
Abstract
Nurses have a high prevalence of musculoskeletal symptoms from patient handling tasks such as lifting, transferring, and repositioning. Comorbidities such as musculoskeletal symptoms may negatively affect engagement in leisure-time physical activity (LTPA). However, limited data are available on the relationship between musculoskeletal symptoms and LTPA among nurses. The purpose of this study was to describe musculoskeletal symptoms and LTPA, and to examine the relationships of musculoskeletal symptoms, sociodemographics, and body mass index with LTPA among nurses. Cross-sectional data on sociodemographics, employment characteristics, musculoskeletal symptoms, body mass index, and LTPA were collected from a statewide random sample of 454 California nurses from January to July 2013. Descriptive statistics, bivariate and multiple logistic regressions were performed. We observed that non-White nurses were less likely to engage in regular aerobic physical activity than White nurses (odds ratio [OR] = 0.61; 95% confidence interval [CI] = [0.40, 0.94]). Currently working nurses were less likely to engage in regular aerobic physical activity than their counterparts (OR = 0.48; 95% CI = [0.25, 0.91]). Nurses with higher body mass index were less likely to perform regular aerobic physical activity (OR = 0.93; 95% CI = [0.89, 0.97]) or muscle-strengthening physical activity (OR = 0.92; 95% CI = [0.88, 0.96]). This study found no evidence that musculoskeletal symptoms may interfere with regular engagement in LTPA. Physical activity promotion interventions should address employment-related barriers, and particularly target racial minority nurses and those who have a high body mass index.
Keywords
Introduction
Regular physical activity has many health benefits, including the reduced risk of obesity, Type 2 diabetes, and some types of cancer, as well as improving mental health (Centers for Disease Control and Prevention [CDC], 2013; Dunn, Trivedi, & O’Neal, 2001; Kesaniemi et al., 2001). In 2015, however, only 51% of U.S. adults met the 2008 physical activity guidelines for aerobic activity, and 21% met the guidelines for both aerobic and muscle-strengthening activities (CDC, 2016b). A recent study of nurses found that many nurses did not participate in leisure-time physical activity (LTPA) on a regular basis: Only 41% met the recommended level of aerobic physical activity (Chin, Nam, & Lee, 2016). This raises concerns because physical inactivity is a risk factor for obesity, and nurses—the largest healthcare occupational group—have a high obesity rate of 30% to 55% (Chin et al., 2016; Han, Trinkoff, Storr, & Geiger-Brown, 2011). Lack of LTPA may also result in low productivity in the workplace (Goetzel et al., 2010; Tucker, Harris, Pipe, & Stevens, 2010).
Physically demanding nursing jobs which involve long work hours and shift work schedules may contribute to low levels of LTPA among nurses (Chin et al., 2016; Han, Trinkoff, & Geiger-Brown, 2014). Studies suggest that occupational physical activity and LTPA may not provide the same health benefits with mixed results (Allman-Farinelli, Chey, Merom, & Bauman, 2010; Gutiérrez-Fisac et al., 2002; Martin, Nieto, Ruiz, & Jimenez, 2008). Some studies have shown that occupations involving moderate to high levels of physical activity are associated with low body mass index (BMI; Church et al., 2011; G. A. King et al., 2001; Steeves, Bassett, Thompson, & Fitzhugh, 2012), while other studies have shown that high levels of occupational physical activity are associated with a high BMI (Gutiérrez-Fisac et al., 2002; Jang, Kim, Lee, Myong, & Koo, 2014; Kaleta, Makowiec-Dabrowska, & Jegier, 2007; McLaren & Godley, 2009; Singer et al., 2016). The risk of not taking up LTPA was higher among individuals who expended more calories per week on occupational physical activity or individuals with high job strain (Kaleta et al., 2007; Kouvonen et al., 2005).
Nurses have a high prevalence of musculoskeletal symptoms from physically demanding tasks (S. J. Lee, Lee, & Gershon, 2015), which could be a potential barrier for nurses to participate in LTPA. A recent systematic review of 132 studies of nursing workers reported that on average, 55% experienced low back symptoms in the previous year, 44% had low back symptoms in the previous 3 to 6 months, and 35% had current low back symptoms (Davis & Kotowski, 2015). Studies of young nursing students or dentists showed that musculoskeletal symptoms may negatively affect engagement in LTPA (Backaberg, Rask, Brunt, & Gummesson, 2014; Feng, Liang, Wang, Andersen, & Szeto, 2014). Frequent or severe musculoskeletal symptoms can interfere with an individual’s LTPA by causing limitation or discomfort related to physical activity (Backaberg et al., 2014). Nonetheless, there is little research on the relationship between musculoskeletal symptoms and LTPA among nurses.
Sociodemographic characteristics have also been shown to be related to LTPA. In a review of physical activity from diverse racial/ethnic groups, women had lower rates of engagement in LTPA than men, and racial/ethnic minority women such as Blacks, Asians, and Hispanics reported lower rates of LTPA engagement than White women (Eyler et al., 2002). Findings on the relationship between age and LPTA were mixed. An inverse relationship between age and physical activity was found in White and Black women but not among men (Eyler et al., 2002). Another study showed that age was not associated with LPTA in Blacks and Whites (A. C. King et al., 2000).
The relationship between BMI and LTPA in many studies in the general population appears to be bidirectional. In longitudinal studies, individuals who were sedentary or had a lack of LTPA had increased odds of developing obesity than their counterparts (Morseth, Jacobsen, Emaus, Wilsgaard, & Jorgensen, 2016; Su et al., 2017). Also, individuals with high BMI engaged less in LTPA than individuals with normal BMI, in part due to more perceived barriers to LTPA, such as low exercise self-efficacy and comorbid conditions (Morseth et al., 2016; Schutzer & Graves, 2004).
Understanding the relationship between musculoskeletal symptoms and LTPA among nurses, and other risk factors of their LTPA could help guide future workplace wellness programs to improve health among nurses. Therefore, the purpose of this study was twofold: (a) to describe musculoskeletal symptoms and LTPA levels among nurses, and (b) to examine the relationships of musculoskeletal symptoms, sociodemographics, and BMI with LTPA among nurses. Based on our literature review, we hypothesized the following:
Method
Design, Sample, and Procedures
A statewide cross-sectional survey of registered nurses in California was conducted from January to July 2013. A mail survey was sent to 2,000 nurses randomly selected from a 2012 list of actively licensed nurses by the California Board of Registered Nursing. The survey packet contained an information letter, informed consent, and a study questionnaire. Respondents were also given an alternative response option of online completion following log-in information provided in the study information letter. Postal reminders were sent at 2-week intervals up to 4 times. As a reward for participation, 20 respondents selected through random drawing received a US$50 gift card. All study protocols were approved by the Institutional Review Board of University of California, San Francisco prior to implementation.
Variables and Instruments
Sociodemographics included age, gender, race/ethnicity, and education. Employment status was categorized as working, not working, retired, and student; and then dichotomized into working versus not working, which included retirees and students. Workplace and employment factors included type of workplace (e.g., hospital), job title (e.g., staff nurse), work status (e.g., full-time), work shift (e.g., day), hours worked per shift, and hours worked per week.
Physical activity variables included leisure-time aerobic physical activity and muscle-strengthening physical activity. The questions were adapted from the Behavioral Risk Factor Surveillance System (CDC, 2016a). Aerobic physical activity was measured by the following two questions: “During the past month, other than your regular job, how many times per week did you take part in any physical activities or exercises such as running, calisthenics, golf, gardening, or walking for exercise?” Those who reported at least 1 day were then asked, “When you took part in this activity, for how many minutes did you usually keep at it?” Using the two questions, the total number of minutes per week of aerobic physical activity was calculated by multiplying the frequency of physical activity per week by the number of minutes spent on physical activity. Based on the 2008 Physical Activity Guidelines for Americans (U.S. Department of Health and Human Services [USDHHS], 2008), regular aerobic physical activity was defined as engaging in at least 150 minutes per week of aerobic physical activity. Muscle-strengthening physical activity was measured by asking, “During the past month, other than your regular job, how many times per week or per month did you do physical activities or exercises to strengthen your muscles?” Regular muscle-strengthening physical activity was defined as performing muscle-strengthening physical activity 2 or more days a week (USDHHS, 2008).
BMI was calculated by weight in kilograms divided by height in meters squared (kg/m2), and categorized as underweight (<18.5 kg/m2), normal (18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), or obese (≥30 kg/m2; CDC, 2012).
Musculoskeletal symptoms were assessed by questions adapted from the validated Nordic Musculoskeletal Questionnaire (Kuorinka et al., 1987; Trinkoff, Lipscomb, Geiger-Brown, & Brady, 2002). Respondents were asked whether they had pain, aching, stiffness, burning, numbness, or tingling in the low back, neck, shoulders, or hands/wrists in the past 12 months. Subsequent questions for reported symptoms included frequency, duration, and severity of symptoms. Major symptoms were defined as moderate or severe symptoms that either occurred at least monthly, or lasted for 1 week or longer. This definition was based on the method by Trinkoff et al. (2002). A musculoskeletal symptom index was created as an aggregate measure of symptoms in the low back, neck, shoulders, or hands/wrists. One point was assigned for each of the following criteria: (a) the intensity of symptoms was at least moderate, (b) the duration was at least 1 week, and (c) the frequency was at least monthly. The musculoskeletal symptom index was the sum of points for all four body regions, ranging from 0 (no symptoms) to 12 (maximum symptoms).
Statistical analysis
Descriptive statistics were used to summarize study variables. Values for continuous variables were presented as means and standard deviations (SD); categorical variables were summarized by frequencies and percentages. The prevalence of regular LTPA (aerobic and muscle-strengthening physical activities) was described by sociodemographics, musculoskeletal symptoms, and BMI. Logistic regression analyses were conducted to examine the relationships of sociodemographics, musculoskeletal symptoms, and BMI with aerobic physical activity and muscle-strengthening physical activity. To identify potential confounders and to avoid multicollinearity problems in multivariable analysis, several logistic models were tested and compared. Covariates with p < .10 in bivariate analysis were retained in the multivariable models. Correlations of ≥.80 between independent variables, tolerance of ≤0.1, and variance inflation factors (VIFs) of >5 were considered indicative of multicollinearity (Stevens, 2009).
We assessed model fit using the Hosmer–Lemeshow test, and assessed the degree of unique variability accounted for by using Cox and Snell R2 and Nagelkerke R2. Categorical variables were dichotomized, considering the distributions and bivariate findings. The odds ratios (ORs) and 95% confidence intervals (CIs) were obtained from the logistic regression models. All hypothesis testing was two sided; Type I error was controlled at the .05 significance level.
Results
Of 2,000 nurses who received a mail survey, 528 actively licensed registered nurses responded (response rate = 26.4%) and 468 nurses answered the physical activity questions. We excluded 14 nurses on disability leave due to pregnancy or other medical conditions because their conditions of disability could confound results on musculoskeletal symptoms and LTPA prevalence. The final sample for this study was 454 nurses.
The majority of participants were women (91.2%) and non-Hispanic White (65.2%) with a mean age of 49.6 years (SD = 13.1). Of the participants, 86.8% (n = 394) were currently working; of these working nurses, 61.4% worked in hospital settings, 81.7% worked as staff nurses, and 69% worked full-time (Table 1). The principal work schedules were reported as follows: 65.0% day shift, 6.3% evening shift, 18.8% night shift, and about 10% either rotating shift or did not answer. Mean working hours per week was 37.5 hours (SD = 11.9). Among not-working nurses (n = 60), 39 were retirees, one reported as a student, and 20 reported currently not working. The mean BMI was 25.6 kg/m2 (SD = 4.8); 47.7% were overweight or obese. For physical activity among all nurses, 44.1% engaged in regular aerobic physical activity and 55.8% performed regular muscle-strengthening activity.
Sample Characteristics of California Nurses (n = 454)
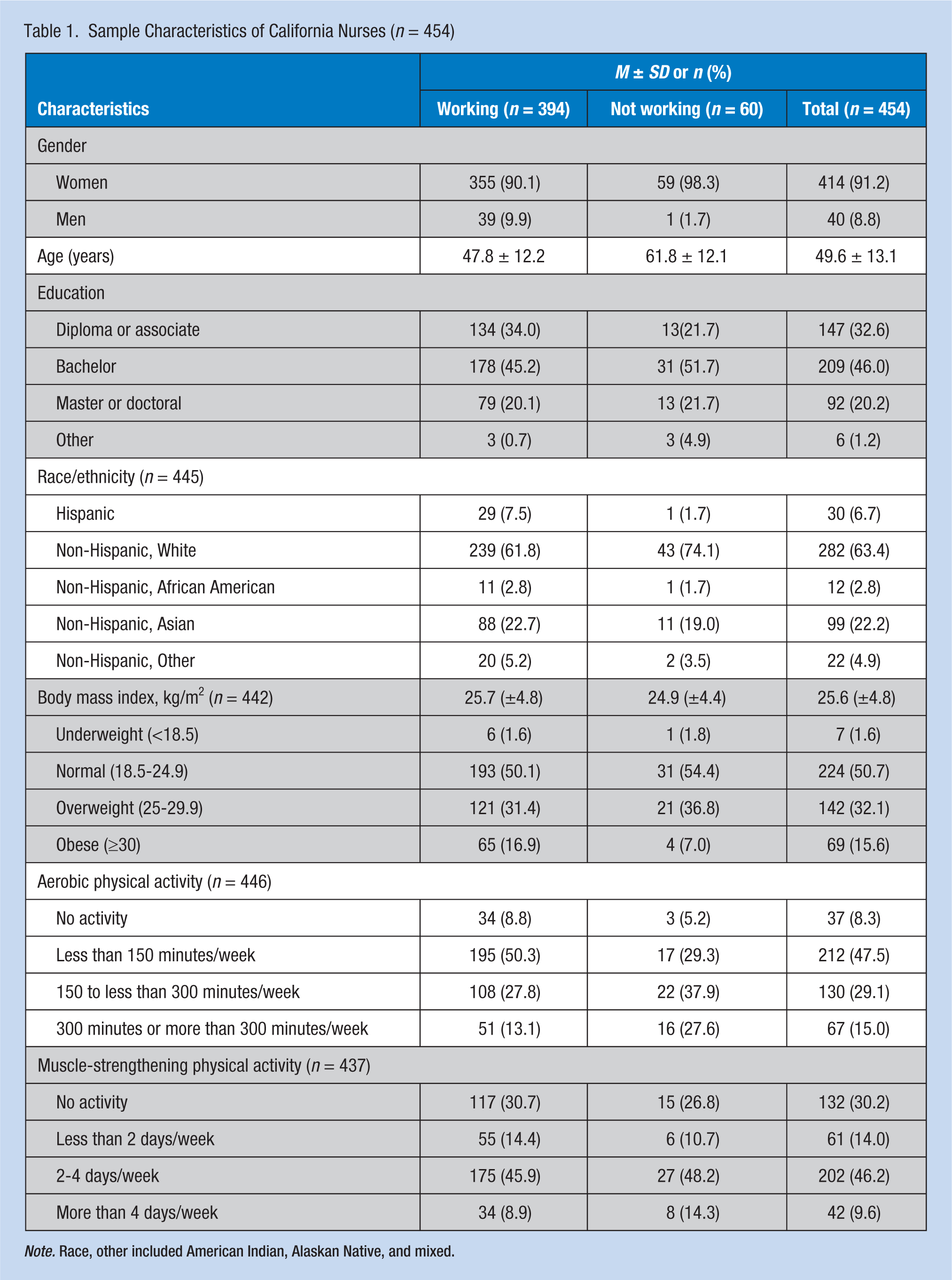
Note. Race, other included American Indian, Alaskan Native, and mixed.
Table 2 presents descriptions of musculoskeletal symptoms by body region. Among our participants, low back symptoms were most frequently reported (61.7%), followed by neck symptoms (48.5%), shoulder symptoms (41.9%), and wrist/hand symptoms (41.6%). The mean score of musculoskeletal symptom index was 3.2 (SD = 3.1) of 12: 37.7% (n = 171) had the symptom index score of 1 to 3, 20.7% (n = 94) scored 4 to 6; and 16.3% (n = 74) scored greater than 6.
Musculoskeletal Pain Symptoms in the Past 12 Months by Body Region Among California Nurses (n = 454)
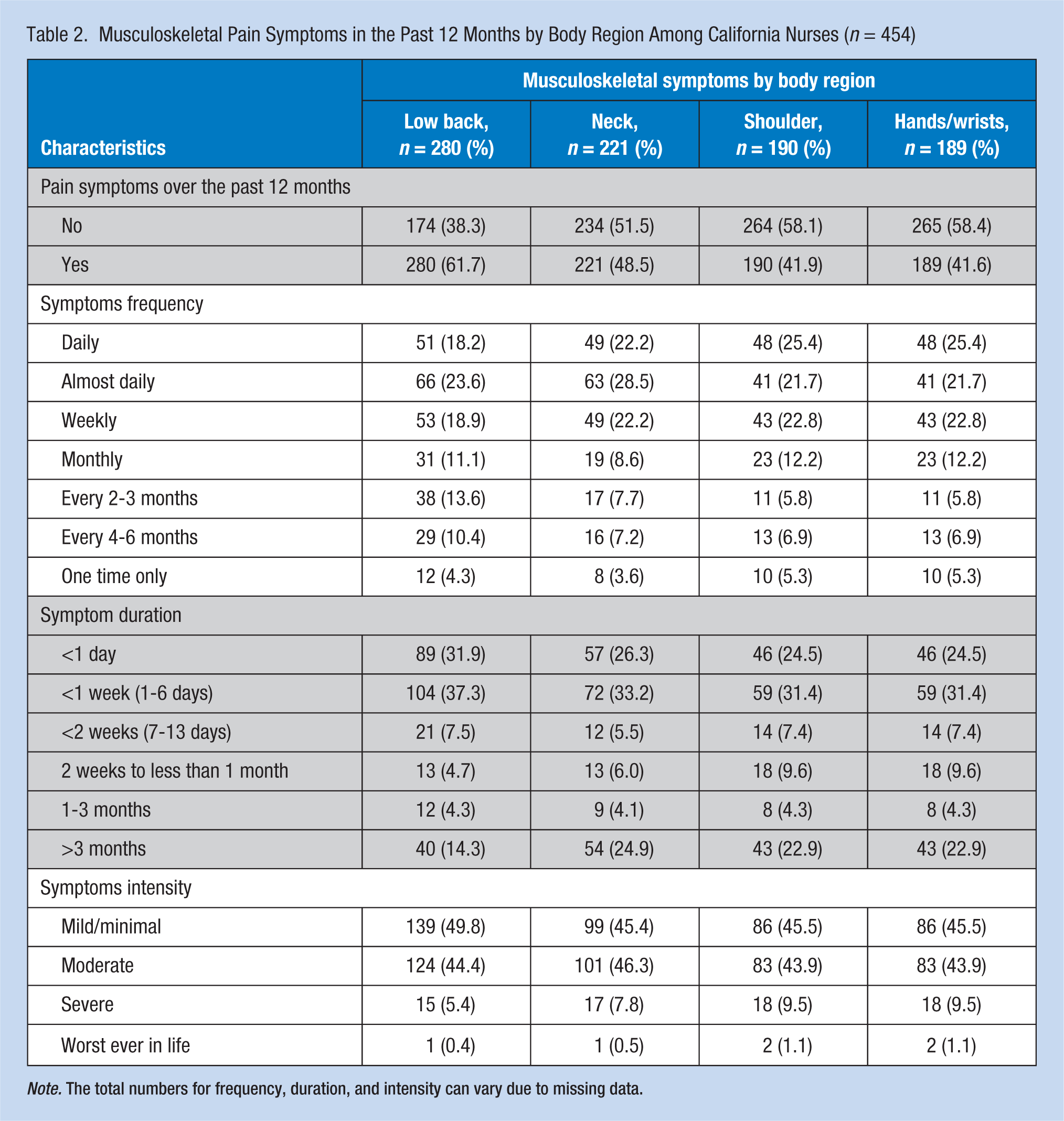
Note. The total numbers for frequency, duration, and intensity can vary due to missing data.
Regular Physical Activity by Sociodemographics, BMI, and Musculoskeletal Symptoms
Nurse characteristics of age (p < .01) and race (p = .03) were significantly associated with regular aerobic physical activity (Table 3). The prevalence of regular aerobic physical activity was the lowest among nurses 35 to 44 years of age (24.3%) and Asian nurses (30.9%). Currently working nurses were significantly less engaged in regular aerobic physical activity than nonworking nurses (41.0% vs. 65.5%; OR = 0.36; 95% CI = [0.20, 0.65]). Compared with nurses with normal BMI, nurses with BMI ≥30 were significantly less likely to engage in regular aerobic physical activities (46.8% vs. 24.6%; OR = 0.36; 95% CI = [0.20, 0.67]) and muscle strengthening (62.7% vs. 40.3%; OR = 0.42; 95% CI = [0.24, 0.73]). For musculoskeletal symptoms, nurses with a symptom index ranging from 1 to 3 were significantly less likely to engage in regular aerobic physical activity than nurses without any symptoms (39.2% vs. 51.8%; OR = 0.60; 95% CI = [0.37, 0.97]). Nurses with a symptom index ranging from 4 to 12 also showed lower prevalence rates, but the findings were not significant. Nurses with a symptom index ranging from 1 to 3 also showed the lowest prevalence of muscle-strengthening activity (49.1%); the finding was marginally significant (OR = 0.63; 95% CI = [0.38, 1.03]).
Prevalence (%) and Bivariate Analyses of Aerobic PA and Muscle-Strengthening PA Among California Nurses (n = 454)
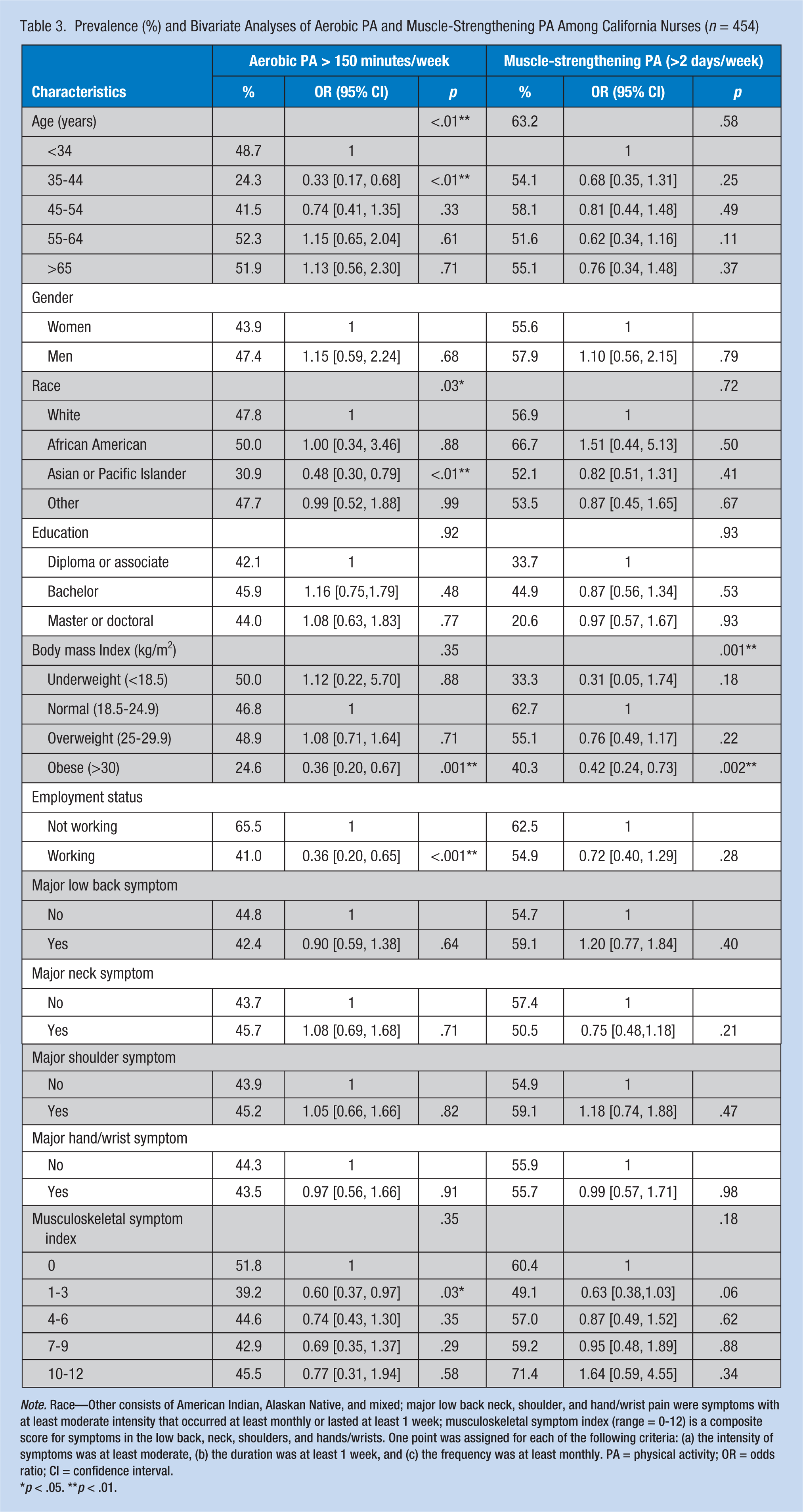
Note. Race—Other consists of American Indian, Alaskan Native, and mixed; major low back neck, shoulder, and hand/wrist pain were symptoms with at least moderate intensity that occurred at least monthly or lasted at least 1 week; musculoskeletal symptom index (range = 0-12) is a composite score for symptoms in the low back, neck, shoulders, and hands/wrists. One point was assigned for each of the following criteria: (a) the intensity of symptoms was at least moderate, (b) the duration was at least 1 week, and (c) the frequency was at least monthly. PA = physical activity; OR = odds ratio; CI = confidence interval.
p < .05. **p < .01.
Factors Associated With Regular Physical Activity: Multivariable Analysis
Multivariable analyses indicated that non-White nurses (OR = 0.61; 95% CI = [0.40, 0.94]), working nurses (OR = 0.48; 95% CI = [0.25, 0.91]), and nurses with higher BMI (OR = 0.93; 95% CI = [0.89, 0.97]) were significantly less likely to engage in regular aerobic physical activity (Table 4). Nurses with higher BMI (OR = 0.92; 95% CI = [0.88, 0.96]) were also significantly less likely to engage in regular muscle-strengthening physical activity. The musculoskeletal symptom index was not significant in the multivariable model.
Multivariable Logistic Regression Models of Aerobic PA and Muscle-Strengthening PA Among California Nurses (n = 454)
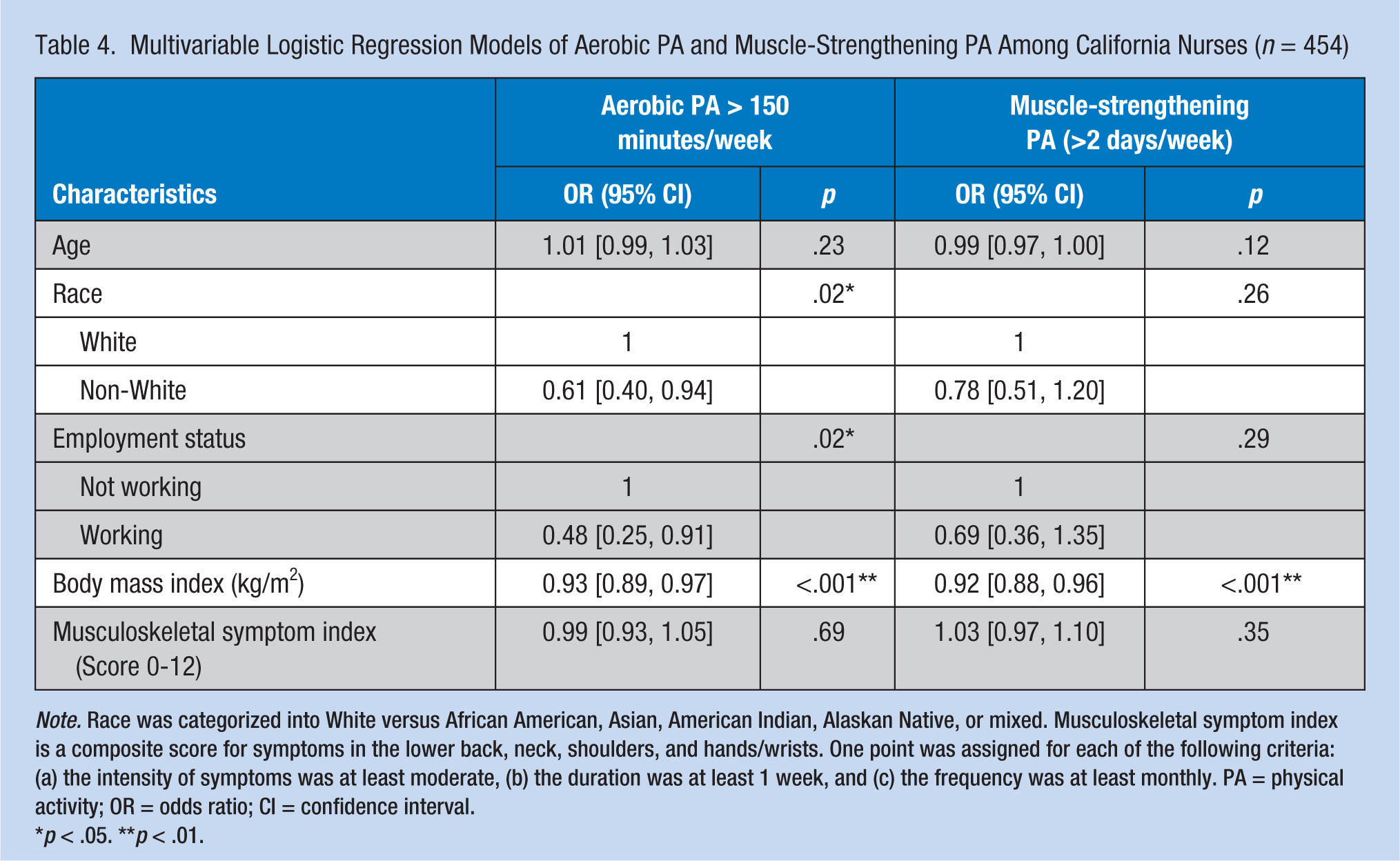
Note. Race was categorized into White versus African American, Asian, American Indian, Alaskan Native, or mixed. Musculoskeletal symptom index is a composite score for symptoms in the lower back, neck, shoulders, and hands/wrists. One point was assigned for each of the following criteria: (a) the intensity of symptoms was at least moderate, (b) the duration was at least 1 week, and (c) the frequency was at least monthly. PA = physical activity; OR = odds ratio; CI = confidence interval.
p < .05. **p < .01.
Discussion
Nurses are at high risk of musculoskeletal injuries from work; however, the relationship between musculoskeletal symptoms and regular LTPA among nurses has been surprisingly understudied. The majority of working nurses in our sample reported having symptoms in the low back, neck, shoulders, or hands/wrists daily or almost daily, and their regular LTPA levels were far from optimal: a rate of 44% and 56% for aerobic and muscle-strengthening physical activities, respectively. However, different from our hypothesis, musculoskeletal symptoms were not a significant risk factor for LTPA after controlling for other correlates, yet we found significant associations with employment status, race, and BMI.
Although musculoskeletal symptoms were not significant in our multivariable model, in bivariate analysis we found a significantly lower level of regular LTPA among nurses with low musculoskeletal symptom index scores (1-3) than among nurses without any symptoms. Interestingly, nurses with higher symptom index scores tended to show slightly higher LTPA rates than nurses with low symptom index scores. This finding suggests that having musculoskeletal symptoms negatively affects LTPA, but experiencing more or greater symptoms may affect their motivation to perform LTPA to manage their symptoms or prevent further injuries. In fact, some studies have shown that regular LTPA could prevent occupation-related musculoskeletal injury (Feng et al., 2014; Hildebrandt, Bongers, Dul, van Dijk, & Kemper, 2000). For example, in a prospective study of 2,265 workers in the Royal Norwegian Navy, engaging in regular LTPA was significantly associated with fewer musculoskeletal symptoms (Morken, Mageroy, & Moen, 2007). As such, the relationship between LTPA and musculoskeletal symptoms is likely to be bidirectional, and this mixed bidirectional effect may have been present in our study findings. Future research with prospective study and large samples is needed to elucidate the impact of musculoskeletal symptoms on LTPA.
The novel finding in this study is that employment status, race, and BMI were significant factors for engaging in regular aerobic physical activity among nurses. Among these factors, only BMI was significantly associated with regular muscle-strengthening physical activity. Studies on physical activity showed that employed women were less likely to engage in LTPA, particularly among racial/ethnic minority groups (Eaton et al., 1993; S. H. Lee & Im, 2010; Sternfeld, Cauley, Harlow, Liu, & Lee, 2000), and our study of nurses also showed there to be consistent findings. Also, consistent with other studies of the general population (Taylor, Kimbro, Evans-Hudnall, Haughton McNeill, & Barnes, 2015; Whitt-Glover et al., 2009), minority nurses such as Asian nurses showed significantly lower levels of LTPA than White nurses. Previous studies showed that racial-specific correlates of LTPA among minority women were often health beliefs, social support, and time constraints due to family responsibilities (Cassetta, Boden-Albala, Sciacca, & Giardina, 2007; Sweet et al., 2009; Trost, Owen, Bauman, Sallis, & Brown, 2002). Along the same lines, we found that working nurses and middle-aged groups (34-54 years) who may have many competing jobs and family responsibilities were less likely to engage in LTPA.
Last, consistent with most studies of the general population (Donnelly et al., 2009), nurses with higher BMI in our study engaged in less LTPA, both aerobic and muscle-strengthening physical activities. Although most working nurses perform work-related physical activities, the biological effects of different types of physical activities (i.e., LTPA vs. occupational physical activity) on obesity and health might be different (Gutiérrez-Fisac et al., 2002; Koenig, Sund, Döring, & Ernst, 1997). Studies have shown that energy expenditures from occupational physical activity were not associated with lower BMI, waist/hip ratio, body fat composition, or cardiovascular disease risk (Gutiérrez-Fisac et al., 2002; Koenig et al., 1997). Moreover, a job requiring a demanding level of physical tasks can have a negative influence on mental health such as depression, stress, and anxiety, and in turn, negatively influences LTPA engagement (Feng et al., 2014; Fransson et al., 2012; Han et al., 2014; Lallukka, Lahelma, et al., 2008; Lallukka, Sarlio-Lahteenkorva, et al., 2008). Also, the energy expenditure derived from occupational physical activity could be neutralized by higher dietary intake in individuals who are more active at work (Gutiérrez-Fisac et al., 2002; Paeratakul, Popkin, Keyou, Adair, & Stevens, 1998). In fact, individuals with greater occupational physical activity reported higher caloric intake than those whose occupation required less physical activity (Paeratakul et al., 1998). Although our study cannot provide a definitive explanation— without controlling for the effect of diet and a level of occupational physical activity—the findings of the high obesity rate and low LTPA rate may be partially explained by our sample whose jobs often require physically demanding work. More research is needed to understand LTPA and occupational physical activity along with other lifestyle risk factors such as unhealthy eating or disrupted sleep cycles.
Limitations of this study include the use of self-report measures, which are subject to recall or reporting bias in physical activity levels, BMI, and musculoskeletal symptoms. Our study may have underestimated the prevalence of obesity and overestimated the prevalence of LTPA. The nature of this cross-sectional study made it impossible to infer causality. In addition, nurses were recruited from one geographical area where the obesity rate was relatively low than in other states (CDC, 2017); this may limit the generalizability of our study findings. All participants had an active California nursing license to be included in the study, but a small number of nurses belonged to the nonworking group and about half of them were retirees. As such, with a heterogeneous sample, we did not include occupational physical activity in this study, which may affect LTPA engagement. In addition, we included only musculoskeletal symptoms in the upper body, commonly reported among nurses, and thus our findings are limited to explain the relationship between LTPA and overall musculoskeletal symptoms. To better understand the relationships, future research needs to further examine both occupational and leisure-time physical activities in relation to musculoskeletal symptoms. Last, potential confounders such as income, neighborhood environment, sleep patterns, social support, and health beliefs may be associated with LTPA levels among nurses but were not evaluated in our study. This might have influenced our findings on nurses’ LTPA.
Implications for Occupational Health Nurse Practice
Workplace health-promotion or wellness programs have evolved to promote workers’ health and well-being, and physical activity is one of the main components in wellness programs. Our study findings suggest that nurses also need education and better support in the workplace for personal health behavior change for their own health as well as for their patients. As shown in other worker populations, worksite physical activity interventions would be beneficial for nurses to improve their physical and mental health, and job productivity (Anderson et al., 2009; Flannery, Resnick, & McMullen, 2012; Kobayashi, Kaneyoshi, Yokota, & Kawakami, 2008; Nam & Whittemore, 2014).
In particular, nurses are in a key position to promote regular physical activity and to endorse prevention of obesity. In a review of healthcare providers’ LTPA habits and their health-promotion practices, higher LTPA levels among physicians and nurses were associated with higher physical-activity-promoting practices for their patients (Abramson, Stein, Schaufele, Frates, & Rogan, 2000; Fie, Norman, & While, 2013). A majority of patients reported that they received physical activity consultations more from nurses than from physicians (Fie et al., 2013; Puig Ribera, McKenna, & Riddoch, 2005). In another study, nurses reported positive views about health promotion in general, but the study patients recalled very low levels of lifestyle counseling advice delivered by nurses, including physical activity promotion (Duaso & Cheung, 2002).
Occupational health nurses play a central role in designing and providing workplace wellness programs. In designing the program, occupational health nurses should be aware that health disparities exist among healthcare workers (Chou & Johnson, 2008; Mawn et al., 2010; Nam & Whittemore, 2014). Particularly, Black, Hispanic, and Asian healthcare workers are less likely to report their general health status as excellent than White healthcare workers, and tend to report more job-related injuries, burnouts, and physical inactivity (Caban-Martinez et al., 2007; Chou & Johnson, 2008; Luckhaupt, Cohen, Li, & Calvert, 2014). Special efforts to reduce health disparities should be made in providing workplace wellness programs.
Conclusion
In summary, our study sample of registered nurses— who are well poised to promote physical activity— reported low engagement in LTPA, and the majority did not meet the recommended level of aerobic physical activity. In particular, currently working and Asian nurses were less likely to engage in regular aerobic physical activity. Nurses with higher BMI engaged less in regular aerobic and muscle-strengthening physical activity. Future research to understand the relationship of LTPA with musculoskeletal symptoms and job-related factors including occupational physical activity is needed. It is also important to identify barriers and facilitators to physical activity among nurses, and improve health disparities within the healthcare workforce by developing appropriate health interventions. Promoting the health of healthcare workers should be an important priority to deliver quality healthcare and improve the overall health status of the nation.
Applying Research to Practice
Nurses are in a key position to promote regular physical activity and to endorse prevention of obesity. However, nurses, the largest health care occupation group, have a high obesity rate and low leisure-time physical activity (LTPA). Frequent or severe musculoskeletal symptoms can interfere with individual's LTPA by experiencing limitation or discomfort related to physical activity. Nurses have a high prevalence of musculoskeletal symptoms from physically demanding tasks. There is a dearth of research examining factors affecting nurses' LTPA levels including both aerobic and muscle strengthening physical activity. Understanding the relationship between musculoskeletal symptoms and LTPA among nurses and potential correlates with their LTPA would help guide future workplace wellness programs to improve health among nurses and workplace productivity.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Southern California National Institute for Occupational Safety and Health (NIOSH) Education and Research Center Pilot Project Research Training Grant (Grant No. 2 T42 OH008412-08) and the National Institute of Nursing Research (K23NR014661).
Author Biographies
Soohyun Nam is an associate professor in the School of Nursing at Yale University, Orange, Connecticut.
MinKyoung Song is an assistant professor in the School of Nursing at Oregon Health & Science University, Portland, Oregon.
Soo-Jeong Lee is an associate professor in the School of Nursing at University of California, San Francisco (UCSF).