
Abstract
Nursing knowledge surrounding anesthesia providers’ maintaining or obtaining employment after treatment of substance use disorder (SUD) is notably absent in the literature. An alternative method, dimensional analysis, allows for exploration of this concept from many perspectives, with social context as the basis from which to determine what barriers exist and how to prevail over them. Anesthesia practice is a socially constructed profession. The concept, barriers to reentry into nurse anesthesia practice, was explored and defined for purposes of identifying their impact on the recovering certified registered nurse anesthetist (CRNA). Defining the barriers places the CRNA one step closer to successful reentry into anesthesia practice.
Introduction
Reentry into nurse anesthesia practice following substance use disorder (SUD) treatment is challenging for the affected nurse anesthetist, their peers, and employers. Substance use disorder or SUD is a disease in which an individual misuses medications such as psychotropic substances resulting in the disruption of a person’s health and judgment (Crowley & Morgan, 2014; Higgins Roche, 2007). According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), “the essential feature of a substance use disorder is a cluster of cognitive, behavioral, and physiological symptoms indicating that the individual continues using the substance despite significant substance-related problems” (Substance Use Disorders, para. 1). The DSM-5 (American Psychiatric Association, 2013) further describes the diagnosis of SUD as a consistent pattern of behavior involving the use of a substance, with severity ranging from mild to severe. Drug misuse and diversion of substances relate to the misappropriation of medications such as narcotics, benzodiazepines, and the agent propofol, used in the course of anesthesia practice. Diversion of medication involves stealing drugs intended for patient care needs and using them for personal use or other illegal use (Crowley & Morgan, 2014).
Being an anesthesia provider places a person at risk for developing SUD, in part, to the ready accessibility of substances in the workplace. Similar to other chronic conditions such as hypertension and diabetes, SUD can be treated and managed successfully, resulting in the provider reentering the workforce (Bettinardi-Angres & Garcia, 2015; Wright, McGuinness, Schumacher, Zwerling, & Moneyham, 2014). Whether the provider self-reported misuse or diversion of substances of abuse to the state board of nursing (SBON), or the provider was discovered diverting substances of abuse, there are many obstacles for the nurse anesthetist attempting reentry as peers have difficulty accepting the affected nurse anesthetist back into practice because trust has been breached. Employers must balance retaining talented providers while simultaneously protecting their patients. However, SUD, like other chronic diseases, has an identifiable spectrum and if certain conditions are met, the disease may be managed successfully (Bryson & Levine, 2008; Wilson & Compton, 2009).
Background
According to the Substance and Mental Health Services Administration (SAMHSA) in 2014, 27.0 million people aged 12 or older used an illicit drug, which corresponds to about 1 in 10 Americans (SAMHSA, 2017). Data on prevalence of substance use and abuse among health care professionals, particularly nurse anesthetists, is not as easily obtained, as noted by McDonough in 1990 and then by Wright and colleagues 22 years later (Wright et al., 2012). Estimations of SUD among nurse anesthetists are derived primarily from survey questionnaires and treatment center data (Bennett & O’Donovan, 2001; Higgins Roche, 2007). Bell, McDonough, Ellison, and Fitzhugh (1999) surveyed nurse anesthetists and found that 9.8% of respondents reported diversion of substances for personal use. This correlates to approximately 10% (or 5,000 as of 2014) of nurse anesthetists in the United States with some form of SUD (Valdes, 2014).
In anesthesia practice, SUD is one of the leading occupational hazards (Bajwa & Kaur, 2012; Collins, McAllister, Jensen, & Gooden, 2005). Ease of access to medications and genetic susceptibility place those at risk for developing the disease in the position to begin a devastating spiral of diversion and use, advancing to abuse and dependence. If left untreated, similar to other undiagnosed chronic diseases, death can occur, which in anesthesia providers may be the first sign of the disease (Valdes, 2014; Wright et al., 2012). Though the signs of SUD rarely go undetected, accidental or intentional overdose may be the first recognized occurrence of the disease (Higgins Roche, 2007).
With advances in SUD resources including treatment, support, and after-care, SUD need not be career ending in nurse anesthesia (Higgins Roche, 2007; Kunyk, 2015). Prior study findings indicate a gap in nursing knowledge surrounding anesthesia providers’ maintaining or obtaining employment after treatment of SUD (Hamza & Monroe, 2011; Wright et al., 2014). Ideal goals for the addicted certified registered nurse anesthetist (CRNA) should be to receive proper treatment for SUD and, if deemed fit to return to work, to reenter the workforce successfully with after-care and support systems in place. However, there are both real and perceived barriers that impede the process of returning to work successfully (Matthias-Anderson & Yurkovich, 2016). The focus of this concept analysis included the diversion and misuse of anesthetic agents (narcotics, benzodiazepines, propofol and inhalational gases) in the course of anesthesia practice. Through the process of an in-depth literature review, we sought to clarify the concept barriers to reentry into anesthesia practice after SUD treatment.
Literature Search
The literature search is outlined in Figure 1. Multiple databases were used to search the literature including PubMed, Cumulative Index to Nursing and Allied Health (CINAHL), Scopus, Google Scholar, Embase, Cochrane Library, BioMed Central, Dissertations and Theses, Grey Literature Report, and PsycINFO. An initial search in PubMed using the terms “substance use disorder” AND “anesthesia” was used to increase the yield of relevant literature. Adjusting the search terms to “substance-related disorder” AND “addiction” AND “anesthesiologist” AND “nurse anesthetist” OR “anesthesia provider,” the search resulted in 210 results in PubMed and 117 results in CINAHL. The search terms “barriers to reentry” AND “anesthesia” yielded zero results in PubMed and in CINAHL.
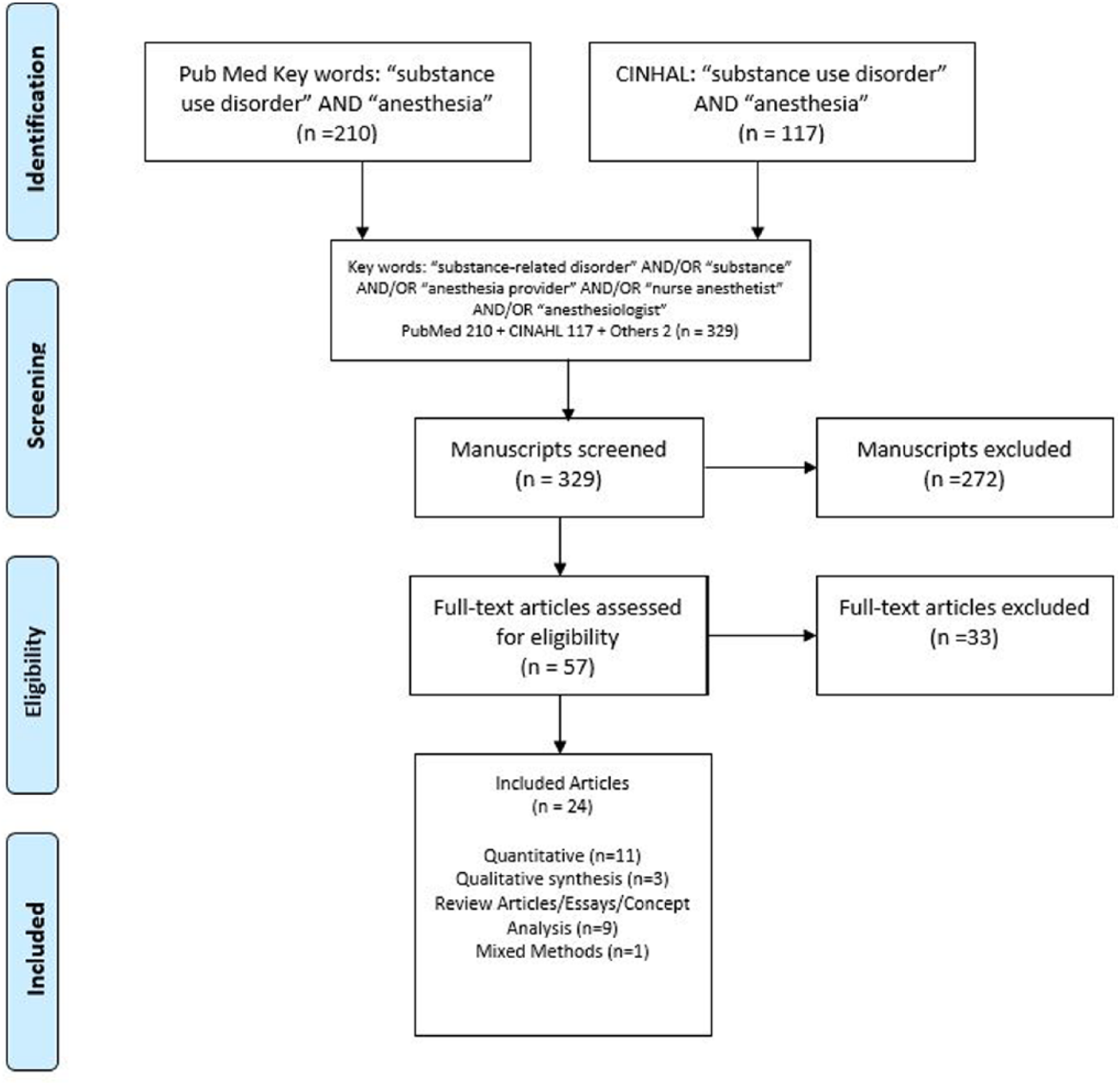
Literature search strategy to identify articles that contributed to the concept analysis of barriers of reentry into nurse anesthesia practice following substance use disorder.
In addition to the searches in PubMed and CINAHL, the same search term combinations were used in the remaining databases contributing two additional articles. The combined results of PubMed, CINHAL, and the other database searches yielded 327 total articles. In addition, two book sources, Crowley and Morgan (2014) and Higgins Roche (2007), were identified in the search.
A review of article titles and abstracts was conducted based on our inclusion criteria: the article had to pertain to anesthesia practitioners (nurse anesthetists and anesthesiologists), all date ranges, full text available, and written in English. This initial title and abstract review excluded 272 articles, resulting in 57 articles that were eligible for full-text review. Utilizing the inclusion criteria in the full-text review, 33 articles were excluded, leaving 24 articles for this literature review.
In summary, 24 peer-reviewed journal articles and 2 books contributed to this review of literature. The quantitative studies consisted of 11 studies, of which six studies were from nursing and five were from medicine. There were three qualitative studies of which two were conducted by the nurse anesthesia discipline. There was one study that was a mixed methods of both quantitative and qualitative. The remaining 13 articles were literature reviews in which four were from nursing, two from psychiatry, two from anesthesiology, two from other physician specialties, and three from nurse anesthesia.
Approach
Twenty-four articles discussed aspects of barriers to reentry, yet none of them clearly defined the concept, as described in Table 1. A concept analysis was performed to provide a clearer understanding of the concept of interest, with the overall intent of contributing to nursing knowledge (Foley & Davis, 2017). There are several ways a concept analysis can be conducted, including methods pioneered by Wilson, Rodgers, and Walker and Avant (Caron & Bowers, 2000). Dimensional analysis is an alternative method of a concept analysis in that it utilizes social construction to understand concepts essential to developing nursing knowledge (Caron & Bowers, 2000). Simply stated, it is a way to examine a concept central to nursing through a social platform; specifically, gathering information on how people think and feel about a socially constructed subject. Developed by Schatzman (1991), dimensional analysis is grounded in the philosophical paradigm of pragmatism and symbolic interactionism. Organizing the available literature into common themes is a pragmatic way to explore the concept of barriers to reentry. According to Blumer (1969), symbolic interactionism includes three assumptions: people react to things in their lives according to their recognized meanings; meanings originate from interactions with others; and people alter meanings through various processes to have a clearer understanding of their social environment. The practice of anesthesia is a socially constructed profession due to the frequent interactions with patients and their families, surgeons, colleagues, and perioperative staff, each will have different perspectives about barriers to reentry into anesthesia practice. Through the review of literature, themes manifested that were identified as separate characteristics yet were interrelated to the overall subject matter.
Summary of the Literature Highlighted in the Concept Analysis
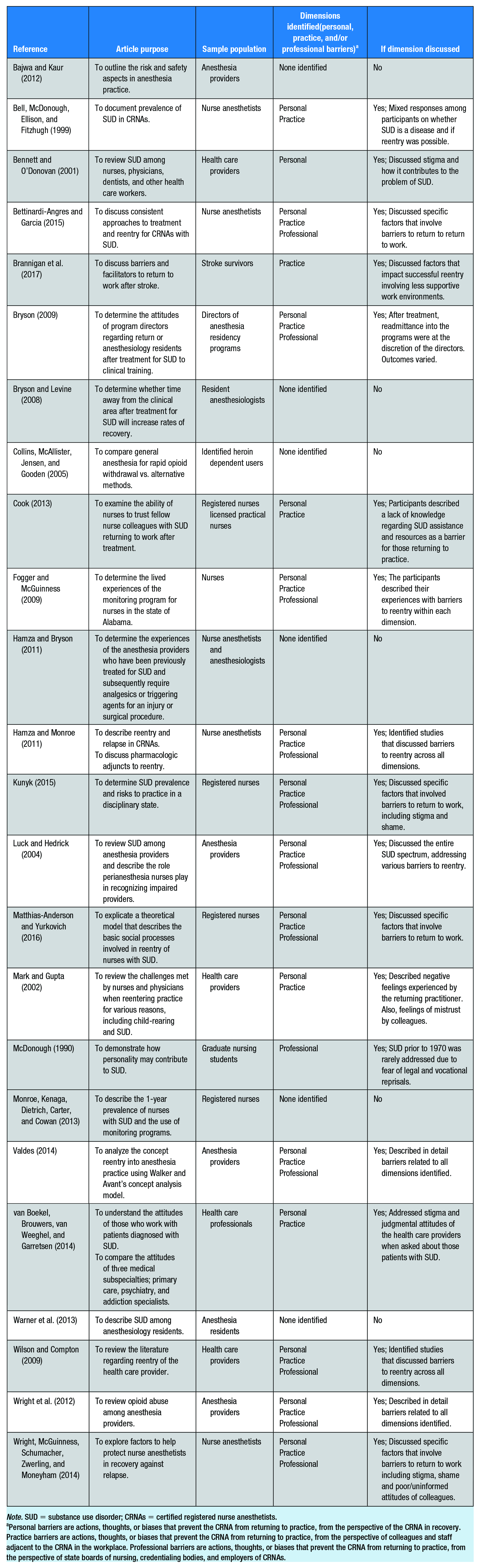
Note. SUD = substance use disorder; CRNAs = certified registered nurse anesthetists.
Personal barriers are actions, thoughts, or biases that prevent the CRNA from returning to practice, from the perspective of the CRNA in recovery. Practice barriers are actions, thoughts, or biases that prevent the CRNA from returning to practice, from the perspective of colleagues and staff adjacent to the CRNA in the workplace. Professional barriers are actions, thoughts, or biases that prevent the CRNA from returning to practice, from the perspective of state boards of nursing, credentialing bodies, and employers of CRNAs.
Findings
Dimensions of Work Reentry
It was revealed from the literature that barriers to reentry is a multifaceted phenomenon. The views on what barriers may or may not exist varied between those most closely involved in the workplace. Based on the review of literature, themes from the literature were operationalized into three different, yet interconnected domains including: (a) personal barriers, (b) practice barriers, and (c) professional barriers, as illustrated in Figure 2. Personal barriers are actions, thoughts, or biases that prevent the CRNA from returning to practice, from the perspective of the CRNA in recovery; practice barriers are actions, thoughts, or biases that prevent the CRNA from returning to practice, from the perspective of colleagues and staff adjacent to the CRNA in the workplace; and professional barriers are actions, thoughts, or biases that prevent the CRNA from returning to practice, from the perspective of state boards of nursing, credentialing bodies, and employers of CRNAs.
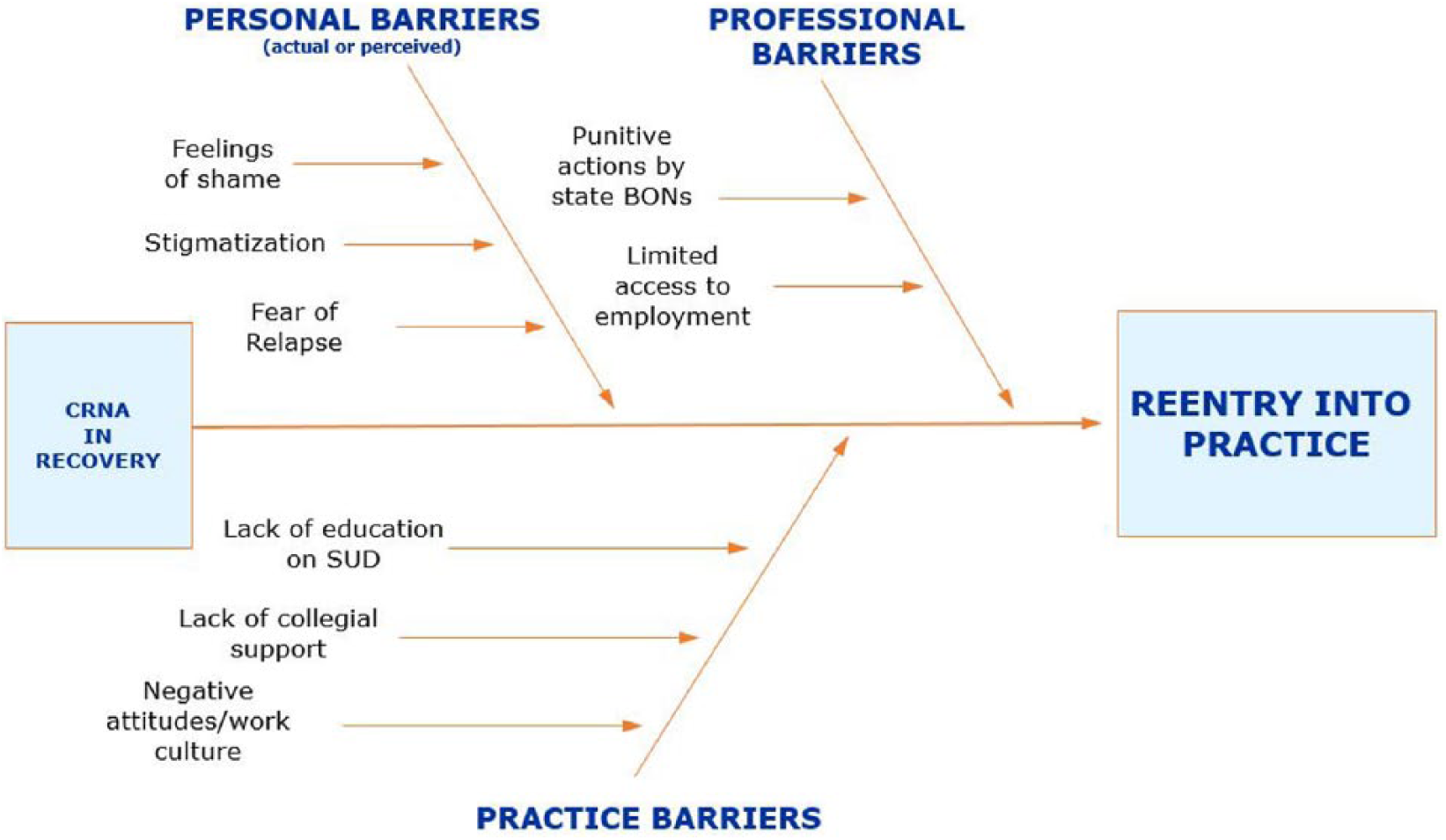
Dimensions and perspectives identified from the concept analysis of barriers to reentry into nurse anesthesia practice following treatment for substance use disorder.
Personal Barriers to Work Reentry
The personal dimension was an important factor to consider as the CRNA in recovery learned to live with SUD as a treatable and manageable disease. One barrier often mentioned by CRNAs in recovery was the potential for relapse due to the accessibility of the substance of abuse (Hamza & Bryson, 2011; Hamza & Monroe, 2011; Higgins Roche, 2007). The availability and access of controlled substances could lead to misuse, potentially triggering a relapse (Bell et al., 1999; Hamza & Bryson, 2011; Wright et al., 2012). Valdes (2014) reported relapse rates ranging from 25% to 56%. A noted gap was that neither the timing from reentry to relapse nor the contributing factors of the relapse were available in the literature (Hamza & Bryson, 2011).
We found that there are no set guidelines which specifically address when a provider should reenter the workforce. There were also no uniform standards established regarding return to work after treatment for SUD. According to the National Council of State Boards of Nursing (NCSBN), each state is governed by individual employers, its respective Nurse Practice Act, and its presence or absence of an alternative to discipline (ATD) program (2017b). Alternative to discipline programs focus on rehabilitative efforts of returning the provider to an optimal state of health and reentry into the workforce as opposed to disciplinary actions punitive treatment alone (Monroe, Vandoren, Smith, Cole, & Kenaga, 2011). However, the most common recommendation was for the addicted provider to remain out of anesthesia for at least 1 year after diagnosis of SUD (Bryson & Levine, 2008; Higgins Roche, 2007). Once a provider returned to the clinical setting, avoidance of substances that led to abuse may not be possible. More than likely, the CRNA would be working with the very drugs they began to divert. Reducing cravings and trigger management are key to successfully managing relapse (Wright et al., 2014).
There was one novel case study in the literature where an anesthesia department worked with recovering medical doctors of anesthesia (MDAs) and placed them in the best position possible to prevent relapse after treatment for SUD. Bryson and Levine (2008) studied five anesthesiology medical residents for 1 year to determine whether time away from the clinical setting would reduce the rate of relapse. Instead of being placed back in the operating room providing anesthesia with patients, the residents were assigned to the anesthesia simulation lab for a period of 12 months. During that time, the emphasis was placed on the importance of early recovery by working in the simulation lab and allowing time off to attend support group meetings. After the completion of the 12 months in the simulation lab, actual operating room clinical time was slowly added into their schedules. For the first 3 months, a reduced schedule consisting of strict work hours (40 hours maximum per week) was enforced. Call shifts were eventually introduced into their schedules over time. Of the five participants, two residents (40%) relapsed after 3 months, during the time additional responsibilities were added to their schedules. The remaining three residents (60%) successfully completed the program and gradually reentered practice after 1 year.
Another barrier identified in the literature was the financial stress that is placed on the CRNA while in recovery. If employers adhered to the recommendation of 1 year away from anesthesia practice, that is a minimum of 1 year of lost income. The loss of health insurance, cost of frequent urine drugs screens at the expense of the CRNA, and fees for legal representation are all related to the barrier of financial stress which can hinder reentry into anesthesia practice (Matthias-Anderson & Yurkovich, 2016; Valdes, 2014).
Other barriers cited in the literature involved fear, stigma, and shame that accompanied SUD (Higgins Roche, 2007; Matthias-Anderson & Yurkovich, 2016). Avoiding the stigma and self-judgment that accompanies SUD can be difficult (Crowley & Morgan, 2014). Characterized as internal barriers to work reentry, those perceptions along with poor self-image acted not only as barriers into reentry into anesthesia practice following SUD treatment, they were also some of the very same characteristics that limited those seeking help initially for SUD (Kunyk, 2015; Mark & Gupta, 2002; Warner et al., 2013).
Practice Barriers to Reentry to Work
The practice dimension was explored from the perspective of colleagues and perioperative staff. The elements of this dimension included potential lack of collegial support, potential lack of education regarding SUD as a disease, and the potential lack of creating a culture of encouragement and acceptance to facilitate a smooth transition of a provider back into the workplace after treatment. Once a provider was identified as impaired, ideally, they were removed from practice, placed in an inpatient treatment facility, and received the help they needed to become healthy enough to return to the workplace (Hamza & Monroe, 2011; Higgins Roche, 2007). Colleagues and staff were often left to deal with feelings of shock, betrayal, and mistrust during the aftermath of the discovery of an impaired provider (Cook, 2013; Crowley & Morgan, 2014). A debriefing, if performed, provided an opportunity to educate the staff on the disease of addiction and facilitated a supportive transition once the provider was deemed eligible to return to practice. The lived experiences of colleagues and staff surrounding a provider who suffered with the disease of SUD in the workplace were not well defined.
Complicating reentry was the lack of education about SUD on the part of colleagues and perioperative staff. Uninformed colleagues, nursing supervisors, department chiefs, and human resources staff were identified as active barriers to reentry into practice (Hamza & Monroe, 2011; Higgins Roche, 2007; Matthias-Anderson & Yurkovich, 2016). Although there was a minimal amount of literature about this dimension and SUD, there were studies that examined return to work following other chronic disease states. Brannigan et al. (2017) performed a meta-synthesis on the barriers and facilitators when returning to work after stroke and found an association among return to work, supportive work colleagues, and supportive work environments.
Collegial attitudes such as denial, blaming, avoidance, shaming, and ignorance vary within each discipline and across disciplines regarding reentry of providers in recovery for SUD (Crowley & Morgan, 2014). Nurses and physicians surveyed revealed those with prior experience with someone with SUD are more likely to be accepting of a recovering provider reentering the workplace (Bryson, 2009; Cook, 2013; van Boekel et al., 2014). A supportive culture in the workplace could have a positive impact on improving attitudes and perceptions regarding those with SUD.
Professional Barriers to Reentry to Work
The professional dimension was explored from the perspective of SBONs regulatory agencies and prospective employers. Two of the most challenging barriers found in the literature surrounding successful reentry into anesthesia practice following treatment for SUD were actual and potential disciplinary actions from the SBON and finding employers willing to monitor someone in recovery (Bettinardi-Angres & Garcia, 2015; Hamza & Monroe, 2011; Wilson & Compton, 2009). The directive of each SBON is to protect the public’s health by ensuring the safe practice of nursing by regulating nursing practice and enforcing the nursing laws of every state (NCSBN, 2017c).
The National Council of State Boards of Nursing (NCSBN, 2017) reported there are 38 states and the District of Columbia with established ATD programs. Alternative to discipline programs emphasize the treatment of SUD as a disease and the promotion of rehabilitation (Crowley & Morgan, 2014; NCSBN, 2017a). Remaining are providers in four states that have vague provider ATD programs subject to individual board approval and eight remaining states without an ATD, leaving them vulnerable to disciplinary actions only, which is rooted in punitive rather than restorative actions (NCSBN, 2017a). Fear of punishment by the SBON, coupled with extended wait times for SBON to complete investigations, are viewed as barriers to reentry into anesthesia practice (Fogger & McGuinness, 2009; Matthias-Anderson & Yurkovich, 2016; Monroe, Kenaga, Dietrich, Carter, & Cowan, 2013).
Another barrier noted was the lack of available monitoring of the recovering CRNA in the workplace. Successful reentry is aided by allowing a colleague to work closely with the recovering provider for a specified amount of time. Finding employers willing to monitor someone in recovery, and working with managers, hospital administrators and credentialing committees who are generally uninformed about SUD are also considered barriers to reentry into anesthesia practice (Bettinardi-Angres & Garcia, 2015; Hamza & Monroe, 2011; Wilson & Compton, 2009). Monitoring the recovering CRNA helps limit employer liability, protect the public, and provide colleagues a way to detect relapse early, as the recovering CRNA is not working alone or unmonitored (Crowley & Morgan, 2014; Higgins Roche, 2007).
The number of CRNAs who reenter anesthesia practice after treatment for SUD is unknown. However, organizational barriers continued to be challenging to those in recovery who were seeking to reenter the workforce. Employers are reluctant to hire providers in recovery due to fear of relapse (Bryson, 2009; Valdes, 2014). However, with advances in treatment modalities and after-care monitoring programs, reentry is less expensive than hiring and training new staff (Higgins Roche, 2007; Kunyk, 2015; Luck & Hedrick, 2004). A CRNA’s ability to practice relies on being actively licensed by the SBON. Without a nursing license, a CRNA cannot practice anesthesia. Inability to practice as a CRNA leads to potential loss in certification, which is another professional barrier to reentry into anesthesia practice.
Discussion
This concept analysis of barriers to reentry into anesthesia practice following SUD treatment is multidimensional. Though concepts such as shame, stigmatization, and fear of relapse have been explored in the literature, enduring gaps in knowledge persist. One notable gap is the time period, or the transition from discovery of drug use and diversion to entering treatment. Some anesthesia departments have guidelines in place that assist the employer and the provider on the steps to treatment and recovery (Crowley & Morgan, 2014; Higgins Roche, 2007). Unfortunately, this is not available nationwide. Once treatment has commenced, the recovering CRNA can find after care support in Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) meetings. Wright and colleagues (2014) examined protective factors against relapse in nurse anesthetists and noted that participants credited 12-step processes such as AA and NA to their continued recovery.
Higgins Roche (2007) reported that from an economic standpoint, reentry is less expensive than hiring and training a replacement. This may be an advantage to both the recovering CRNA and the organization. Furthermore, retaining a provider in recovery with a worksite monitor keeps someone with identified SUD under scrutiny, which enhances patient safety.
There is a dearth of information available in the literature. The experiences of colleagues working with recovering providers is unknown. If a recovering provider does return to work, an additional hurdle is working with colleagues who have varying opinions on SUD and may be misinformed about the topic. This may add additional challenges to reentry for the recovering CRNA. More education is needed on the topic of SUD for practicing CRNAs and for hospital administration at every level.
A culture of rehabilitation and acceptance of SUD as a disease process is desired rather than a culture of punitive actions and shame. Eight SBONs do not have any version of an ATD program. Although protection of the public is the top priority for regulatory agencies, clearly barriers exist within them that prohibit providers from reentering the workplace once deemed fit to return to practice. SBONs need to recognize that addiction is a disease that can be treated and managed successfully. Nursing should be the leaders in showing compassion and aiding fellow nurses toward rehabilitation. The major limitation of this concept analysis is the lack of available literature about barriers to reentry after SUD treatment.
Conclusion
Barriers to reentry into anesthesia practice following SUD treatment is a multidimensional concept that requires further study. SUD is a disease that many people experience in some form either directly or indirectly as a friend, family member, colleague, or supervisor. Despite the prevalence of SUD, it is a topic that very few people want to discuss due to the associated stigma. Nurse researchers have the opportunity lead to research in reentry into practice after treatment for SUD. The increased prevalence of SUD in the United States indicates this issue is not likely to diminish any time soon. Additional research is needed to advance the knowledge of barriers to reentry into anesthesia practice after treatment for SUD and begin to identify facilitators to successful reentry.
Implications for Occupational Health Nurse Practice
Lack of education and misinformation can directly impact someone seeking treatment for SUD or not. The occupational health nurse has the unique ability to impact how providers with SUDs are received in the workplace. By providing as much education to staff as possible, occupational health nurses can increase awareness by making SUD screening a vital part of their initial assessment strategy. The American Association of Nurse Anesthetists (AANA) has compiled evidenced-based policies and procedures that can be adopted as guidelines to assist other health care disciplines in navigating issues regarding SUD. Figure 3 outlines a screening tool that occupational health nurses can utilize to identify someone who potentially is impaired from a SUD in the workplace. Instituting this screening tool as a part of everyday practice, the occupational health nurse may lead to the early detection of an impaired provider. Occupational health nurses play an important role in striking the delicate balance between protecting the public and ensuring competent providers are returned to practice after treatment for SUD.
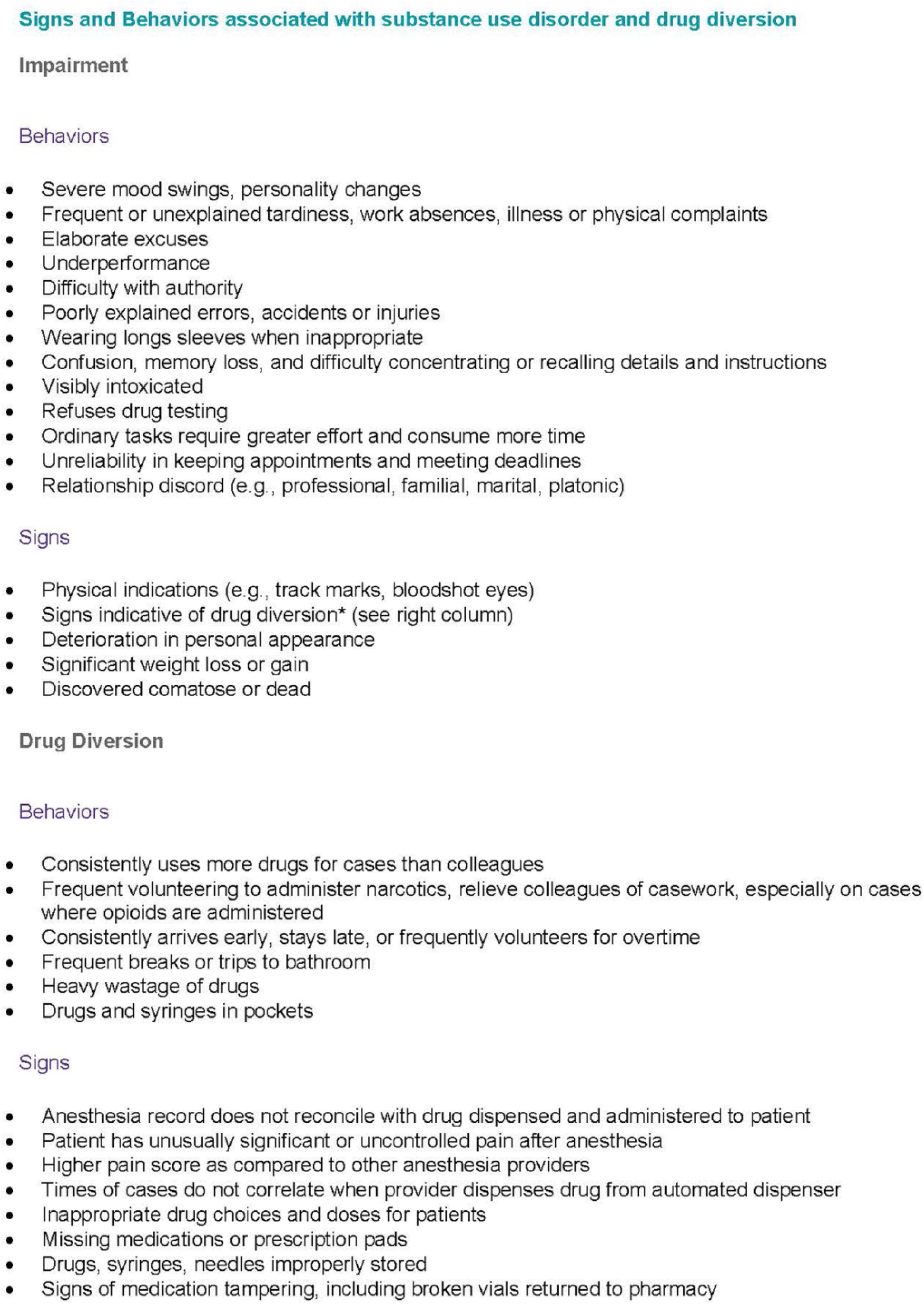
Screening tool for occupational health nurses to identify impairment, adapted from the American Association of Nurse Anesthetists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Deep South Center for Occupational Health and Safety (NIOSH-T42OH008436).
Author Biographies
T’Anya Carter is a NIOSH Fellow and PhD trainee in the University of Alabama at Birmingham’s Nursing Program. Her research interest includes substance use disorder among Certified Registered Nurse Anesthetists (CRNAs).
Susan P. McMullan is an associate professor and the Doctor of Nursing Practice (DNP) Nurse Anesthesia Program Director at the University of Alabama at Birmingham School of Nursing. She has been a CRNA for over 30 years and has provided anesthesia for all patient populations.
Patricia A. Patrician, PhD, RN, FAAN is professor and Rachel Z. Booth Endowed Chair at the University of Alabama at Birmingham (UAB) School of Nursing and Co-Directs the Birmingham, VA Quality Scholars Fellowship Program. Prior to joining UAB in August 2008, she served 26 years in the US Army Nurse Corps, retiring as Colonel. She teaches concept analysis and theory to PhD students and conducts research on nurse staffing, the practice environment, patient safety and quality patient and nurse outcomes.