
Abstract
The purpose of the study was to evaluate the effects of a modified mindfulness-based stress reduction (MBSR) program on the levels of stress, affect, and resilience among nurses in general hospitals in mainland China. In addition, the study attempted to determine the impact of the program on job satisfaction. A total of 110 nurses were randomly assigned to the intervention versus control groups. The intervention group participated in a modified 8-week MBSR program. All participants were evaluated with questionnaires at baseline, immediately after the intervention, and 3 months later. The intervention group showed decreases in stress and negative affect and increases in positive affect and resilience after the intervention. No improvement in job satisfaction was observed, but the trends of the data were in the hypothesized direction that job satisfaction would improve. The modified MBSR program is an effective approach for nurses to decrease stress and negative affect and improve positive affect and resilience. In addition, the program has the potential to improve job satisfaction.
Nursing professionals face extraordinary stressors in the medical environment. The main sources of stress for nurses are workload, the emotional cost of caring, lack of reward and shift rotation, complex interpersonal relationships, and the increased need for knowledge of ever-changing technology (Botha, Gwin, & Purpora, 2015; Guillaumie, Boiral, & Champagne, 2017). Persistent high stress has a negative impact not only on the physical and mental health of nurses but also on work activities and performance, leading to burnout, compassion fatigue, lower job satisfaction, high workplace turnover, and poor quality of care for patients (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002; Howlett et al., 2015; Leiter & Maslach, 2009; McHugh, Kutney-Lee, Cimiotti, Sloane, & Aiken, 2011). Aiken et al. (2011), in a study of nurses from nine countries, reported that high nurse burnout was found in hospitals in all countries except Germany and ranged from roughly one third of nurses to approximately 60% of nurses in South Korea and Japan. Job dissatisfaction among nurses was close to 20% in most countries and as high as 60% in Japan. With regard to quality of care, half or more of the nurses surveyed, regardless of country, lacked confidence that their patients could care for themselves following discharge.
China is contending with a very serious nursing shortage compared with many other countries (Yun, Jie, & Anli, 2010). By the end of 2016, China reached a total of 3.5 million registered nurses (National Health and Family Planning Commission of the People’s Republic of China, 2016), but the increase in trained nurses was much lower than the increase in outpatient visits and inpatient numbers (Gu, 2011). Furthermore, nurses in China have frequently suffered from occupational stress owing to the speed of economic development and the new medical reform program, which have led to a higher demand for better medical services and a more complex nurse–patient relationship (Wu et al., 2011; Zhang et al., 2014).
The negative consequences of work-related stress among Chinese nurses are well characterized in the literature. Dong, Zhang, Sun, Sang, and Xu (2017) recently reported that the overall prevalence of sleep disturbances among clinical nurses in general hospitals in mainland China is 63.9%, which is higher than that in the general population (Chung & Tang, 2006; Gu, Xu, & Yin, 2015; Guo et al., 2005; Soldatos, Allaert, Ohta, & Dikeos, 2005; Wong & Fielding, 2011). According to a large study (n = 1,807) of Chinese nurses working in public hospitals, the prevalence rates of anxiety and depressive symptoms were 43.4% and 61.7%, respectively (Gao et al., 2012a, 2012b). In a separate study of 9,698 nurses from 181 hospitals in China, nearly 20% of the nurses reported high levels of burnout in the three dimensions of emotional exhaustion, depersonalization, and reduced personal accomplishment (Zhang et al., 2014). In addition, 54% of the nurses were dissatisfied with their current job, and 5% reported their intention to leave. These findings suggest that Chinese nurses have poor health prospects that may affect the quality and safety of nursing services, which ultimately influences the health of the population at large.
Mindfulness-Based Interventions (MBIs)
Mindfulness can be defined as the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally (Kabat-Zinn, 2003). The practice of mindfulness was originally developed in an Asian culture that emphasized the value of being, nonstriving, and acceptance of experience (Dundas, Thorsheim, Hjeltnes, & Binder, 2016). In the 1970s and 1980s, mindfulness was introduced to Western countries and gradually evolved into one of the most important concepts and techniques in contemporary psychotherapy (Hayes, Follette, & Linehan, 2004). In recent years, mindfulness practice, an effective way to reduce stress and improve health, has been widely applied in both clinical and nonclinical populations (Fjorback, Arendt, Ørnbøl, Fink, & Walach, 2011). The most widely known structured program for mindfulness practice is Mindfulness-Based Stress Reduction (MBSR; Kabat-Zinn, 1982; Kabat-Zinn, Lipworth, & Burney, 1985), which has inspired the development of several MBIs (Kabat-Zinn, 2003) worldwide, including Mindfulness-Based Cognitive Therapy (MBCT; Teasdale et al., 2000).
An increasing number of reports in the literature discuss the use of MBIs for health care professionals, especially nurses, who are an indispensable resource in patient care and are particularly vulnerable to work-related stress and burnout (Sillero & Zabalegui, 2018; Xie, Wang, & Chen, 2011; Zhang et al., 2014). In a recent mixed-methods systematic review (Guillaumie et al., 2017), the meta-analysis suggested that MBIs may be effective in significantly reducing anxiety and depression among nurses, and qualitative studies and uncontrolled studies have provided insight into the benefits overlooked in randomized controlled trials (RCTs), including improvements in the well-being of individuals and improved performance at work. A review (Hunter, 2016) using critical interpretative synthesis of five studies examining the impact of MBIs on nursing and midwifery practice indicated that mindfulness training enabled nurses and midwives to gain some control over their thoughts and stress levels, thereby creating a quiet mental space to give them perspective which led to improved care, including a more patient-centered focus, increased presence, and listening. Another literature review (Smith, 2014) outlined evidence to support that mindfulness training may be a promising intervention to decrease stress, anxiety, and burnout and improve focus, empathy, self-care, and mood. In addition, given the demanding nature and busy schedule of nurses’ work, a few studies have analyzed the effects of adapted MBSR, which was divided into three categories: modified traditional MBSR, abbreviated MBSR, and nontraditional mindfulness training (Luken & Sammons, 2016). For example, Mackenzie, Poulin, and Seidman-Carlson (2006) found significant improvements in burnout symptoms, relaxation, and life satisfaction among nurses and nurse aides after a brief 4-week mindfulness intervention. Similarly, Duchemin, Steinberg, Marks, Vanover, and Klatt (2015) found that a workplace-modified MBI for surgical intensive care unit workers (nurses represented 69% of the participants) was positively associated with reductions in indicators of stress and burnout. Furthermore, a study by Wylde, Mahrer, Meyer, and Gold (2017) delivered MBIs through smartphone applications to a group of novice nurses. This nontraditional mindfulness training showed promise in equipping nurses with important coping skills to manage stress.
Although an increasing number of studies have demonstrated that MBIs can reduce stress and improve health and work performance among nurse professionals, there is still a paucity of rigorous studies exploring the effectiveness of MBIs in Chinese nurses. The aim of this study was to evaluate the effects of a modified MBSR program on levels of stress, affect, and resilience among nurses in general hospitals in mainland China. In addition, the study attempted to determine the impact on nurses’ job satisfaction. We hypothesized that, compared with a wait-list comparison group, participants receiving mindfulness training would experience (a) decreased perceived stress, (b) decreased negative affect, (c) increased positive affect, (d) increased resilience, and (e) increased job satisfaction.
Method
This study utilized a randomized controlled design. Eligible participants were randomized 1:1 using a computer-generated random number table to the intervention group or the wait-list control group. The intervention group was given a modified 8-week MBSR program, and the control group was not given an intervention, but was offered the option to participate in the same program immediately after the study. Assessments were performed for all participants of both groups at baseline, immediately after the intervention, and again at the 3-month follow-up.
Setting and Sample
Two hospitals were selected from seven tertiary-level general hospitals by convenience sampling in Dongguan, South China. In mainland China, hospitals are divided into three levels based on their staffing, function, and technology. A third-level hospital is considered a general and sophisticated hospital, providing high-quality service and a high level of education and research across regions. Once the hospitals were selected, a notice was issued through the hospital mobile platform to invite nurses for voluntary participation in the study, and the subjects were screened after the Ethical Committee of Xiangya Nursing School granted approval (approval number 2015078).
The inclusion criteria included being employed as a full-time nurse. The exclusion criteria were as follows: (a) being a student nurse, (b) suffering from serious somatic disease, (c) taking mood-regulating drugs, (d) having suffered a major traumatic event in the past 6 months, and (e) having participated in mindfulness training previously. Ultimately, 110 nurses provided informed consent, enrolled in the training program, and were randomly divided into the intervention group (n = 55) and the control group (n = 55).
Intervention
The program was an 8-week mindfulness-based group intervention generally based on the principles and exercises of MBSR (Kabat-Zinn, 1990) and MBCT (Teasdale et al., 2000). Although MBCT is derived from MBSR, it incorporates some elements of cognitive-behavioral therapy and places greater emphasis on promoting enhanced awareness of one’s relationship with thoughts and feelings, which facilitates coping with a painful affect and challenging circumstances (Sipe & Eisendrath, 2012). A traditional MBSR program developed by Kabat-Zinn consists of eight weekly group sessions lasting for 2.5 hours, 45 minutes of home-based practice daily, and one half-day retreat (6 hours of formal mindfulness training) between the sixth and seventh weeks. To address the time constraints of nurses, we modified the length of the weekly group sessions and the daily home-based practice and did not include a half-day retreat. Therefore, the final manualized intervention consisted of eight 2-hour weekly group sessions and 20 minutes of formal mindfulness practice at home daily for 6 days a week for 8 weeks. The weekly group sessions were facilitated by an MBSR instructor and included guided practice, education, and dialogues around participants’ observations of their feelings, thoughts, and body sensations during practice. The specific content of program is shown in Table 1. In addition, we set up a network Chatgroup through WeChat (Tencent Inc., China) on mobile phones, sending session PowerPoint slides and audio recordings of guided mindfulness exercises, which helped the participants to share their practice experience or to ask the MBSR instructor questions.
Overview of the MBSR Program
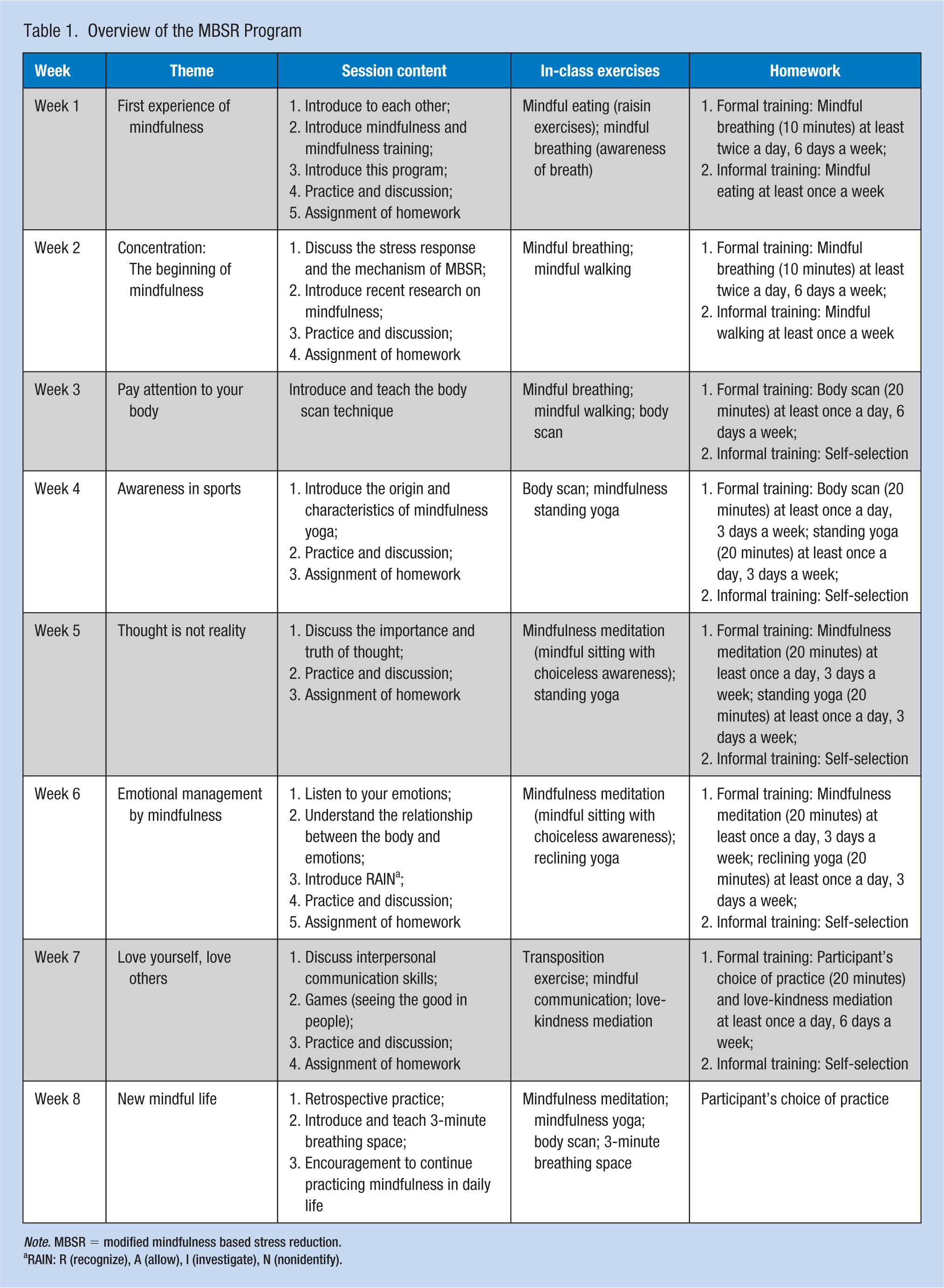
Note. MBSR = modified mindfulness based stress reduction.
RAIN: R (recognize), A (allow), I (investigate), N (nonidentify).
Procedures
The modified program used in this study was conducted by a researcher who has been practicing mindfulness for 2 years and attended several MBSR courses, retreats, and other training activities related to mindfulness and meditation. Pretest, posttest, and tracking measurements were performed by research assistants who were trained in program management procedures and methods and in the measurements. Prior to the intervention, strong support was received from the nursing department of each hospital, and the session calendar was released to nurses in advance to facilitate the nurses’ scheduling.
The group intervention occurred for 8 weeks from April 25, 2017 to June 16, 2017. As the intervention group included 55 nurses, it was divided into two groups. Group 1 included 30 nurses who attended sessions at 15:00 to 17:00 every Tuesday afternoon, and Group 2 included 25 nurses who attended sessions at 15:00 to 17:00 every Friday afternoon. The participants in both Group 1 and Group 2 were guided by the same instructor, and the content and length of the sessions were identical. During the 8-week sessions, research assistants recorded the attendance of the members of the intervention group. If a participant was absent more than two times, the participant was classified as a dropout from the intervention. In addition, through the WeChat group, we urged the nurses to attend their sessions on time, to complete home-based practice, and to fill out the questionnaires, but home-based practice was not mandatory and was not assessed. The control group also had a WeChat group for connection and to send questionnaires. Upon completion of the program, the participants were incentivized with continuing education (CE) credits if they attended at least 50% of the group sessions.
Data Collection
Social demographic data were collected at baseline, including age, gender, education, professional title, marital status, duration of employment, and work during the night shift or not. In addition, a battery of questionnaires was used for the evaluations at baseline (T0), immediately after the intervention (T1), and at the 3-month follow-up (T2). Researchers sent a link to the online questionnaires through the WeChat group. Before completing the questionnaires, the participants were informed of the purpose of the study, the scoring methods, and matters needing attention. The participants completed and submitted the questionnaires on the day they were issued, and the researchers checked the quality of the submitted questionnaires, verifying them immediately if there was any doubt.
Effectiveness of the intervention was measured via data collection at the three specific time periods, which pertained to the worker’s perceived stress, positive and negative affect, resilience, and job satisfaction. The following is a description of the specific scales used.
Perceived Stress Scale (PSS)
The PSS (Cohen, Kamarck, & Mermelstein, 1983) is a 14-item self-report tool that provides a global measure of perceived stress. This study adopts the Chinese version revised by Prof. Yang Tingzhong, which has good reliability and validity (Yang & Huang, 2003). The scale consists of 14 items reflecting stress and loss of control, and responses range on a 5-point scale from never to very often. A higher score indicates greater stress. The internal consistency (Cronbach’s alpha) of the PSS was .802 in this study.
Positive and Negative Affect Schedule (PANAS)
Watson, Clark, and Tellegen (1988) developed the PANAS, and Huang, Yang, & Li (2003) established a Chinese version with satisfactory validity and reliability. The PANAS is a self-report instrument that measures positive and negative affect. The instrument consists of a list of 20 adjectives, 10 per subscale, to be rated on a 5-point scale within the time constraints established by the researcher. In this study, the Cronbach’s alphas were .861 for the positive affect subscale and .834 for the negative affect subscale.
Connor–Davidson Resilience Scale (CD-RISC)
The CD-RISC (Connor & Davidson, 2003) was developed in the United States to measure individuals’ ability to cope effectively when faced with adversity. The present study adopted the Chinese version revised by Yu and Zhang (2007), which has good reliability and validity. The revised scale includes 25 items and three dimensions (tenacity, strength, and optimism). Each item is rated on a Likert-type scale ranging from 0 (not at all) to 4 (almost always). The range of possible total scores is 0 to 100, with higher scores indicating higher levels of resilience. In this study, the Cronbach’s alpha of the CD-RISC was .895.
The McCloskey/Mueller Satisfaction Scale (MMSS)
Mueller and McCloskey (1990) developed the MMSS, and He, Zhang, and Bai (2008) established a Chinese version with satisfactory validity and reliability. The MMSS is a 31-item scale that measures hospital nurses’ job satisfaction. The scale measures eight types of satisfaction: extrinsic rewards, scheduling, family and work balance, coworkers, interactions, professional opportunities, praise and recognition, and control and responsibility. Responses were coded on a Likert-type scale ranging from 1 (very dissatisfied) to 5 (very satisfied). The possible range of total scores is 31 to 155, with higher scores indicating greater job satisfaction. In this study, the Cronbach’s alpha of the MMSS was .934.
Data Analysis
A data analysis was performed using SPSS 22.0 (IBM Corp., Armonk, NY, USA). All statistical tests were two-tailed, and the significance level was set at p < .05. The demographic data of the two groups were compared by Student’s t test or the chi-square test. The effects of the intervention as indicated by changes in the outcome variables (perceived stress, positive affect, negative affect, resilience, and job satisfaction) were analyzed using 2 (groups) × 3 (times) repeated-measures ANOVA. When the data did not satisfy the hypothesis of spherical symmetry, the F values from the ANOVA were corrected by the Greenhouse–Geisser method. If no significant group effect but a significant effect of the Group × Time interaction was observed, then a simple effects analysis was performed. First, an independent-sample t test was used to compare the two groups within each time point. Second, one-way ANOVA was used to compare the three time points within each group, and the least significant difference (LSD) method was used for multiple comparisons.
Results
In the intervention group, 11 participants missed the weekly sessions more than twice. In the control group, six participants did not complete the questionnaire, and three participants submitted invalid questionnaires. Therefore, the effective sample size was 90, including 44 in the intervention group and 46 in the control group. No significant differences were observed between the two groups for any of the demographic characteristics (see Table 2).
Demographic Characteristics of Study Participants (N = 90)
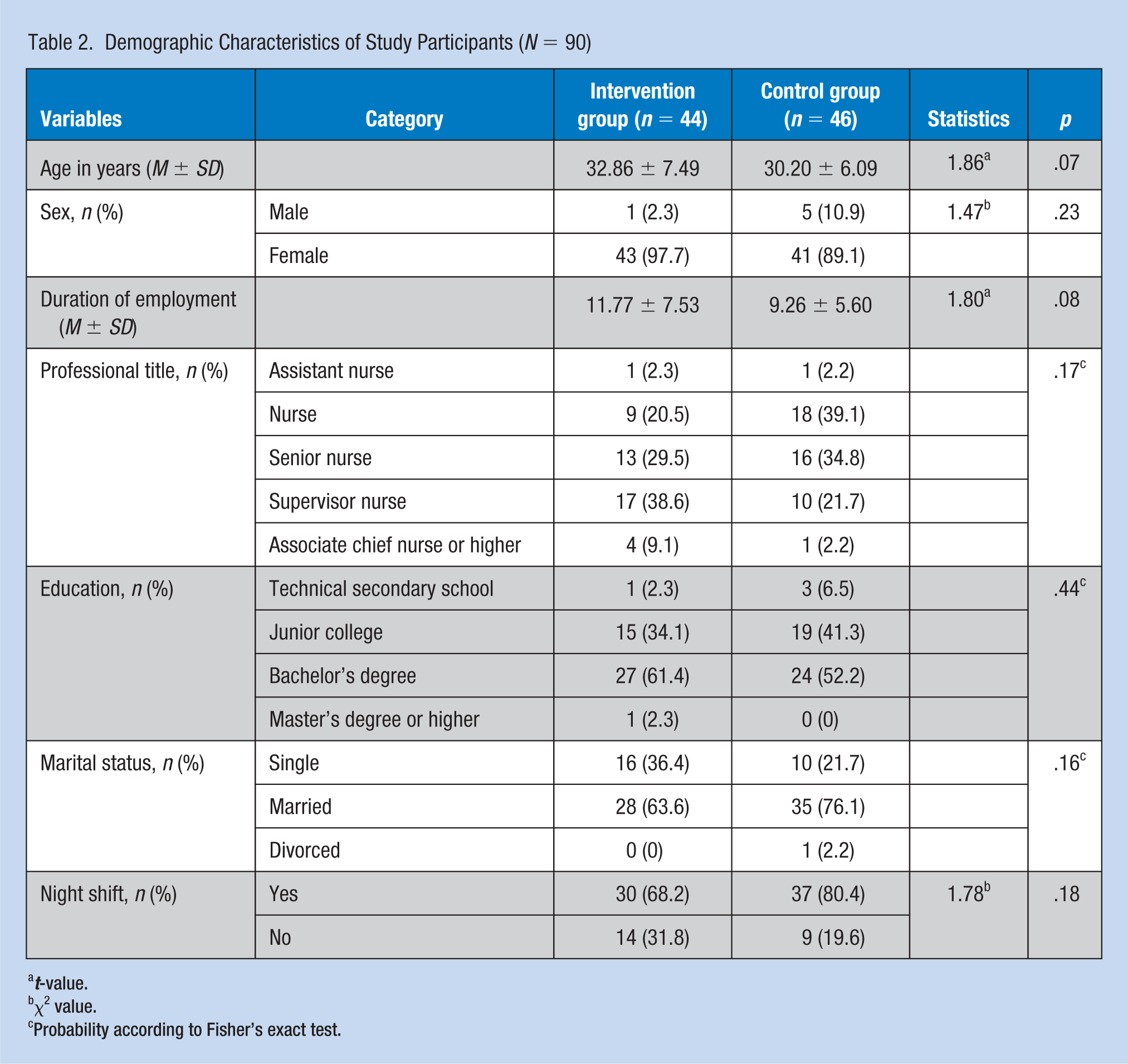
t-value.
χ2 value.
Probability according to Fisher’s exact test.
Repeated-measures ANOVA showed that the group effect was not significant (p > .05), but statistically significant effects of time and the Group × Time interaction on perceived stress, positive affect, and negative affect were observed between the two groups at baseline (T0), immediately after the intervention (T1), and at the 3-month follow-up (T2; p < .05; Table 3). No significant effect of group or time on resilience was identified between the two groups (p > .05), but the effect of the Group × Time interaction on resilience was statistically significant (p < .05). No significant effect of group or time or the Group × Time interaction on job satisfaction was identified between the two groups (p > .05), but the trends of the data were in the hypothesized direction.
Comparisons of Outcomes Between Nurses That Received the MBSR Intervention and the Control Group Over Three Time Periods (n = 90)
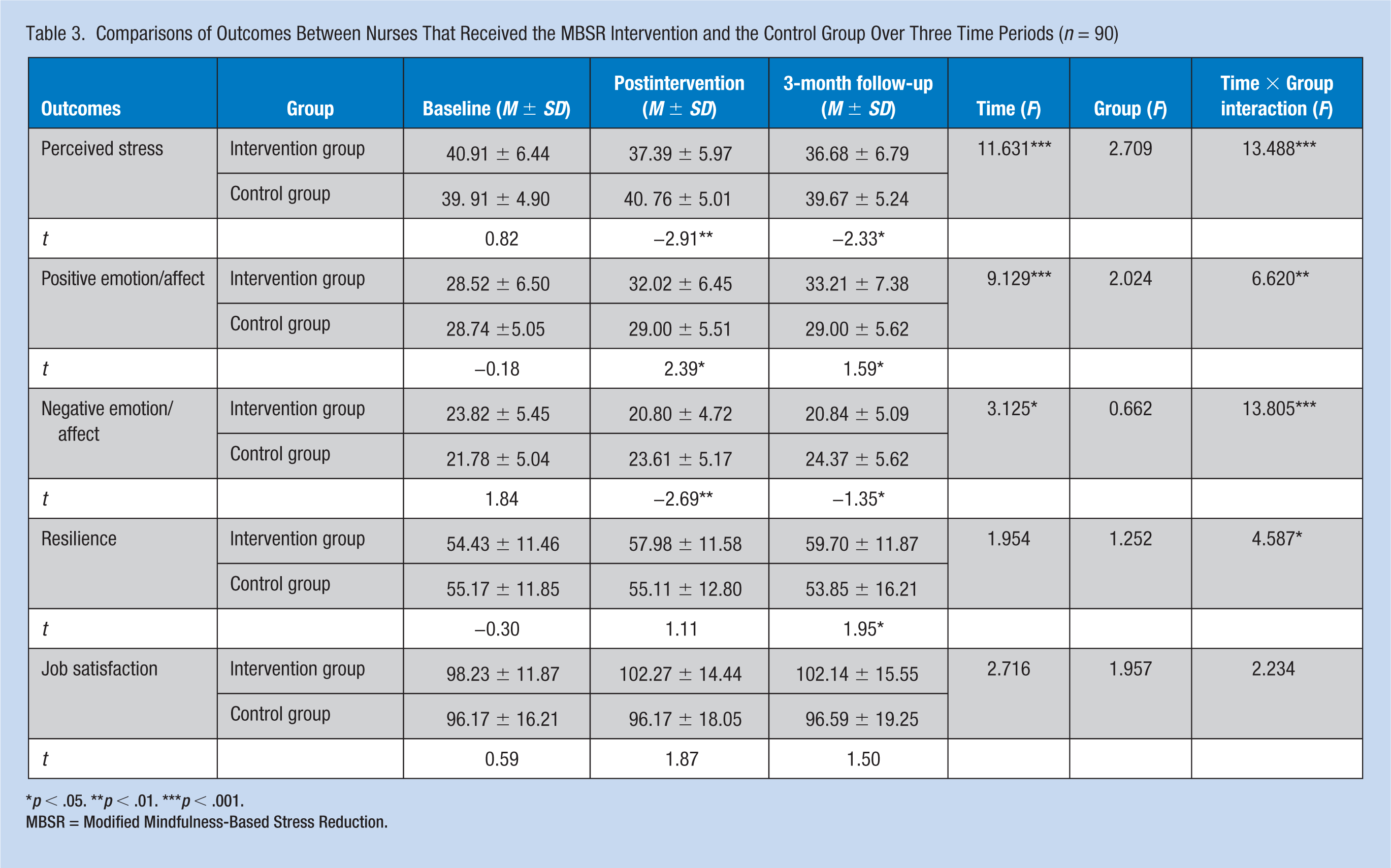
p < .05. **p < .01. ***p < .001.
MBSR = Modified Mindfulness-Based Stress Reduction.
The results of the simple effects analysis (independent-samples t tests and one-way ANOVA) were as follows: First, when the time points were fixed, no significant differences in perceived stress, positive affect, negative affect, or resilience were noted between the two groups at baseline (p > .05), but significant differences were found in perceived stress, positive affect, and negative affect between the two groups immediately after the intervention and at the 3-month follow-up (p < .05), and significant differences in resilience were found between the two groups at the 3-month follow-up (p < .05; see Table 3). When the groups were fixed, no significant differences were found in perceived stress, positive affect, negative affect, or resilience across different time points in the control group (p > .05; Table 4); when different time points were compared in the intervention group, the levels of perceived stress, positive affect, and negative affect were significantly different between T0 and both T1 and T2 (p < .05), and the levels of resilience were significantly different between T0 and T2 (p < .05).
The Examination of the Effects of MBSR Within Groups: Intervention and Control (N = 90)
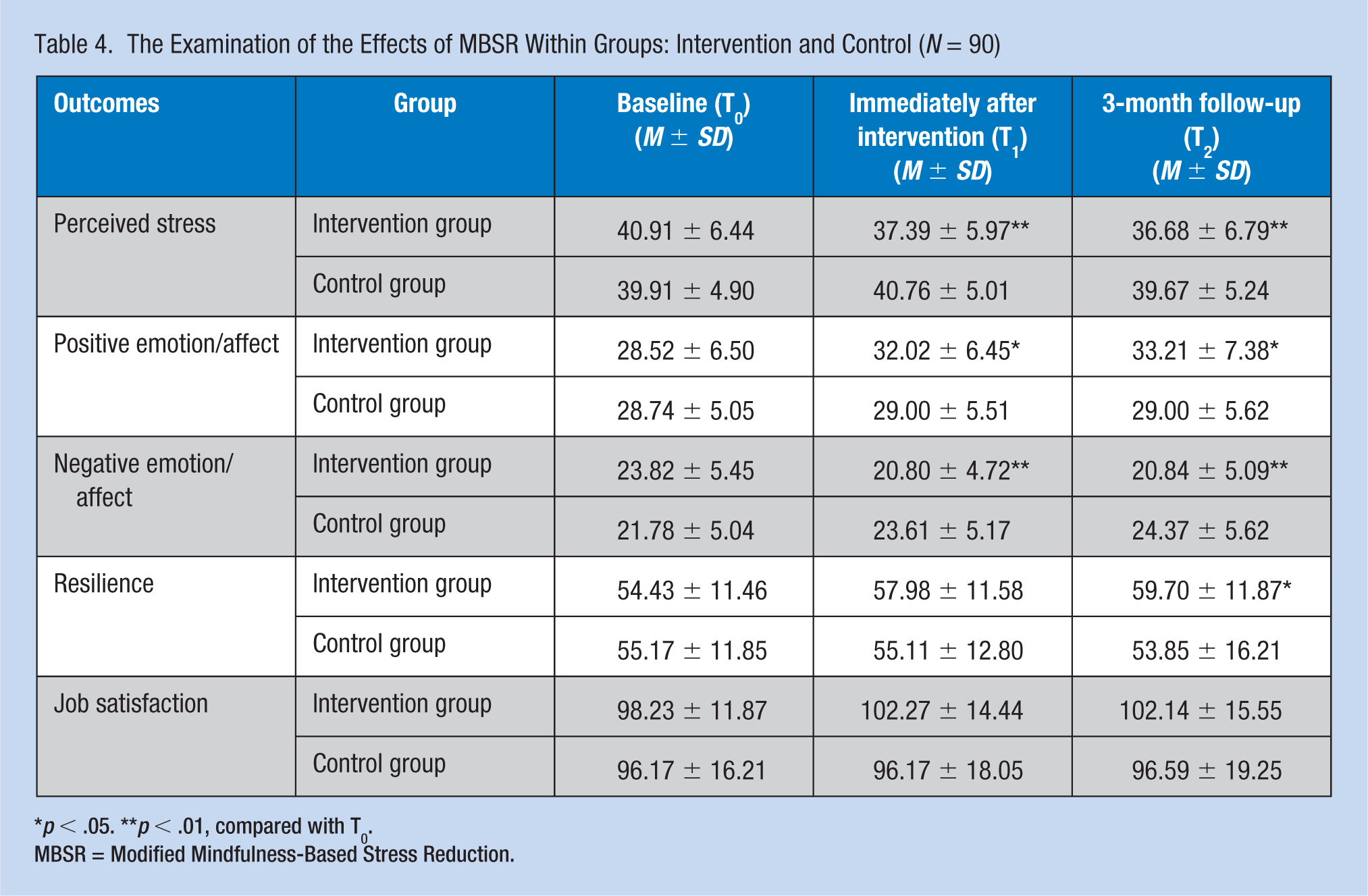
p < .05. **p < .01, compared with T0.
MBSR = Modified Mindfulness-Based Stress Reduction.
Discussion
To the best of our knowledge, this is the first study to investigate the effectiveness of a modified MBSR program with respect to the stress, affect, resilience, and job satisfaction of nurses in general hospitals in mainland China. There was a significant improvement in perceived stress, negative affect, and positive affect immediately after the intervention and at the 3-month follow-up. The results were consistent with those of similar previous studies. For example, studies with mixed samples of health care staff reported improvements in stress reduction (Fortney, Luchterhand, Zakletskaia, Zgierska, & Rakel, 2013; Goldhagen, Kingsolver, Stinnett, & Rosdahl, 2015). Studies with nurses have also found that participating in an MBI leads to decreases in perceived stress (Bazarko, Cate, Azocar, & Kreitzer, 2013; Dos Santos et al., 2016; Spadaro & Hunker, 2016) and negative affect (Craigie et al., 2016) and increases in positive affect (Demarzo et al., 2017). Mindfulness emphasizes continuous, nonjudgmental attention to the internal and external stimuli present at the moment, which helps nurses enhance their experience, cultivate self-compassion, and avoid becoming trapped in a negative affect or preoccupied by thoughts caused by stress (Hunter, 2016; Kabat-Zinn, 1990). When negative affect or thoughts appear, mindfulness enables one to observe and describe them with an accepting attitude, allowing them to fade away gradually. Thus, mindfulness helps nurses to cope with stress in healthier and adaptive ways rather than through habitual and often maladaptive reactions. Several studies (Davidson & McEwen, 2012; Flook, Goldberg, Pinger, Bonus, & Davidson, 2013; Lutz, Slagter, Dunne, & Davidson, 2008) have also suggested that mindfulness has a positive effect on brain areas associated with attention regulation and emotional adaptation and that this is the physiological and neuroscientific basis of stress reduction associated with MBIs.
Changes in resilience did not offer significant results immediately after the intervention, but the changes were statistically significant at the 3-month follow-up. The results were similar to those of Pidgeon, Ford, and Klaassen (2014), who used an RCT to evaluate the effects of a retreat-based Mindfulness with Metta Training Program on human service professionals’ mindfulness, self-compassion, and resilience. The study found no significant difference in resilience between the intervention and control groups immediately after the intervention, but significant improvement was observed at the 4-month follow-up. Resilience, defined as competency to cope and adapt in the face of adversity, is considered a significant protective factor against the negative effects of job stress (Hart, Brannan, & De Chesnay, 2014). An individual’s power of resilience is not fixed but is very complicated and related to a large number of influences, including demographic features, personal traits, and environmental factors (Guo et al., 2017). MBIs are based primarily on strengthening intrapersonal factors to enhance resilience (Grafton, Gillespie, & Henderson, 2010), which is a gradual and complex process that needs to be founded on changes in related factors such as mindfulness (Pidgeon et al., 2014), self-compassion (Pidgeon et al., 2014), and positive affect (Lord, Rumburg, & Jaser, 2015). Therefore, the development of resilience requires time and it is difficult to observe positive changes immediately after an intervention, which has also been confirmed by two other studies (Craigie et al., 2016; Demarzo et al., 2017).
Regarding job satisfaction, we found no significant improvement either immediately after the intervention or at the 3-month follow-up, but the trends of the data were in the hypothesized direction. This result is not surprising to us because job satisfaction is a very complex and multifactorial construct (Silva, Velasque, & Tonini, 2017) that a modified MBSR program might not sufficiently improve in a short period of time. A mixed-methods systematic review (Guillaumie et al., 2017) indicated that only a few studies have explored the effect of mindfulness on organizational changes (e.g., patient satisfaction, job satisfaction, turnover, and absenteeism) at nurses’ work, and the meta-analysis revealed no significant impact on job satisfaction, which is similar to our findings. Future research should focus on organization-related variables and further explore the long-term impacts of MBIs on nurses’ job satisfaction.
Overall, these results suggest that the modified MBSR program may help nurses manage stress and improve their affect, resilience, and job satisfaction in Chinese hospital settings.
Strengths and Limitations
This study has several strengths. First, there is still a paucity of studies exploring the use of MBIs for Chinese nurses and the associated effects on stress, affect, resilience, and job satisfaction, and this study therefore addresses a major scarcity in the field. Second, this study assessed the effectiveness of a modified MBSR that may be more adaptive to busy professionals working in stressful conditions such as nurses. The program combined elements of MBSR and MBCT, not only teaching and practicing basic skills such as mindful breathing, yoga, meditation, body scan, and 3-minute breathing space but also discussing self-care and mindful communication as well as exploring the relationship between an individual and his or her own thoughts and affect, which helps nurses cope more effectively with stress and negative affect in their work. Third, although the modified version of the program was 8 weeks long, paralleling the traditional MBSR, the weekly group sessions and daily home-based practice were shorter and a half-day retreat was not included, allowing the intervention to more easily fit into the schedules of hospital nurses. Finally, a WeChat group on mobile phones was established to facilitate communication between instructors and trainees after group sessions, which is a very flexible, convenient, and time-efficient strategy to supplement the main interventions.
The study is not without limitations. The hospitals in this study are third-level general hospitals in the city and were selected by convenience sampling, which affected the representativeness of the sample to a certain extent. In addition, the sample size was relatively small (n = 90), warranting a larger randomized control trial to confirm the results. In addition, the modified program was evaluated in this study primarily using quantitative methods by self-reported questionnaires. Although we collected some qualitative data, including the participants’ WeChat sharing records and reports of learning experiences at the end of the intervention, no qualitative interviews and no in-depth analyses of the data were carried out. Because qualitative research is the best way to unpack the mechanisms of MBI benefit on nurses’ work performance, enabling an open and inductive inquiry (Hunter, 2016), future research should combine quantitative and qualitative methods to explore the effect of MBIs in a more comprehensive and deeper way. Moreover, although the training program has been simplified from traditional MBSR, 20% of the intervention group (n = 11) did not complete the weekly sessions, and most of them did not finish the homework as required owing to a lack of time (according to reports of learning experiences); this noncompliance reduces the effectiveness of the intervention to a certain extent. Some attempts have been made to increase the feasibility and accessibility of MBIs while maintaining their efficacy, adapting them to specific target populations and contexts. However, many questions remain unanswered, such as the minimum number and length of sessions and daily practice required to maintain effectiveness and the types and order of the therapeutic components and mindfulness exercises to be included (Demarzo et al., 2017). Therefore, future work should focus on identifying the above factors to develop the shortest and most effective program available and to improve the accessibility of such programs to a larger number of health care professionals with high levels of job stress.
Implications for Practice
In this study, an RCT combining within-group and between-group comparisons was used to evaluate the effects of the modified MBSR program. The results showed that this program was an effective approach to improving the levels of stress, affect, and resilience among nurses in Chinese hospital settings. In addition, the program has the potential to improve nurses’ job satisfaction. Although further research is necessary, the results have some implications for nursing practice and education. First, as an effective strategy to reduce stress and improve health, the modified MBSR program or other MBIs can be integrated into short-term or long-term health promotion plans for nurses. Second, nursing educators should recognize the importance of mindfulness and incorporate it into the nursing curriculum, which can help improve resilience among nursing students when they enter the clinical environment.
Applying Research to Practice
This randomized clinical trial provides evidence that a modified MBSR program is a promising approach for nurses to improve stress, affect, resilience, and job satisfaction. Although further research is necessary, the results have some implications for nursing practice and education. First, as an effective strategy to reduce stress and improve health, the modified MBSR program or other MBIs can be integrated into short-term or long-term health promotion plans for nurses. Second, nursing educators should recognize the importance of mindfulness and incorporate it into the nursing curriculum, which can help improve resilience among nursing students when they enter the clinical environment.
Footnotes
Acknowledgements
We thank the nurse executives and staff nurses of the study hospitals for their participation in our study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the General Program of Science and Technology Plan for Health Care in Dongguan City of Guangdong Province (2016105101286). The funder played no role in the study design, data collection, data analysis, manuscript preparation, or decision to publish the report.
Author Biographies
Lin Lin is a PhD student in Xiangya Nursing School of Central South University and a Lecturer in the Nursing School of Guangdong Medical University.
Guoping He is a professor and doctoral supervisor in the Xiangya Nursing School of Central South University.
Jin Yan is a clinical nursing specialist and works as Director of Nursing Department in The Third Xiangya Hospital of Central South University.
Can Gu is an associate professor in the Xiangya Nursing School of Central South University, Her research interests in cancer care and long-term care.
Jianfei Xie is a clinical nursing specialist and works as ICU head nurse in The Third Xiangya Hospital of Central South University.