
Abstract
The impact of shift work on sleep and health has been examined in the past, but most studies utilized cross-sectional designs relying on between-subject differences. The purpose this study was to examine the within-subject differences in self-report measures of health and wellness among a group of nurses engaged in rotating shifts. Patient-Reported Outcomes Measurement Information System (PROMIS) measures, collected post-day and post-night shift, were used to assess health, sleep disturbances and sleep-related impairment, fatigue, emotional distress (anger), satisfaction with social roles outside of work, and applied cognitive abilities. Among the sample of 23 White, mostly female (91.3%) nurses, all PROMIS measures were worse indicting lower health and wellness after working night shifts compare to after working day shifts (p values from .167 to < .001). During both time points of assessment, sleep-related impairment was highly correlated with greater emotional distress, greater fatigue, and worse memory and concentration. Study findings support prior studies that shift work can negatively impact health and wellness.
Introduction
It is estimated that over 15% of the United States workforce engages in shift work, defined as working evening, night, earlier morning, or rotating shifts (Wright, Bogan, & Wyatt, 2013). Shift work can result in circadian disruptions that are associated with cardiometabolic diseases, cancers, gastrointestinal health issues, and the worsening of mood disorders and depressive symptoms (Davila et al., 2010; Gu et al., 2015; Karlsson, Alfredsson, & Knutsson, 2005; Morrissette, 2013). In addition to these negative health consequences, shift work is associated with road and workplace accidents (Culpepper, 2010; Gold et al., 1992; Scott et al., 2007).
Working night shift disrupts the timing and amount of food intake and is associated with a preference for high-fat foods. This negatively affects energy balance while impairing glucose tolerance and insulin sensitivity (Cain, Filtness, Phillips, & Anderson, 2015; Depner, Stothard, & Wright, 2014). For example, Davila and colleagues (2010) found that among transportation workers, those rotating shifts were up to 30% more likely to have impaired glucose metabolism, measured with HbA1c levels, and 70% more likely to have metabolic syndrome compared to those not rotating shifts. There is significant evidence from epidemiological studies that long-term shift work is associated with higher mortality from diabetes, cardiovascular disease, and stroke (Gu et al., 2015; Karlsson et al., 2005; Morrissette, 2013).
Numerous studies and meta-analyses support a dose-response relationship between night shift and cancers, specifically breast cancer in females (Leonardi et al., 2012; Lin et al., 2015), prostate cancer in males (Rao, Yu, Bai, Zheng, & Xie, 2015; Sigurdardottir et al., 2012), and colorectal cancer in both men and women (Sigurdardottir et al., 2012). Similarly, there is growing evidence supporting shift work’s negative impact on gastrointestinal health. Shift work has been linked with an increased risk for peptic ulcer disease, gastroesophageal reflux disease, inflammatory bowel disease, and irritable bowel syndrome (Knutsson & Bøggild, 2010; Konturek, Brzozowski, & Konturek, 2011; Morrissette, 2013). In addition, shift work is associated with depressive symptoms and may exacerbate symptoms in individuals with a history of depression and mood disorders (Culpepper, 2010; Krystal, Roth, & Simon, 2011; Morrissette, 2013).
Shift work has been found to negatively affect sleep. For example, Gold and colleagues (1992) found that night-shift nurses had 1.8 (95% confidence interval [CI]: 1.02, 3.22) greater odds for poor sleep quality compared to nurses that worked strict day- and evening-shift. Short sleep duration, defined as total sleep time (TST) < 6 hr per night, is common among individuals working night shift (Akerstedt & Wright, 2009; Scott et al., 2007). Data from the National Health Interview Survey shows that 52.3% of health care providers working the night shift had short sleep duration compared to 28.9% of day-shift workers (Centers for Disease Control and Prevention, 2012). Objective measurements of the sleep of rotating-shift workers showed that sleep during the day is up to 4 hr shorter than sleep during the night (Akerstedt & Wright, 2009).
The excessive sleepiness and impaired driving performance resulting from shift work increases the risk of motor vehicle crashes by two to four times during the commute to and from work (Barger, Lockley, Rajaratnam, & Landrigan, 2009; Gold et al., 1992; Scott et al., 2007). With excessive sleepiness, concentration and work performance is impaired. A third of nurses working rotating shifts or permanent nights reported falling asleep during their night shift at least once a week (Gold et al., 1992).
The purpose of this repeated-measures study of intensive care unit (ICU) nurses engaged in rotating shifts was to (a) describe the post-day shift and post-night shift correlations between various Patient-Reported Outcomes Measurement Information System (PROMIS) measures of health and wellness and (b) examine the within-subject differences in these self-reported measures after working night shifts compared to after working day shifts. More specifically, we hypothesized that (a) PROMIS scores would be highly correlated with similar findings post-day shift and post-night shift and (b) nurses would report better outcomes (i.e., few sleep-related impartments, less fatigue, more satisfaction with social roles, etc.) when working day shift compared to working night shift. In addition, in a subsample of participants, the differences in self-reported sleep characteristics before day shifts, before night shifts, and before days off were examined.
Method
The purpose of this single group, repeated measures study was to explore the within-subject differences in self-reported health and wellness among a sample of ICU nurses engage in shift work. The study included two sessions, in which the nurses completed surveys, that occurred immediately after working either three consecutive 12-hr day shifts or three consecutive 12-hr night shifts. The sessions took place approximately 2 weeks apart. All study protocols were approved by the Institutional Review Board of the University of Pittsburgh prior to implementation.
Setting and Sample
Nurses were recruited from six intensive care units (ICUs) in UPMC Presbyterian Hospital in Pittsburgh, PA. Potential participants were informed about the study through an email from their nurse managers and through fliers placed in the ICU break rooms. The recruitment materials included information about the study and the Principal Investigator’s contact information. In addition, the emails included a link to an online screening survey and the fliers included a quick response (QR) code that linked to the same survey. When the potential participant accessed the survey via the email link or the QR code, the online screening then occurred in two phases. The phase one inclusion criteria included (a) the nurse being between the ages of 18 to 65 years old, (b) the nurse worked rotating shifts (at least three consecutive day shifts followed by at least three consecutive night shifts), and (c) the nurse being able to speak, read, and write English. If eligible based on the phase one screening questions, the potential participant was asked to provide his or her contact information. During the second phase of screening, the potential participant was contacted and the second phase screening questions were administered. The phase two exclusion criteria included (a) regular use of medications by the nurse that affected sleep, (b) the nurse having had a history of or diagnosis of a sleep disorder (i.e., obstructive sleep apnea, restless leg syndrome), (c) “at risk” or “heavy” alcohol consumption (i.e., > 4 drinks on any day and > 14 drinks per week for males, and > 3 drinks on any day and > 7 per week for females) by the nurse, and (d) acute medical or surgical conditions or hospitalization within the 3 months (e.g., angina, stroke, major surgery, major depression or serious psychiatric conditions). If a potential participant contacted the Principal Investigator directly, both phases of the screening occurred over the telephone in one session.
Procedures
During the first session, which occurred after the nurses worked three consecutive day shifts, informed consent was obtained and the participants completed the sociodemographic and medical history questionnaires along with seven PROMIS measures. Next, participants were given a sleep diary and explained how to complete it. The second session, in which the nurses completed the same PROMIS measures and returned the sleep diary, occurred approximately 2 weeks later after working three consecutive night shifts. Participants were compensated US$20 after the first session and US$30 after the second session.
Instruments and Measures
Sociodemographic information was collected including age, sex, race, marital status, education, and income. Medical history was collected and included information regarding diagnosed conditions, smoking status/history, and alcohol use (i. e., frequency of drinking, number of drinks consumed when drinking, and frequency when more than six drinks on one occasion were consumed). A list of the current prescriptions and over-the-counter medications was requested to check for medications that affected sleep. During the second session, participants were asked if there had been any changes to the previous provided list of medications.
Seven Patient-Reported Outcomes Measurement Information System (PROMIS) measures were used. The PROMIS measures were developed by the National Institutes of Health to establish precise and efficient measures of patient-reported symptoms, functioning, and health-related quality of life (Cella et al., 2010; DeWalt, Rothrock, Yount, Stone, & PROMIS Cooperative Group, 2007; Hays, Liu, Spritzer, & Cella, 2007; Reeve et al., 2007). For each measure, a higher score represented more of the concept being measured (e.g., a higher sleep-related impairment score represented greater sleep-related impairment) over the past 7 days (Cella, Gershon, Lai, & Choi, 2007). Raw PROMIS measures scores are summed and converted to T-scores, which are standardized scores in which a T-score of 50 is the mean for the general adult population (Cella et al., 2007). Copies of the PROMIS measures and details on their scoring can be found elsewhere (HealthMeasures, 2018).
The PROMIS Global Health Short Form is a 10-item instrument and was used to calculate Global Physical and Global Mental Health (Hays, Bjorner, Revicki, Spritzer, & Cella, 2009). Six questions assessed health with responses ranging from 1 (poor) to 5 (excellent). One question assessed ability to complete everyday activities with responses ranging from 1 (not at all) to 5 (completely). One question assessed the frequency of being bothered by emotional problems with responses ranging from 1 (always) to 5 (never), one assessed fatigue with responses ranging from 1 (very severe) to 5 (none), and pain was assessed by participants rating their pain on a scale of 0 (no pain) to 10 (worst pain imaginable). The Global Physical scale was found to have an internal consistency reliability coefficient of 0.81 while the Global Mental Health scale has a reliability coefficient of 0.86 (Hays et al., 2009).
The PROMIS Sleep Disturbance Short Form 8b includes eight questions. One question assessed overall sleep quality with responses ranging from 1 (very good) to 5 (very poor), while seven questions assessed self-reported perceptions of sleep quality, sleep depth, and satisfaction with sleep with responses ranging from 1 (not at all) to 5 (very much) (Buysse et al., 2010). These items were used to evaluate difficulties getting to sleep and staying asleep, refreshment upon waking, and worry over falling sleep.
The PROMIS Sleep-Related Impairment Short Form 8a includes eight questions and assessed self-reported perceptions of alertness, sleepiness, and tiredness during usual waking hours, and the perceived functional impairments during wakefulness associated with sleep problems or impaired alertness with responses ranging from 1 (not at all) to 5 (very much) (Buysse et al., 2010).
The PROMIS Fatigue Short Form 8a includes eight questions. Six questions assessed fatigue, ability to start things, degree to which fatigue bothered the individual, and degree to which fatigue interfered with physical functioning with responses ranging from 1 (not at all) to 5 (very much). Two questions assessed the frequency in which the individual had to push to get things done and had trouble finishing things due to fatigue with responses ranging from never (1) to always (5) (Cella et al., 2010; DeWalt, Rothrock, Yount, Stone, & PROMIS Cooperative Group, 2007; Reeve et al., 2007).
The PROMIS Emotional Distress Anger Short Form 5a includes five questions and assessed self-reported angry mood and efforts to control anger with responses ranging from never (1) to always (5) (Pilkonis et al., 2011).
The PROMIS Satisfaction with Social Roles and Activities Short Form 8a includes eight questions and assessed satisfaction with performing one’s usual social roles and activities with responses ranging from not at all (1) to very much (5) (Cella et al., 2010; DeWalt et al., 2007; Reeve et al., 2007). The instrument was found to have an internal consistency of > .95 (Cella et al., 2010).
The PROMIS Applied Cognition-Abilities Short Form 8a includes eight questions that assessed self-reported perceptions of memory, ability to focus, and overall thinking with responses ranging from not at all (1) to very much (5) (Cella et al., 2010; Reeve et al., 2007; Saffer, Lanting, Koehle, Klonsky, & Iverson, 2015). The instrument has an internal consistency reliability of > .95 (Saffer et al., 2015).
Self-reported sleep was collected using the Core Consensus Sleep Diary that was developed based on an assessment of 16 different sleep diaries. These diaries were evaluated by an expert panel and nine items representing the most critical parameters were retained. The items comprise (a) the time of getting into bed, (b) the time at which the individual attempted to fall asleep, (c) sleep onset latency, (d) number of awakenings, (e) duration of awakenings, (f) time of final awakening, (g) final rise time, (h) perceived sleep quality rated via Likert-type scale of 1 (very poor) to 5 (very good), and (i) an additional space for open-ended comments from the respondent (Carney et al., 2012).
Analysis
SPSS version 24.0 (IBM; Armonk, NY) was used to analyze the data. Descriptive statistics were used to summarize study variables. Values for the continuous variables are presented as means with standard deviations (SD) and categorical variables are summarized by frequencies and percentages. PROMIS measures t scores were use in the analyses. Pearson’s correlations were used to examine the post-day shift and post-night shift associations between the various PROMIS measures. Paired t tests were conducted to examine the within-subject differences in post-day shift and post-night shift PROMIS measures and the differences in sleep characteristics before day shifts, before night shifts, and before days off. Statistical significance was set at p < .05. Effects sizes were examined using standardized within-subject mean differences (dwithin).
Results
In total, 30 ICU nurses met the phase one eligibility requirements. Two of the nurses could not be contacted to complete the second phase of the screening. In addition, two nurses regularly used medications to help them sleep failing to meet the phase two exclusion criteria. Two nurses screened eligible for the study, but were “no shows” for the first session and could not be contacted to reschedule. Twenty four nurses were eligible and were consented for the study, one participant was lost to follow-up, resulting in 23 study participants that completed the study.
The participants were primarily female (n = 21, 91.3%) with a mean age of 27.0 ± 4.5 years, ranging from 22.0 to 38.0 years (Table 1), Nine were married or living with a partner/significant other (39.1%); only one participant had children. All participants had health insurance. Overall, the participants were healthy with few significant medical conditions: seven reported emotional/psychiatric problems (i.e., depression, anxiety; 30.4%) that were well controlled with therapy or medication; four reported having asthma (17.4%); one participant had diabetes (4.3%); and one reported excessive daytime sleepiness at baseline (4.3%). Two participants were current smokers.
Baseline Characteristics ICU Nurses (N = 23).
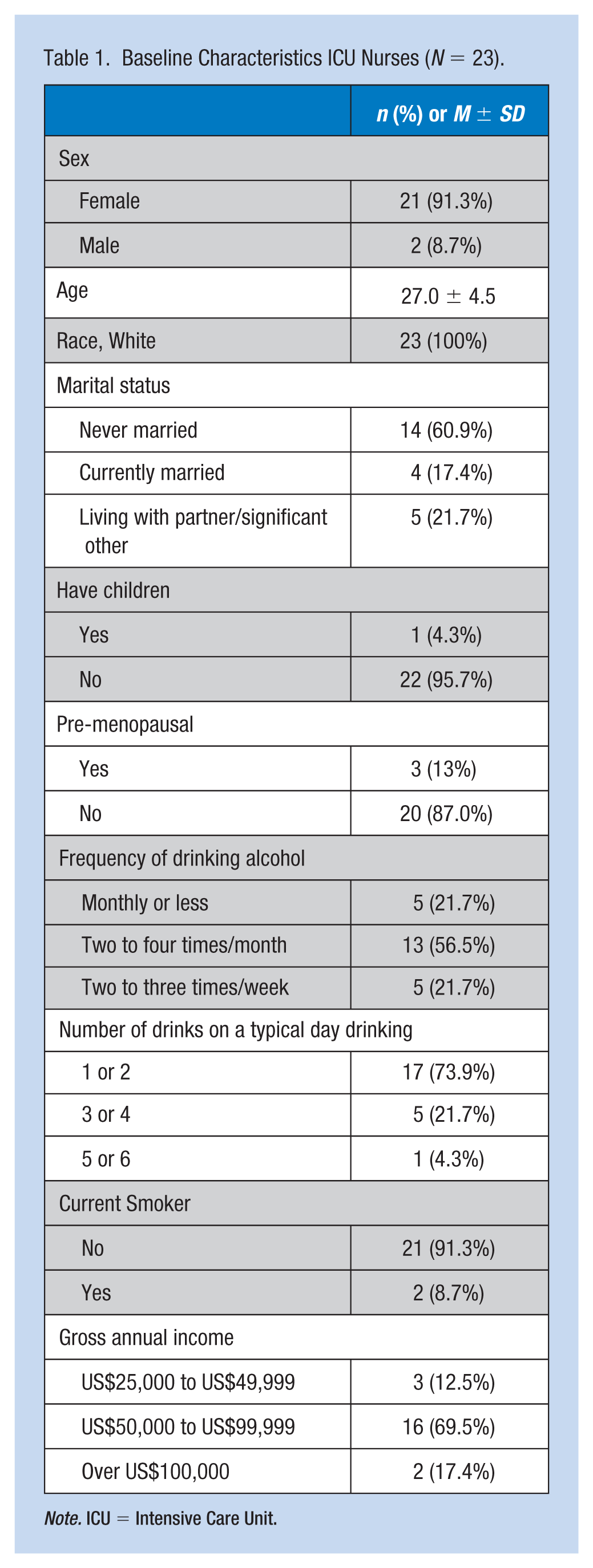
Note. ICU = Intensive Care Unit.
Correlations Between PROMIS Measures Scores
Post-Day Shift and Post-Night Shift Correlations
During both the post-day shift and post-night shift assessments, higher global physical health scores were correlated with higher global mental health scores and lower global mental health scores were correlated with higher emotional distress and lower satisfaction with social roles scores (Tables 2 and 3). In addition, higher sleep disturbance scores were correlated with higher sleep-related impairment, while greater sleep-related impairment scores were correlated with greater fatigue and greater emotional distress scores. Finally, higher fatigue scores were correlated with a higher emotional distress, lower satisfaction with social roles, and lower memory and concentration scores.
Correlations Among PROMIS Scores Collected Post-Day Shift Among ICU Nurses (N = 23).
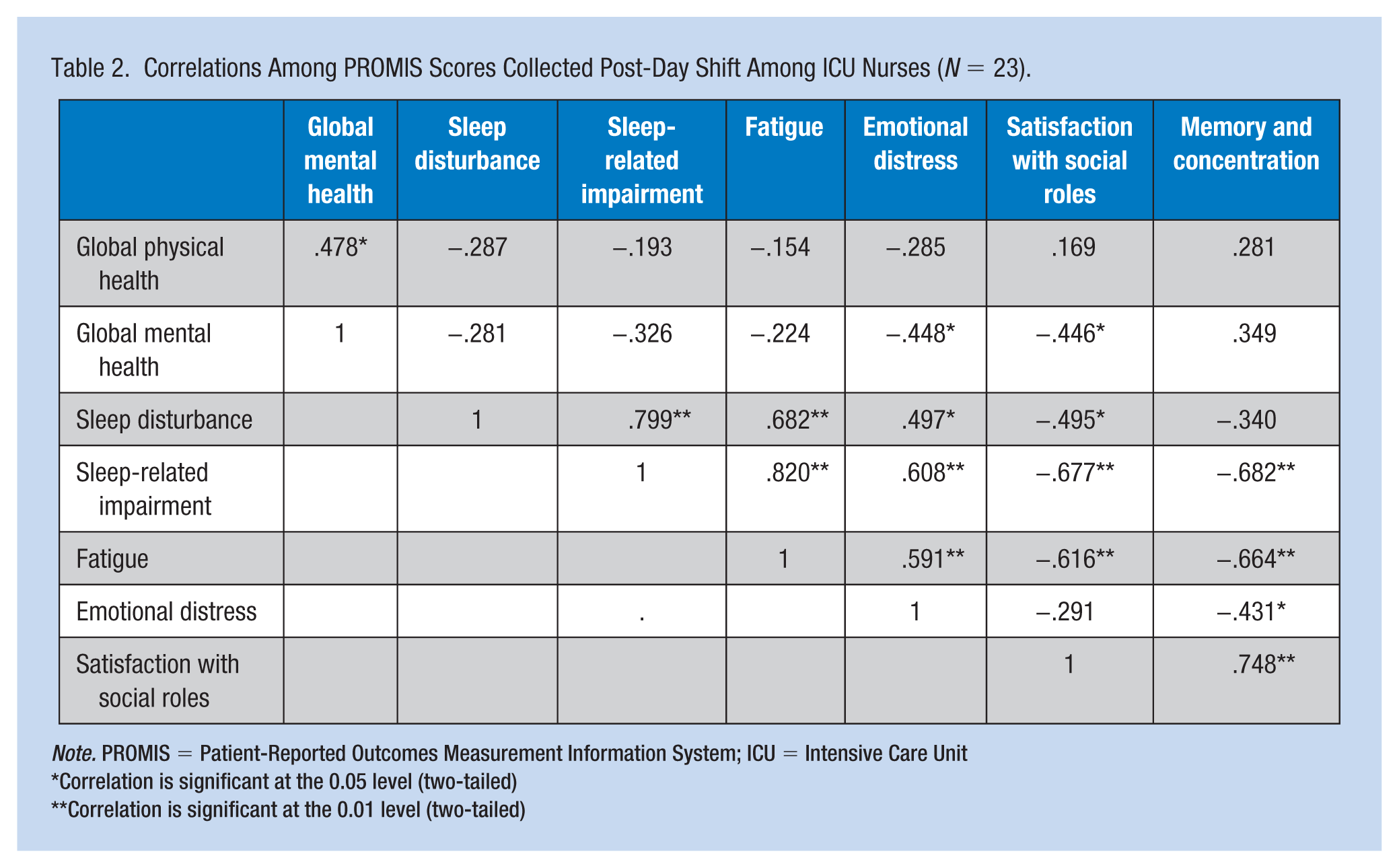
Note. PROMIS = Patient-Reported Outcomes Measurement Information System; ICU = Intensive Care Unit
Correlation is significant at the 0.05 level (two-tailed)
Correlation is significant at the 0.01 level (two-tailed)
Correlations Among PROMIS Scores Collected Post-Night Shift Among ICU Nurses (N = 23).
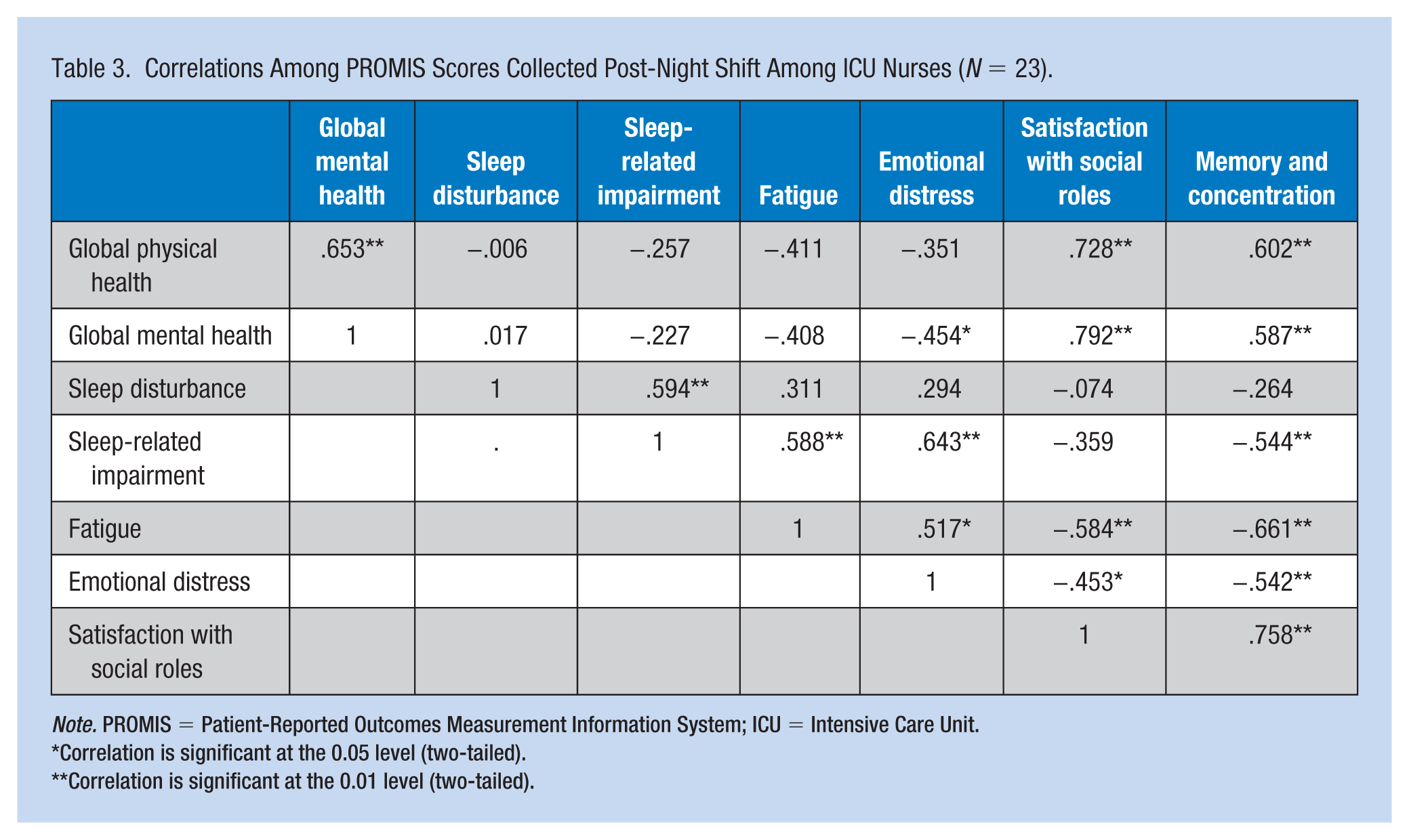
Note. PROMIS = Patient-Reported Outcomes Measurement Information System; ICU = Intensive Care Unit.
Correlation is significant at the 0.05 level (two-tailed).
Correlation is significant at the 0.01 level (two-tailed).
Post-day shift only correlations
During the post-day shift assessment only, higher sleep disturbance scores were correlated with higher fatigue (r = .682, p < .01), higher emotional distress (r = .497, p < .05), and lower satisfaction with social roles (r = −.446, p < .05) scores (Table 2). Also, greater sleep-related impairment scores were correlated with lower satisfaction with social roles scores (r = −.677, p < .01)
Post-night shift only correlation
During the post-night shift assessment only, higher global physical health scores were correlated with higher satisfaction with social roles (r = .728, p < .01) and higher memory and concentration (r = .602, p < .01) scores (Table 3). In addition, higher mental health scores were correlated with higher satisfaction with social roles (r = .587, p < .01) and higher emotional distress scores were correlated with lower satisfaction with social roles scores (r = -.453, p < .05).
Comparisons of PROMIS Measures Between Post-Day Shift and Post-Night Shift
Compared to the post-day shift assessment, all PROMIS measures were worse during the post-night shift assessment with medium to large effect sizes with the exception of sleep disturbance (Table 4). The most significant differences were worse fatigue (54.9 ± 4.6 vs. 49.3 ± 6.0; p < .001, dwithin = −0.90), greater sleep-related impairment (54.0 ± 6.1 vs. 47.7 ± 5.2; p = .001, dwithin = −0.78), lower satisfaction with social roles (48.7 ± 5.9 vs. 51.9 ± 7.3; p =.002, dwithin = 0.72), and lower global physical health (51.7 ± 5.1 vs. 54.7 ± 5.1; p = .009, dwithin = 0.60) after night shifts compared to after day shifts.
Difference in PROMIS t Scores From Post-Day Shift to Post-Night Shift (N = 23).
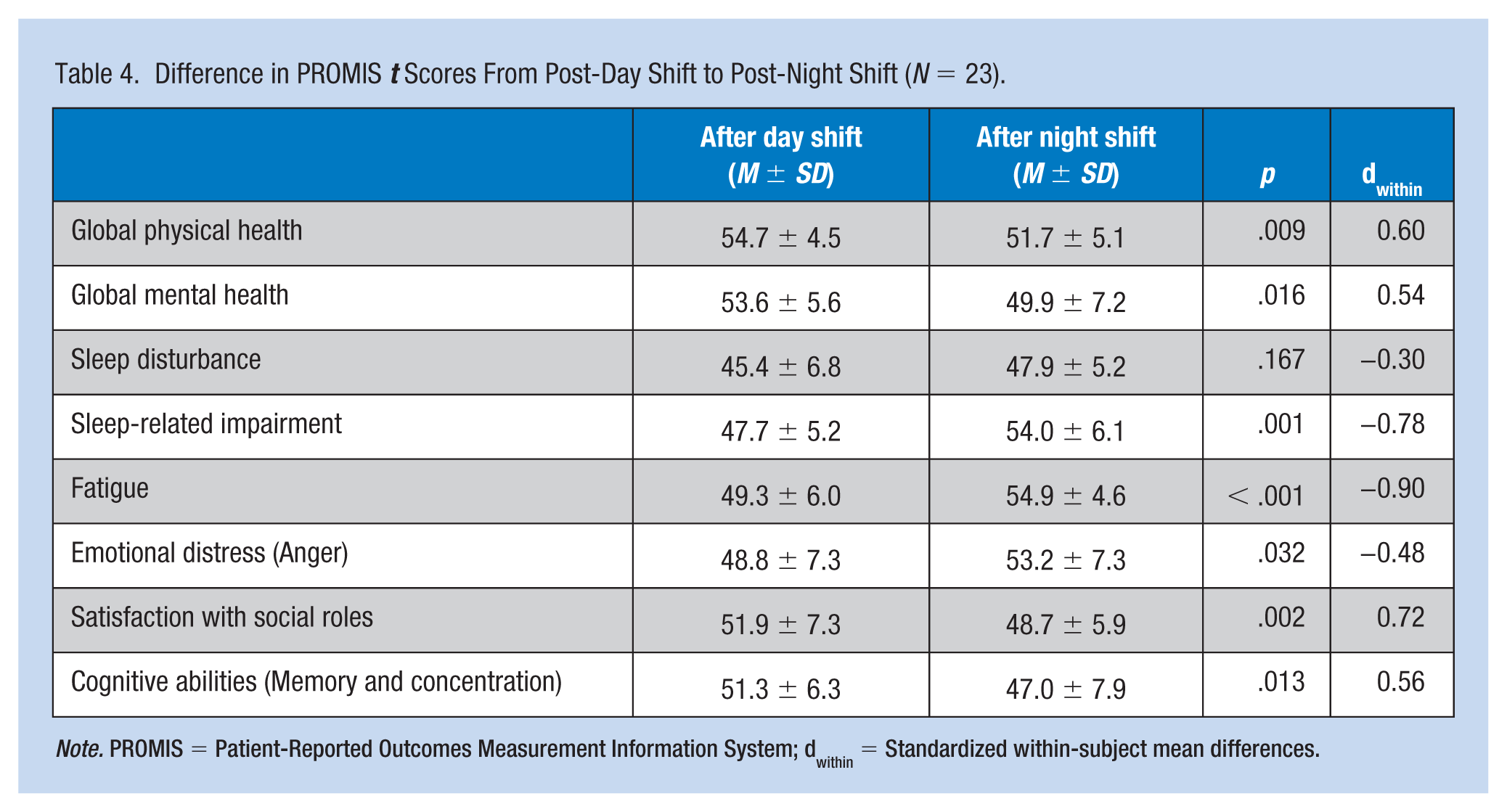
Note. PROMIS = Patient-Reported Outcomes Measurement Information System; dwithin = Standardized within-subject mean differences.
Differences in Self-Report Sleep
Due to their schedules, only seven nurses had complete sleep diaries that included sleep before multiple day shifts, multiple night shifts, and multiple days offs. Based on their sleep diaries, no statistically significant differences in total sleep time (TST) between shifts was seen (p = .636, dwithin = 0.19). Wake after sleep onset, which is a measure of sleep fragmentation, was greater in the sleep before night shifts compared to the sleep before day shifts (p = .015, dwithin = 1.3). In addition, the quality of sleep was lower before night shifts compared to before day shifts (p = .111, dwithin = .7).
When comparing sleep duration before day shifts to sleep duration before days off, total sleep time was 125 min shorter before day shifts (p = .001, dwithin = 2.1). Furthermore, when comparing sleep duration before night shifts to sleep duration before days off, total sleep time was 140 min shorter before night shifts (p = .002, dwithin = 1.9). When comparing sleep quality before night shifts to sleep quality before days off, sleep quality was 0.9 points lower before night shifts (p = .012, dwithin = 1.4). The 0.9 points represents a difference in sleep quality of fair before night shifts to good before days off.
Discussion
In this study of ICU nurses engaged in shift work, sleep-related impairment was strongly correlated with fatigue, emotional distress (anger), and worse cognitive abilities (memory and concentration). These correlations were found both after working day shifts and night shifts. Furthermore, all the PROMIS measures examined in this study were worse after working night shifts compared to after working day shifts. Although the data were limited to the sleep patterns of seven nurses, their sleep quality and sleep fragmentation were negatively affected by working night shift.
The findings from this study are consistent with other studies. For example, Wilson and colleagues (2017) compared the sleep (measured with wrist Actigraphy), sleepiness (measured using the Karolinska Sleepiness Scale), and reaction time (measured using the Psychomotor Vigilance Test) of 11 day-shift nurses to 11 night-shift nurses. Overall, there were no differences in total sleep time. For the night-shift nurses, reaction time degraded with time on duty while it remained relatively stable for day-shift nurses. Similar results were observed for sleepiness. Correspondingly, a cross-sectional study by Park, Lee, and Park (2018), found that shiftwork, greater sleep disturbances, and lower subjective sleep quality were statistically significant predictors for lower nurse productivity.
This study found that working night shifts, compared with working day shifts was associated with decreased physical and mental health and less satisfaction with social roles. As previously mentioned, shift work is associated with an increased risk for numerous health conditions. Specifically among ICU nurses, Jensen, Larsen, and Thomsen (2018) found that night shift was associated with mood swings and physical symptoms such as headaches and nausea. Furthermore, in a recent cross-sectional study of nurses by Zhang, Duffy, de Castillero, and Wang (2018) sleep difficulties, specifically sleep onset latency > 30 min and the use of sleep promoting substances were associated with increased risk for work-related musculoskeletal disorders after adjusted for covariates. From the same study, the research team found an association between work–family conflict and more depressive symptoms and that sleep disturbances partially mediated the association (ZhangY, Duffy, & de Castillero, 2017). Similarly, Bazazan, Dianat, Mombeini, Aynehchi, and Asghari Jafarabadi (2018) reported that among nurses, a lower quality of life was associated with mental health problems and that fatigue partial mediated the relationship.
Other studies have reported that shift work among nurses is associated with decreased sleep quality consistent with the finding from this study. For example, Gold et al. (1992) found that individuals that rotated shifts were three times more likely to report poor sleep compared to individuals working fixed-day or fixed-evening shifts. In addition, McDowall, Murphy, and Anderson (2017) reported that working shifts was associated with poor sleep quality after adjusting for age, gender, and years of nursing experience.
The American Academy of Nursing recently released a position statement aimed at reducing the fatigue associated with sleep deficiency and work hours in nurses (Caruso et al., 2017). In their position statement, they urge (a) nurses and employers to educate themselves about the risks associated with shift work (b) employers to incorporate evidence-based practices and promote a workplace culture that encourages sleep health, and (c) experts to develop additional education courses that relay evidence-based practices and interventions that maximize sleep health (Caruso et al., 2017). While these steps are essential, further research is needed to develop interventions that utilize wearable technology to guide sleep habits and promote healthy lifestyle choices.
Limitations of the study include the use of self-reported measures, its small sample size, especially regarding the sleep data before day shifts, night shifts, and days off, and its homogeneous sample. Given that the study was limited to ICU nurses from one hospital and that the sample was white and mostly females without children, the results should be interpreted cautiously. Nonetheless, the study findings are consistent with the literature. A major strength of the study is its use of within-subject, repeated measures. Most of the research on shift work, sleep, and health rely on cross-sectional, between-subject designs.
Conclusion
The results of this study, that rotating shifts negatively affects health and wellness of nurses, are consistent with findings from previous studies. This study demonstrates how sleep-related impairment, which was greater when working night shifts, is highly correlated with greater fatigue, greater emotional distress (anger), and worse cognitive abilities (memory and concentration). Given that shift work is a necessary aspect of acute care, nurses, nurse managers, and employers must emphasize practices and policies that promote healthy sleep behaviors. Researchers should embrace new technologies, such as wearable sleep and fitness trackers, and develop interventions to guide healthy sleep behaviors.
Implications for Occupational Health Nursing Practice
Growing evidence supports the negative effects of working nights and rotating shifts (shift work) on sleep, overall health, memory and concentration, and emotional and mental health. Nurses and nurse managers/administrators play equal roles in promoting sleep health. Nurses must prioritize sleep over other competing demands to ensure adequate sleep duration. But this is only possible when nurse managers and administrators follow evidence-based practices regarding scheduling and work hours that promote an environment that encourages sleep health. Occupational health nurses should educate both nurses and administrators about the risks associated with shift work and actively advocate for policies that maximize rest periods, support appropriate work hours, and ensure adequate scheduling practices.
Applying Research to Practice
This research supports the negative effects of working nights and rotating shifts the on sleep, mental and physical health, and memory and concentration of nurses. While shift work is a necessary aspect of acute care, nurses, nurse managers, and occupational health nurses must work together to create an environment that supports healthy sleep behaviors. Nurses must take personal responsibility to ensure adequate sleep duration while managers must follow evidence-based scheduling practices. Occupational health nurses should educate both nurses and managers on the risks of poor sleep and advocate for practices and policies that encourages healthy sleep.
Footnotes
Acknowledgements
The authors would like to thank the nurses who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the University of Pittsburgh School of Nursing’s Research Seed Money. ERC was supported by NIH K24-NR016685.
Author Biographies
Christopher C. Imes, PhD, RN is an assistant professor in the Acute and Tertiary Care Department at the University of Pittsburgh School of Nursing.
Eileen R. Chasens, PhD, RN, FAAN is a professor in the Health and Community Systems Department at the University of Pittsburgh School of Nursing.