
Abstract
Approximately 8 million health care workers are unnecessarily exposed to highly toxic drugs used to treat cancer; antineoplastic drugs can contribute to negative health effects for these workers. The drugs have been detected in the urine of workers and on the floors and counters of worksites. Safety precautions that could reduce the risk of exposure are underutilized. This cross-sectional study of 163 oncology health care workers used a survey to measure workplace and individual factors, and environmental sampling to measure surface contamination. The study objective was to identify potential exposures to antineoplastic drugs and factors influencing safety behavior. Personal protective equipment (PPE) use was lower than recommended; unit of employment was significantly associated with PPE use. Chemical residue from antineoplastic drugs was found, revealing potential exposures. Workplace safety must be a higher organizational priority. The contamination of common work areas where PPE use is not expected was of utmost concern.
Keywords
Antineoplastic drugs are critical to the treatment of more than 12.1 million individuals diagnosed with cancer worldwide each year (Centers for Disease Control and Prevention, 2015). These drugs can improve quality of life, decrease length of illness, and cure cancer (American Cancer Society, 2015). Increasingly, the drugs are also being used for other diseases such as rheumatoid arthritis, nephritis, multiple sclerosis, and lupus (Vioral & Kennihan, 2012). Use of these drugs has also expanded to more frequent administration in outpatient settings, homes, and veterinary clinics (Hall, Davies, Demers, Nicol, & Peters, 2013). A new forecast has predicted that as a result of the aging U.S. population, the number of cancer cases may double by 2050, resulting in an increase in the use of antineoplastic drugs (Edwards et al., 2002).
The toxicity and health risks associated with antineoplastic drugs are well understood (Boiano, Steege, & Sweeney, 2014; Polovich & Clark, 2012). The International Agency for Research on Cancer (IARC) has classified a number of antineoplastic drugs as carcinogenic to humans (Group 1), probably carcinogenic to humans (Group 2a), or possibly carcinogenic to humans (Group 2b; Turci, Sottani, Spagnoli, & Minoia, 2003). Health care workers are exposed on a repeated basis and often for many years. Even a small exposure to such toxic drugs can cause adverse outcomes to the more than 8 million health care workers potentially exposed (Connor et al., 2010; Vioral & Kennihan, 2012). Beginning in the 1970s, evidence has indicated that health care workers were at risk for harmful effects from occupational exposure to antineoplastic drugs (National Institute for Occupational Safety and Health [NIOSH], 2004). These effects include acute responses such as skin rashes, nausea, hair loss, abdominal pain, nasal sores, allergic reactions, skin or eye injury, and dizziness (Valanis, Vollmer, Labuhn, & Glass, 1993). Chronic effects linked with exposure include reproductive harm such as delayed time to conception (Fransman et al., 2007), spontaneous abortion (Lawson et al., 2012), genotoxic changes (McDiarmid, Oliver, Roth, Rogers, & Escalante, 2010; Rekhadevi et al., 2007; Villarini et al., 2011), and cancers (Skov et al., 1992). Secondary tumor risks for patients receiving these drugs have been confirmed by several studies, and patients are warned about these risks (Deniz, O’Mahony, Ross, & Purushotham, 2003; Josting et al., 2003; Sherins & DeVita, 1973; Spiers, Chikkappa, & Wilbur, 1983). For patients with cancer, the benefit of treatment outweighs the risk of a secondary malignancy in the future. However, for health care workers, the occupational risk is unacceptable.
Although the hazards associated with antineoplastic drugs are recognized, no accepted safe level of exposure has been identified (Turci et al., 2003). Federal guidelines for safe handling of hazardous drugs were first published in 1986 and updated in 2004 by NIOSH. In addition, guidelines for the safe handling of hazardous drugs were also published by the Oncology Nursing Society (Polovich, 2011) and the American Society of Health-System Pharmacists (Polovich & Clark, 2012). These guidelines are only recommendations; federal policies on safe handling practices for health care facilities are lacking. However, recently, state laws have been enacted to standardize hazardous drug safety practices beginning in Washington in 2011 (Smith, 2011), with California (California Legislature, 2013) and North Carolina following (Prevent Hazardous Drug Exposure, House Bill 644, 2014). This lack of consistency in state laws may lead to differences in health care workers’ knowledge of and commitment to safe handling practices in a variety of sites (Boiano et al., 2014; Environmental Working Group, 2007).
Studies have shown more workers are wearing gloves when handling antineoplastic drugs since the first safe handling guidelines were published in 1986 (Martin & Larson, 2003; Polovich & Clark, 2012; Polovich & Martin, 2011). However, a recent large study of health care workers conducted by NIOSH found that nearly one in seven of 2,069 respondents reported not always using gloves while handling antineoplastic agents (Boiano et al., 2014). These studies also found lower than recommended use of chemotherapy gowns and double gloving (Boiano et al., 2014; Martin & Larson, 2003; Polovich & Martin, 2011). A study of 165 nurses published by Polovich also found personal protective equipment (PPE) use varied by activity, with the lowest adherence to recommendations about the handling of patient excreta (Polovich & Clark, 2012). Reasons for the lower than recommended uses of PPE are being considered by researchers (Friese, Himes-Ferris, Frasier, McCullagh, & Griggs, 2012; Polovich & Clark, 2012). Two recent articles reported that organizational factors such as positive safety culture as well as a smaller nurse to patient ratio can positively affect adoption of safe handling practices (Friese et al., 2012; Polovich & Clark, 2012) in contrast to the lack of evidence supporting an association between individual characteristics and safe handling practices (Polovich & Clark, 2012). A study published in the Journal of Patient Safety also found a link between employee safety climate and patient safety culture in health care, meaning improving one will inadvertently improve the other (Mohr, Eaton, McPhaul, & Hodgson, 2015). Scant intervention research has supported strategies that might translate into improved worker safety. To date, only one study has reported the results of an intervention to impact safer work practices by oncology nurses; Hennessy and Dynan (2014) reported findings from a program implemented at the Dana–Farber Cancer Institute, which improved compliance with PPE over time (Hennessy & Dynan, 2014). The program incorporated monitoring and reporting compliance regarding PPE use and also engaged the staff in audit activities. Further research is needed to develop and test interventions that will minimize unnecessary worker exposure to hazardous drugs.
Objectives
The objectives of this study were to determine key factors influencing exposure to antineoplastic agents for nursing and pharmacy staff working in oncology and whether their work surfaces were contaminated with these agents. The central hypothesis, based on previous research, is that reported PPE use will be relatively high for gloves, and low for double gloving, donning gowns, and using a face shield or mask (Boiano et al., 2014; Polovich & Clark, 2012). A second hypothesis predicted that, consistent with other studies, organizational factors such as workplace safety climate will better predict PPE use than individual factors (Friese et al., 2012; Polovich & Clark, 2012). The researchers also hypothesized that surface contamination with antineoplastic drugs would be present at about 50% of locations based on the results of a previous study conducted in university hospitals, which found that 60% of antineoplastic drug-wipe samples were contaminated above the level of detection (Connor et al., 2010).
Method
This study adapted a model developed by Polovich and Clark (2012) that outlines factors associated with safe handling techniques for antineoplastic drug administration by nurses and pharmacy staff potentially exposed to antineoplastic drugs at a university hospital and outpatient clinic. Data were collected online from a self-report staff survey and stored securely using the Research Electronic Data Capture (REDCap) Data System (Harris, Thielke, Payne, Gonzalez, & Conde, 2009) which is hosted by the University of Minnesota. An exposure assessment used area surface sampling to measure environmental contamination from chemotherapy drugs.
The population invited to participate in the survey was nurses, pharmacists, and pharmacy technicians (N = 163) from a university hospital’s inpatient oncology and bone marrow transplant (BMT) units and outpatient chemotherapy infusion center (four units). The survey was offered online to staff for 3 weeks in October 2014. Those who completed the survey were entered into a drawing for a US$50 Visa gift card (e.g., one winner for each unit). Surface samples were collected in the areas in which the surveyed staff worked a day prior to the survey release. The University of Minnesota Institutional Review Board (IRB) approved this study with exempt status. Approval was also granted by the hospital’s Nursing Research Council.
Environmental Assessment
Prior to collection of survey data, wipe samples for surface detection of chemotherapeutic agents were collected in patient care, nursing, and pharmacy areas. Sampling locations were associated with each job task known to have potential chemotherapy exposure: drug preparation, drug administration, drug and equipment disposal, and patient excreta handling. The sampling plan was reviewed by an experienced industrial hygienist who provided guidance on the planning and implementation of the exposure assessment and wipe sampling. Areas on each unit were tested based on work flow and locations at which selected drugs were most commonly used. For example, the nursing desk in the inpatient oncology unit was tested based on charge nurse feedback that workers set their chemotherapy bags on the desk while double-checking for the right drug, right patient, right dose, right route, and right time. Selection of the antineoplastic agents to be tested was based on those agents with the highest volume of use, consistent with the approach used in similar studies (Connor et al., 2010).
A total of 27 locations were tested, accounting for 65 unique antineoplastic agents by location combinations. The area of test sites was 200 cm2 for this study based on recommendations from an exposure assessment consultant. Previous studies have used a 100 cm2 area, which produced varied results. ChemoAlert™ (Bureau Veritas Laboratories, 2013), a custom kit designed to collect chemotherapy drug residues in health care workspaces to assess contact exposure, was used for testing. This method was developed in response to the NIOSH Drug Alert and a housekeeping standard recommendation, U.S. Pharmacopeial Convention (USP) 797 (Bureau Veritas Laboratories, 2013). Areas to be sampled were chosen with input from employees and management. The number of swab strokes was standardized for each sampling area. Two swabs were used for each area and placed in the same vial per laboratory recommendation. The laboratory provided a sample blank (solvent wetted and placed in a vial) that was not used to sample a surface to assure accurate testing.
Survey
The survey collected personal factors (i.e., age, race, and years of experience) and predictor variables (i.e., knowledge, perceived risk, self-efficacy, conflict of interest, perceived barriers, workplace safety climate, and interpersonal influence) to determine whether these factors predicted safe handling of chemotherapeutic drugs by staff. Survey items were taken from instruments with established reliability and validity and used in a previous study (Polovich & Clark, 2012).
Dependent or outcome variable
Use of Safe Handling Techniques was measured on a 5-point scale with questions adapted from the Revised Hazardous Drug Handling Questionnaire (Polovich & Clark, 2012), which was based on the current guidelines for safe handling (NIOSH, 2004). The availability and use of PPE were measured during four categories of potential exposure: preparation, administration, disposal, and patient excreta handling. Personal protective equipment questions were scored from 5 (always use) to 0 (never use). Higher scores showed more common use of PPE. A PPE use score was calculated for respondents based on their responses to the use of gloves, double gloves, gowns, and whether or not they reused disposable gowns and eye and respiratory protection.
Independent variables
Predictor variables and their attributes are listed in Table 1. These measures were adapted from Geer et al. (2007), Gershon et al. (1995), and Gershon et al. (2007), and included perceived risk, self-efficacy, conflict of interest, perceived barriers, workplace safety climate, and interpersonal influence. Knowledge of the hazard was measured using an adaptation of the NIOSH Survey of Safe Handling for Workers and the Chemotherapy Exposure Knowledge Scale (Polovich & Clark, 2012).
Predictor Variables
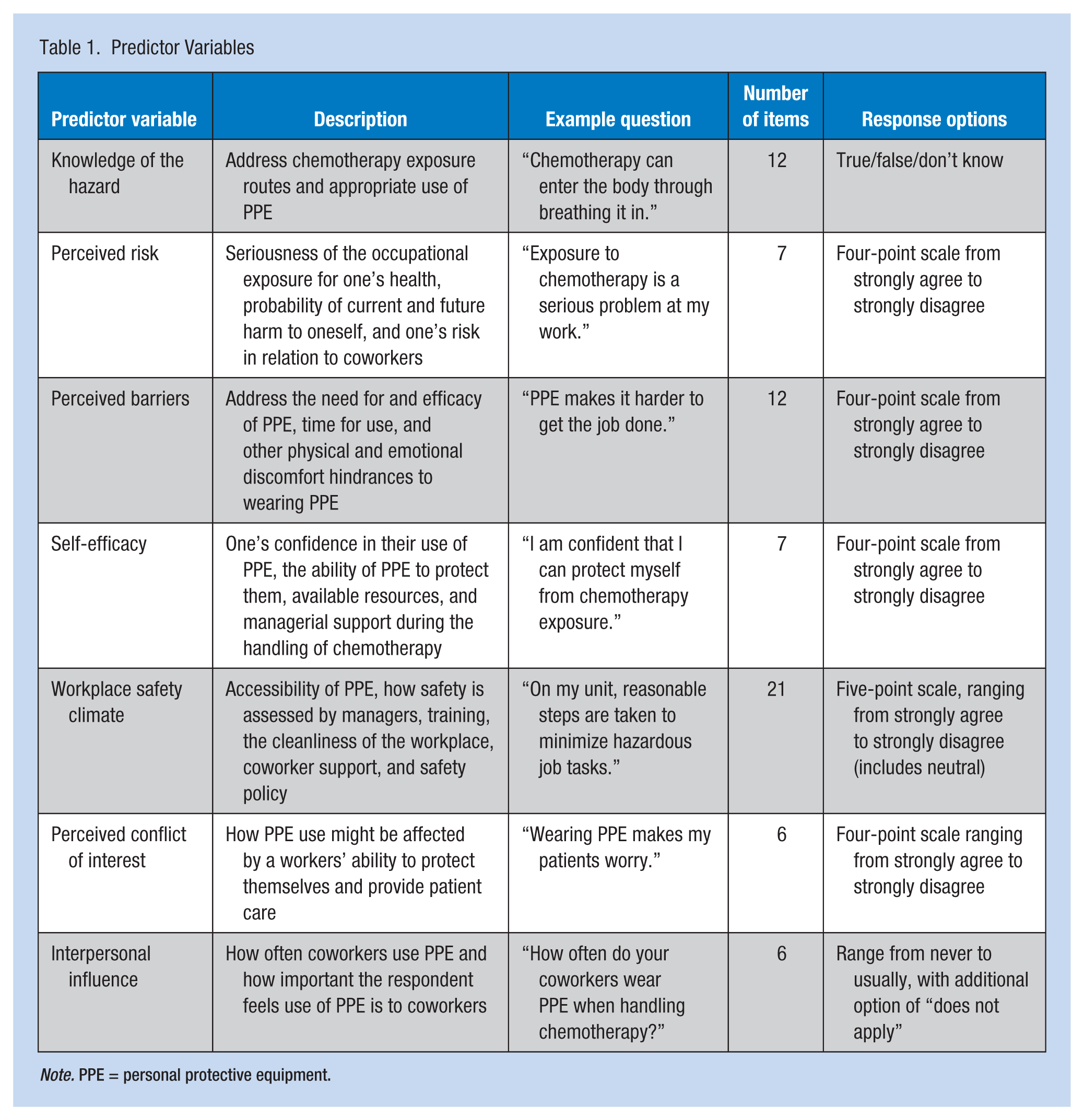
Note. PPE = personal protective equipment.
Pregnancy and alternative duty
Respondents were also asked whether or not they had been pregnant during their current job, and if so, whether they sought alternative duty because of their pregnancies. If they had not been pregnant, the survey asked whether they thought they would seek alternative duty if they became pregnant. These questions were pilot tested with nurse managers.
Data Analysis
Bureau Veritas Laboratories analyzed the wipe samples for each antineoplastic agent’s unique level of detection. Because no safe level of antineoplastic agents has been established, any result over the level of detection was considered “contaminated” (Turci et al., 2003).
Descriptive analysis of the survey variables included calculation of frequency distributions, means, and standard deviations. Univariate regression was used to assess the strength of the relationship between PPE use and age, years of oncology experience, unit, knowledge, perceived barriers, perceived risk, workplace safety climate, self-efficacy, interpersonal influence, and conflict of interest. The regression model for multivariable estimation was based on the use of directed acyclic graphs (DAGs; Greenland, Pearl, & Robins, 1999). The purpose of using DAGs in observational and cross-sectional studies is to ensure the regression models address the aims of the study by incorporating causal assumptions and avoiding confounded models. Directed acyclic graphs visually display the underlying assumptions of the casual relationships between the exposure of interest, covariates, and outcome of interest. The graphs facilitated the selection of potential confounders when testing the casual association between specific exposures and the outcome, use of safe handling techniques. The data analysis was generated using SAS software, Version 9.3, SAS System for PC (SAS Institute, Inc., 2010).
Results
Environmental Assessment
Overall, five samples, from a total of 62, tested above the limit of detection (8%). The unit with the highest number of areas that tested positive was the outpatient chemotherapy infusion center with three specific areas that were contaminated with chemotherapy. The inpatient BMT and inpatient oncology units each had one area with high levels of contamination. One of the pharmacy areas had no positive samples, and the other pharmacy area had one positive sample, which was a countertop shared between pharmacy and the outpatient chemotherapy infusion center. Table 2 shows results for the areas sampled.
Surface Contamination Results
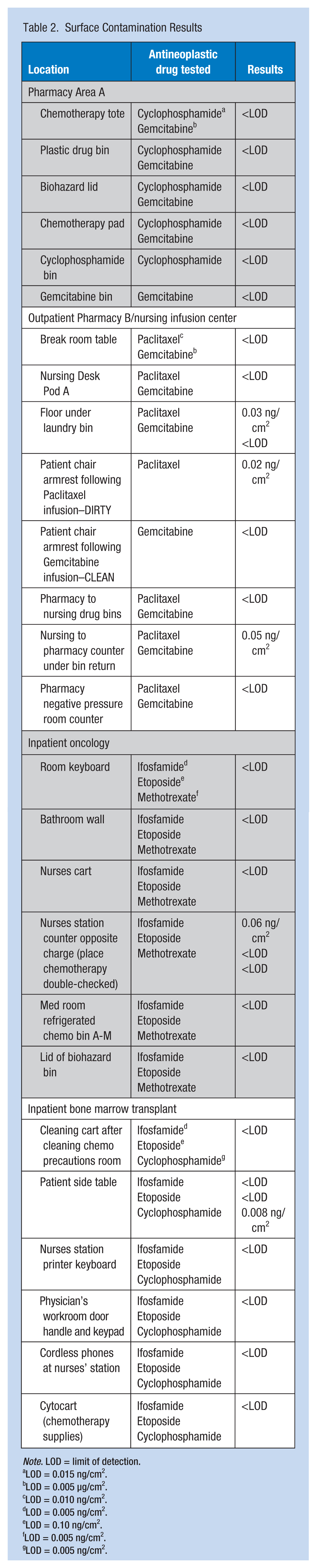
Note. LOD = limit of detection.
LOD = 0.015 ng/cm2.
LOD = 0.005 µg/cm2.
LOD = 0.010 ng/cm2.
LOD = 0.005 ng/cm2.
LOD = 0.10 ng/cm2.
LOD = 0.005 ng/cm2.
LOD = 0.005 ng/cm2.
Survey
Overall, the survey response rate was 62% of 163 employees, with each unit’s response rate at least 57%. Eleven of 19 pharmacy staff and 89 of 144 nurses responded to the questionnaire. The average age of survey respondents was 38 years, and the sample was 85% White. Nurse respondents reported an average of 12 years of nursing experience and an average of 10.5 years of oncology nursing experience. Forty-one percent of the nurse participants were oncology nursing certified. Demographic results are outlined in Table 3.
Demographics of Survey Respondents
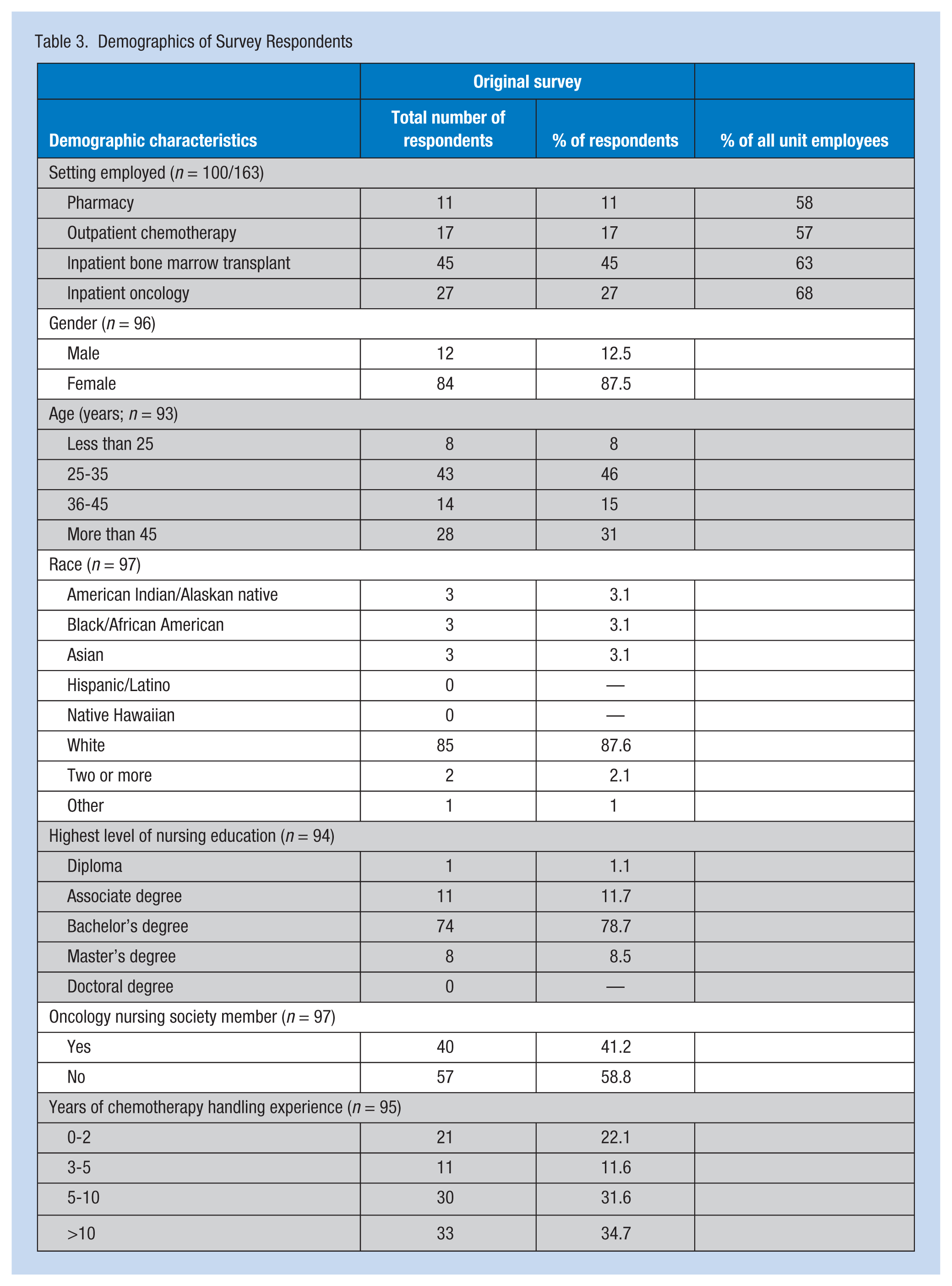
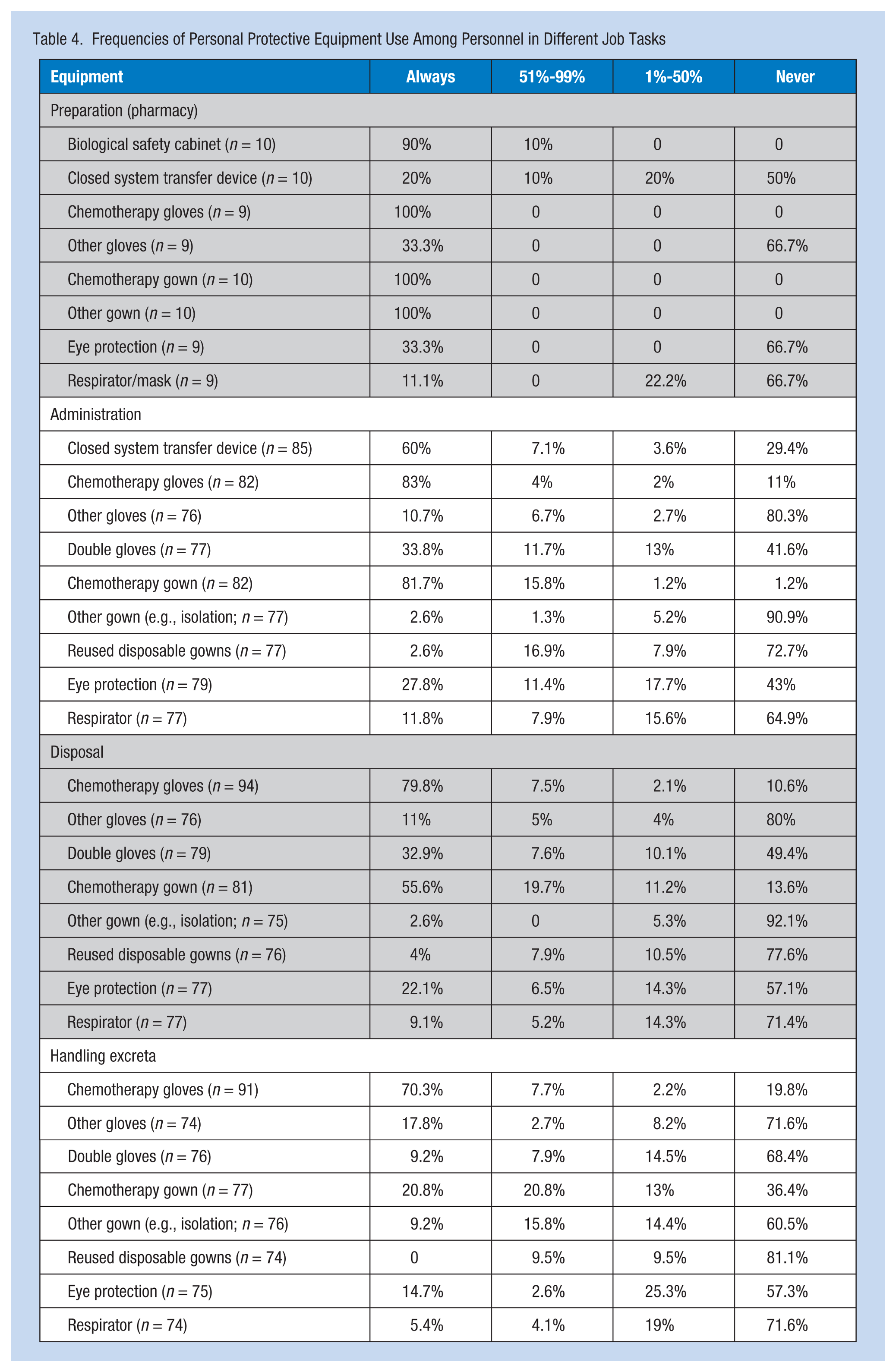
Study participants were similar to respondents who answered the nonparticipant survey with respect to average age (38 vs. 36 years), years of oncology experience (10.5 vs. 12.5 years), and reported PPE use (combined measure score of 40 vs. 40.3). Reported PPE use is outlined in Table 4. Overall, glove use was high; use of gowns and double gloving were lower, and use of respirator or eye protection scored lowest of these work practices.
Frequencies of Personal Protective Equipment Use Among Personnel in Different Job Tasks
Univariate regression was used to assess the strength of the relationship between PPE use and variables measuring constructs in the theoretical model, including personal factors (i.e., age, gender, and years of chemotherapy experience) and predictor variables (i.e., knowledge, perceived risk, self-efficacy, interpersonal influence, perceived barriers, workplace safety climate, and conflict of interest). Unit and patient load were also considered as these variables were strongly correlated with PPE use. Significant univariate associations were found for workplace safety climate, self-efficacy, perceived risk, perceived barriers, knowledge, conflict of interest, patients per day, and selected workplace units. The outpatient infusion center and the inpatient oncology unit in the hospital had lower PPE use scores, whereas the pharmacy had higher scores compared with the inpatient BMT group.
Multivariate regression models were estimated to determine the association of unit, self-efficacy, workplace safety climate, and perceived barriers to PPE use. Potential confounding variables were identified with the aid of DAGs. The findings revealed that unit was significantly associated with use of PPE. Self-efficacy was also associated with PPE use after controlling for appropriate confounders. Two models of workplace safety climate were estimated, which varied only by the inclusion or exclusion of the unit variable. The findings revealed the model which did not include the unit was statistically significant. Results of regression models are shown in Table 5.
Results of Univariate and Multivariate Regressions: Factors Influencing Personal Protective Equipment Use
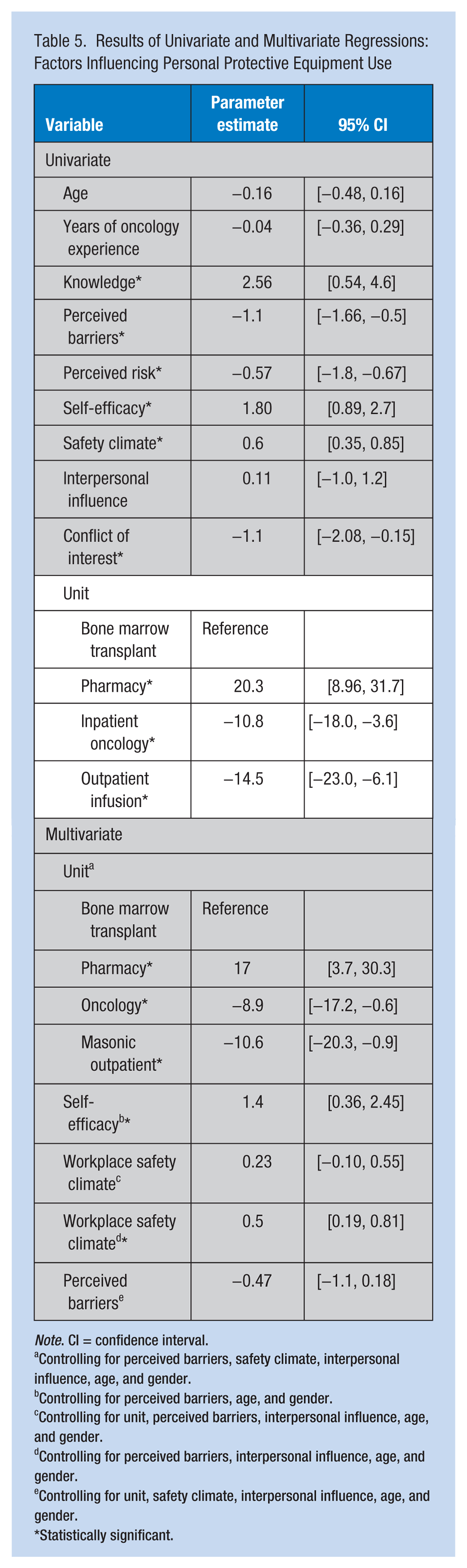
Note. CI = confidence interval.
Controlling for perceived barriers, safety climate, interpersonal influence, age, and gender.
Controlling for perceived barriers, age, and gender.
Controlling for unit, perceived barriers, interpersonal influence, age, and gender.
Controlling for perceived barriers, interpersonal influence, age, and gender.
Controlling for unit, safety climate, interpersonal influence, age, and gender.
Statistically significant.
Pregnancy and Alternative Duty
Twenty-eight percent of respondents reported having been pregnant while working their current job, and four of these respondents reported having sought alternative duty. Of the 72% who have not been pregnant while employed at their current job, 33% reported that they would seek alternative duty if they became pregnant and 26% reported being unsure whether they would seek alternative duty or not. Institutional policy is that alternative duty will be provided if requested.
Discussion
Study findings revealed that the organizational unit where a nurse or pharmacist worked was most strongly associated with use of PPE when adjusting for other factors such as perceived barriers, safety climate, interpersonal influence, gender, and age. Analyses demonstrated that safety climate and perceived barriers were not associated with PPE use when holding organizational unit constant. Organizational unit is likely a proxy measure for many factors potentially influencing workplace safety, including variables not included in this study (e.g., staffing ratios). Study results showed that workplace safety climate was associated with PPE use, and the association was graded for each organizational unit; as workplace safety climate score increased, PPE use also increased and perceived barriers decreased. The association between safety climate and PPE use is consistent with a previous study by Polovich and Clark (2012) and studies of workplace safety climate in diverse industries including health care (Christian, Bradley, Wallace, & Burke, 2009; Friese et al., 2012; Polovich & Clark, 2012; Zohar, 2010).
Use of PPE, a proxy for safe handling techniques, was highest for pharmacy staff and nurses who worked on the BMT floor. The nurses who worked on the BMT floor also reported caring for the lowest number of patients during a shift, and the pharmacy environment did not involve direct patient care. The unit with the highest number of contaminated areas was the outpatient chemotherapy infusion center with three areas that tested positive for chemotherapy residue including a counter between the outpatient nursing area and the pharmacy area where antineoplastic agents were received by nurses, the floor under a laundry bin, and an armrest of a patient chair following Paclitaxel infusion. The inpatient BMT and inpatient oncology units each had one area with surface contamination. In the BMT unit, it was a patient’s bedside table that showed detectable levels of chemotherapy residue. In the inpatient oncology unit, the area of contamination was at the nurses’ station desk where chemotherapy is double-checked for patient safety with the computer chart prior to infusion in a patient room. It was this latter finding that was of most concern among all the surface wipe samples as it had the highest level of contamination, and it was a space frequently used by multiple health care staff without benefit of PPE. In addition, drink containers have been placed on and near this area, raising questions about potential exposure through dermal absorption and possibly ingestion.
The differences found in PPE use and surface levels of chemotherapy residue between the pharmacy and nursing work environments were unexpected and curious. It may be partially due to different job tasks performed by each discipline. Nurses performed multiple job tasks involving chemotherapy which required the use of PPE, including drug administration and disposal as well as handling patient excreta. Such tasks typically involve many interruptions. In contrast, the pharmacists’ contact with chemotherapy primarily involved drug preparation, a specific job task, which is done without patient and family member interruption. Because this is one of the only studies the authors found that surveyed both nursing and pharmacy staff, additional research is needed to see whether these differences are found in other oncology settings.
Survey results regarding reported PPE use were similar to other published studies where glove use was high and double gloving was much lower (Boiano et al., 2014; Polovich & Clark, 2012). This finding is likely because double gloving takes extra time and may make tasks more cumbersome. The finding also confirms other studies that reported PPE use varied by task, with higher use of PPE among health care workers who are preparing and administering chemotherapy compared with workers disposing of chemotherapy or handling patient excreta. This finding is likely due to the nature of the activities; administration is often a planned event, whereas disposal and handling body fluids are more dynamic.
Predictor variable scores for this study were compared with findings from the study by Polovich and Clark (2012) who used a national sample of outpatient nurses. Results were similar between the studies. Overall, knowledge of exposure and self-efficacy scores were high. Conflict of interest and perceived barriers were low. Workplace safety climate scores were moderate, but lower than the mean of the Polovich and Clark.
The number of nurses who reported they would ask for alternative duty if they became pregnant was much higher than the number who had asked for alternative duty. It is unclear whether this finding is because priorities change once staff members become pregnant, whether a social desirability bias (i.e., the survey somehow suggested that they should ask for alternative duty) was present, or whether staff members who work on these units and enjoy their practices find it difficult to imagine asking for alternative duty and working elsewhere in the hospital or they worry about unanticipated consequences if they ask for accommodations.
Limitations and Recommendations
Several study limitations should be noted when interpreting this study. Although PPE use and predictor variable responses of nonrespondents are unknown, it may be hypothesized that nonrespondents would score lower on the workplace safety climate measure because they did not take time to complete the survey. Those individuals who responded to the short survey did report equal PPE use; however, this was a small group of only 10 workers. Because better workplace safety climate is correlated with higher PPE use, it might also mean that these nonresponders may have slightly lower use of PPE during safe handling. Although the majority of staff on each unit responded to the survey, the responses were from individuals working in only one institution; thus, the generalizability of the study findings to other settings is unknown. Ultimately, the study should be replicated at several institutions with oncology service units to assess generalizability of findings. In addition, an important factor associated with PPE use in some studies is nurse-to-patient ratio, which was not measured in this study but is important for future researchers to consider. Because the organizational unit is likely a proxy measure for many factors potentially influencing workplace safety, future research should identify the relative contributions of factors that vary by unit and may influence use of PPE (e.g., safety climate, self-efficacy, and staffing ratios).
Although environmental sampling was completed in 27 key locations accounting for 65 unique antineoplastic agents by location combinations based on expert, management and staff advice, and resources, ultimately the findings of surface contamination could vary day by day, based on the antineoplastic agents given, staff safety behaviors, cleaning techniques, and whether or not recent spills had occurred. Despite these limitations, this study combined findings on surface contamination, reported PPE use, and influencing variables such as workplace safety climate among both inpatient and outpatient oncology nursing and pharmacy staff. Future studies could benefit from a more comprehensive sampling approach and a design to better understand why surface areas are contaminated with chemotherapy so that health care workers and hospital visitors are protected. The contamination of common work areas where health care workers are not expected to use PPE is of utmost concern.
Implications for Practice
The organizational unit is a significant driver of PPE use during chemotherapy handling. These findings suggest focusing on organizational, rather than individual, factors when encouraging the use of PPE. Surface contamination is a risk to health care workers and others on these oncology units, and precautions should be taken to prevent unnecessary exposure to these dangerous agents. According to NIOSH (2004) recommendations, work surfaces should be cleaned with an appropriate deactivation agent before and after each activity and at the end of the work shift. Surface monitoring should be scheduled every 6 months to a year, or if concerns about worker health are noted (NIOSH, 2004). Although this study focused on nurses and pharmacy staff, other members of the health care team such as patient care assistants, cleaning staff, and delivery personnel also have the potential for exposures. Visitors to the hospital similarly may be at risk, and all of these populations should be addressed in future studies.
Applying Research to Practice
Health care facilities that prepare, administer, or care for patients receiving antineoplastic drugs should review their policies about safe handling and provide proper training to all members of the health care team.
These facilities should also conduct worksite analyses to better identify gaps in the safety behaviors of personnel.
Worksites should create a culture of both patient and worker safety.
Worksites should review and follow, at a minimum, the National Institute for Safety and Health’s 2004 Alert: Preventing Occupational Exposures to Antineoplastic and Other Hazardous Drugs in Health Care Settings (National Institute for Occupational Safety and Health, 2004).
Footnotes
Acknowledgements
The authors thank Susan Arnold, PhD, CIH, FAIHA, for her instrumental help with sampling development and implementation. They also thank the unit managers and staff members for their support and feedback.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided, in part, by the: National Institute for Occupational Safety and Health (NIOSH), Centers for Disease Control and Prevention, Department of Health and Human Services, and the Midwest Center for Occupational Health and Safety (NIOSH Training Grant T42 OH008434).
Author Biographies
Catherine Utecht Graeve, PhD, MPH, RN, has worked as an oncology nurse and is an associate nursing professor and hospice nurse. She is part of the Minnesota Hazardous Drug Work Group.
Patricia Marie McGovern, PhD, MPH, RN, is the Bond Professor of Environmental and Occupational Health Policy at the University of Minnesota, School of Public Health where she also directs the occupational and environmental health nursing program. Her research applies the methods of health services research to occupational and environmental health issues, in particular, exposures impacting women’s and children’s health.
Bruce Alexander, PhD, is an occupational and environmental epidemiologist with interests in respiratory disease, cancer, injuries, agricultural health, global health, and developing public health capacity. He received his doctoral degree in epidemiology from the University of Washington in 1994 and has been on the faculty of the University of Minnesota School of Public Health since 1998.
Timothy Church earned an MS and PhD in biostatistics from the University of Minnesota, where he is currently a tenured professor. He conducts research on occupational injury and risk, mass screening for cancer and other chronic diseases, identification and treatment of cardiac arrhythmia with implantable devices, and statistical and epidemiologic methods. His articles have appeared in Biometrics, the New England Journal of Medicine, the Journal of the American Medical Association, the Journal of the National Cancer Institute, Circulation, and Gastroenterology and have been cited over 16,000 times by other authors.
Andrew Ryan is a senior research fellow in the Division of Environmental Health Sciences at the University of Minnesota. He has 20 years of experience with database management and statistical programming and assists master’s and doctoral students in the Midwest Center with the study design and analysis components of their research projects. He has authored or co-authored more than 30 peer-reviewed publications since 2001.
Martha Polovich, PhD, RN, AOCN, an oncology nurse since 1980, is a nurse researcher in occupational hazardous drug exposure and an assistant professor at the Byrdine F. Lewis School of Nursing at Georgia State University in Atlanta. She is editor of several Oncology Nursing Society publications about chemotherapy. She speaks on chemotherapy safe handling nationally and internationally.