and an indirect influence through access to opportunities and resources. The indirect bootstrap coefficient was negative (−0.13) and significant, because the zero is not in the calculated interval [BC 95% CI: −0.20 – −0.07]. About 59.37% of the effect of informal power on core burnout was direct (−0.19/−0.32), whereas 40.63% was indirect (−0.13/−0.32).
Discussion
The results of the study show the relationships between power in organizations, access to conditions for effective work (opportunities, information, resources, support), and burnout experienced by nursing staff. Of the four dimensions of structural empowerment, only access to opportunities and access to resources were significant predictors of core burnout. The influence of formal power on core burnout was indirect and totally mediated by access to resources and opportunities. Regarding informal power, this type of power had both a direct impact and an indirect impact, mediated by access to opportunities and resources, on the core aspects of burnout syndrome.
Workplace environments with high levels of formal and informal power create the necessary conditions for the emergence of empowering contexts for nurses (Harwood et al., 2010; Kanter, 1993; Laschinger et al., 2001; Meng et al., 2015; Zhang et al., 2018). When these sources of power are available, power is “on” and effective work is possible (Laschinger et al., 2004). Hospitals with high formal power are those in which the work performed by nursing staff is highly visible and recognized by the hospital management, and administrators allow the autonomy, participation, and decision making of nurses in task management (e.g., goals and organizational objectives). A high informal power is the result of cooperation and positive interpersonal relations between colleagues, head nurses, other health professionals, and administrators. When levels of formal and informal power are high, nurses have access to opportunities and resources necessary to be effective at work and perform their professional tasks (Kanter, 1993; Laschinger et al., 2001, 2004).
Nurses who feel that their work context allows them access to these factors are empowered. Empowered nurses are more capable of facing situations with high job demands (e.g., an excessive number of patients) and perceive that they have more control in the workplace. As a consequence, they fulfill their professional role in a meaningful way and they are effective in their work, experiencing lower levels of stress and associated burnout (Guo et al., 2016; Zhang et al., 2018). The negative influence of structural empowerment on burnout registered in the study has been observed in several studies with samples of nurses from different countries (Guo et al., 2016; Harwood et al., 2010; Meng et al., 2016; O’Brien, 2011; Zhang et al., 2018).
Informal power also showed a direct influence on core burnout in this sample of nurses. When the hospital management and administrators facilitate the establishment of networks and positive interpersonal relationships between nurses and other health professionals, there is an increase in information, advice, and guidance that help nurses to perform adequately work, perceiving higher levels of support social at work (e.g., emotional support). Social support has a direct effect on burnout, reducing its effects and negative consequences (Elst et al., 2016).
Although the fit of the explanatory model was adequate, the percentage of core burnout explained was relatively small. A variable related to structural empowerment that could explain much more variance of the core burnout is psychological empowerment (Spreitzer, 1995), which was not assessed in this study. Psychological empowerment is a cognitive state which makes employees have confidence in achieving targets successfully. According to Laschinger et al. (2001, 2004), psychological empowerment represents a reaction of nurses to structural empowerment and is considered as a mediator between structural empowerment and burnout (Guo et al., 2016; Meng et al., 2016; Zhang et al., 2018). Higher levels of structural empowerment generate higher perceptions of psychological empowerment, which reduces the presence of emotional exhaustion and depersonalization in nursing staff.
It should be noted that access to information and access to support were not significant predictors of burnout. In the case of access to support, informal power directly generates social support that negatively affects burnout, without needing to be mediated (Elst et al., 2016). In the case of access to information, its effect on burnout may be mediated by third variables (e.g., psychological empowerment) not assessed in this investigation (Peng et al., 2013; Zhang et al., 2018).
The present study had some limitations which must be considered. First, the cross-sectional design did not allow causal relationships to be established. In this sense, the empirical literature of the structural empowerment model suggests that they are correlated (Kanter, 1993; Laschinger et al., 2001, 2004). Second, the data were collected through self-reported measures which can be sensitive to certain types of bias (i.e., social desirability; Lang & Sesic, 2006). The generalizability of the study may be limited because a convenience sample was used. In addition, there may be covariates that we did not evaluate which may affect the relationships between the study variables, such as psychological empowerment (Peng et al., 2013; Zhang et al., 2018).
Implications for Occupational Health Nursing Practice
This study found that the characteristics of the organization where the nurse works may be one of the most effective structural factors that lower burnout. Providing nurses with workplaces with high levels of formal and informal power, as well as access to resources and opportunities, can lower their levels of core burnout. In this sense, the presence of power or the ability to mobilize resources to “get things done” seems to prevent high levels of burnout in nursing staff (Kanter, 1993; Laschinger et al., 2004). Given the influence of formal and informal power on the core burnout of nursing staff, directors and occupational health nurses can address these issues by fostering the participation of all nursing professionals (e.g., committees, health circles) in the decision making on various aspects of the organization (e.g., goals and organizational objectives, training plans, holidays, etc.), developing more efficient and reasonable work plans and increasing nurses’ autonomy in the workplace. Occupational health nurses can also provide nurses training on social skills (e.g., giving support) and conflict resolution (e.g., avoiding the use of derogatory language) to help foster positive interactions and relations between nurses, other health professionals, and managers (Nowrouzi et al., 2015).
Applying Research to Practice
Power or the ability to mobilize resources to get things done is one of the most effective structural factors that lower burnout in health organizations. In this sense, nurses feel empowered when their workplace offers them “power” to achieve goals and opportunities for professional development. Formal and informal power, through access to opportunities and resources, can lower nurses’ levels of core burnout. Consequently, health managers should foster the participation of all nursing professionals in the decision making on various aspects of the organization (e.g., training plans, holidays) to increase formal power in the organization. In addition, occupational health nurses should provide training on social skills and conflict resolution to nurses in order to increase formal power.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Alejandro Orgambídez, PhD, is assistant professor, Department of Social Psychology, School of Psychology, University of Malaga (Spain). His research interests are focused on work life quality of nurses.
Helena Almeida, PhD, is assistant professor, School of Economics, University of Algarve (Portugal). Her research interests are focused on management of human resources in nursing.