
Abstract
Occupational health nurses motivate employees to engage in healthy behaviors. Both clinicians and researchers need strong theories on which to base decisions for health programs (e.g., healthy diet) and experimental interventions (e.g., workplace walking). The self-determination theory could be useful as it includes concepts of individual autonomy, competence to perform healthy behaviors, and relationships as predictors of health behaviors and outcomes. In this article, the self-determination theory is described and evaluated using Walker and Avant’s criteria. The theory is applied to a population of federal employees who smoke. By increasing employees’ ability to autonomously choose smoking cessation programs, support their competence to stop smoking, and improve their relationships with both others who smoke and employee health services, smoking cessation should increase.
Keywords
Occupational health nurses are challenged to assist employees in maintaining and improving their health. Although nurses can present information and provide specific health programs (e.g., dietary or physical activity programming), it is employees who must engage in the activity and change their health habits which can involve nurses teaching and motivating employees. To better transmit information and motivate behavior change, clinicians and researchers need theoretical frameworks on which to build employee programs or research interventions.
Self-determination theory (SDT) has been applied to various fields of study, including health care and health promotion. This theory focuses on autonomy, competence, and relationships as predictors of performance and health outcomes (Deci & Ryan, 2008). Occupational health nurse clinicians and researchers can use SDT to examine motivating factors that predict behavior change and positive health outcomes in employee health settings. This article includes a description of SDT and an evaluation of its logical adequacy, usefulness, generalizability, and parsimony. The authors briefly describe previous research studies based on this theory and provide practical application of the theory for researchers and clinicians working with federal employees who smoke.
Self Determination Theory Description
The SDT had its origins in psychology; Deci and Ryan (1985) studied students’ behavior in regard to rewards and motivation. In early studies, they investigated how social conditions and human orientations facilitated or undermined human behavior. They defined SDT as a macrotheory that “addresses basic issues as personality development, self-regulation, universal psychological needs, life goals and aspirations, energy and vitality, nonconscious processes, the relations of culture to motivation, and the impact of social environments on motivation, affect, behavior, and well-being” (Deci & Ryan, 2008, p. 182). The theory authors hypothesized that all human beings, regardless of culture or developmental level, had basic psychological needs for autonomy, competence, and relatedness, which can be supported or not supported by social environments (Deci & Ryan, 2000; see Figure 1). When these basic needs are met, individuals are more motivated to change or maintain behaviors. Change is distinguished by the type of motivation (autonomous vs. controlled), not necessarily by how much an individual is motivated to reach a goal or health outcome (Deci & Ryan, 2008).
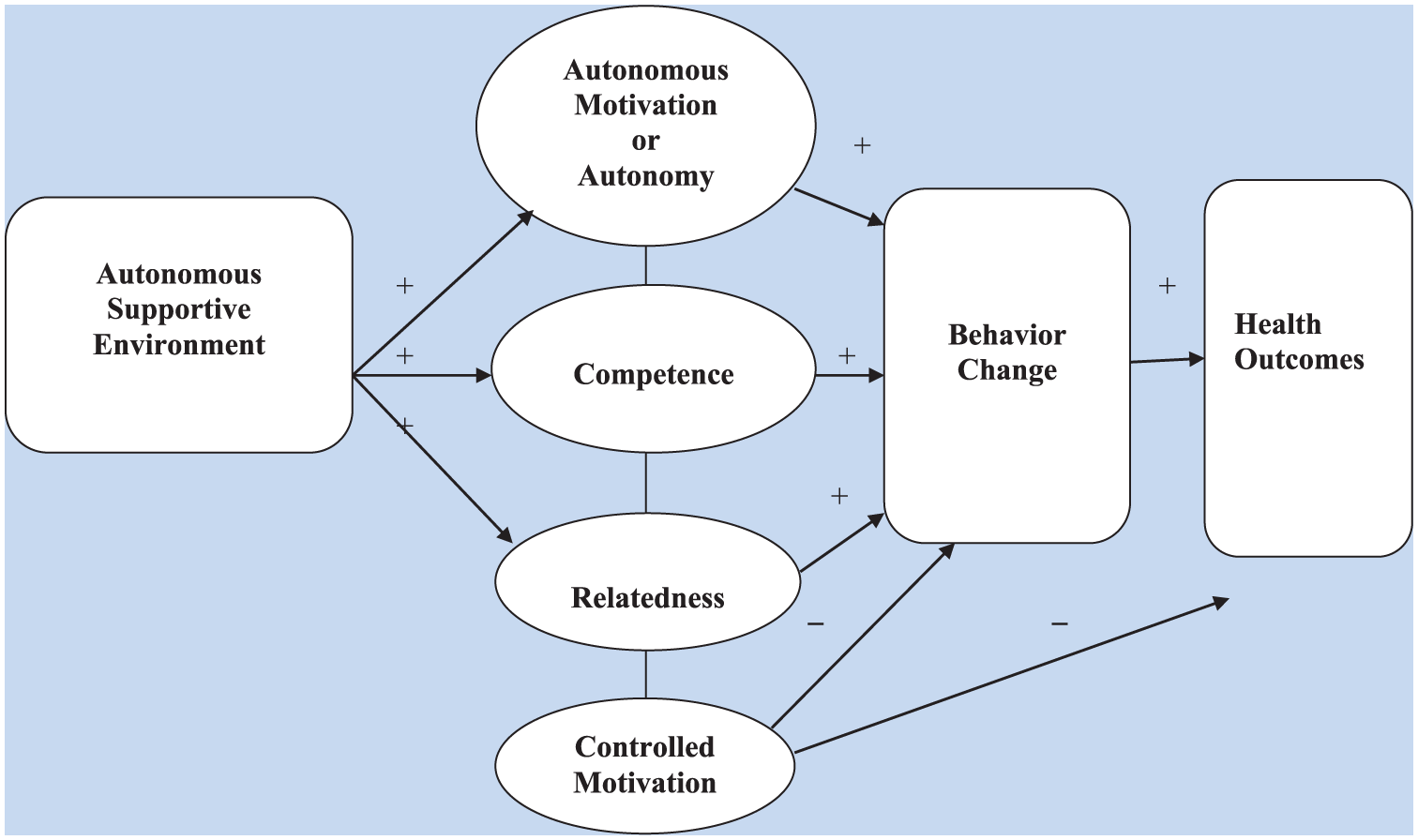
Self-determination theory (created from Deci & Ryan, 2000).
Main Concepts
Autonomous supportive environment
In autonomous supportive environments, individuals are free to provide feedback on decision-making processes as opposed to a controlled environment in which no freedom exists (Williams, Gagné, Ryan, & Deci, 2002). Health care professionals can provide a supportive environment in which individuals can make autonomous decisions and fully participate. For example, when a health professional is nonjudgmental and provides choices, clients are more likely to maintain healthy diets.
Autonomy
Autonomy is defined as self-regulation of life encounters or actions (Ryan & Deci, 2017). When individuals are free to choose specific health behaviors, they are more motivated to maintain behavior change.
Competence
Competence is demonstrated when individuals believe that they can achieve behavior change or health outcomes (Williams et al., 2006b). When individuals feel competent to reach a goal, they are more likely to maintain the behavior. The concept of competence is similar to self-efficacy in Bandura’s (1997) social cognitive theory. The concepts of perceived competence and self-efficacy are not used interchangeably within SDT, but perceived competence and self-efficacy are similar. An example of competence is individuals with hypertension taking their own blood pressure readings at home as part of a hypertension management plan.
Relatedness
Relatedness is defined as a genuine concern and trust in significant others (Williams et al., 2011) and is essential for psychological growth and well-being (Ryan & Deci, 2000). When individuals receive support from others while adopting new health-related behaviors, camaraderie increases motivation to maintain behavior change. For example, individuals engaging in a walking program are more likely to persist if they are walking with friends or coworkers.
Controlled motivation
Motivation is energy that produces an intentional action (Ryan & Deci, 2000). Autonomous motivation is energy for engaging in an action for its inherent satisfaction (i.e., it brings joy) rather than due to external pressures or rewards. In contrast, controlled motivation is energy for participating in an action due to coercion and has no lasting effects on behavioral outcomes. An example of controlled motivation is individuals participating in a weight loss program for incentives. When incentives end, employees are less engaged in the behavior and lose positive health outcomes.
Behavior change
Behavior change results from actively participating in activities or habits that improve psychological or physical health, including avoiding unhealthy behaviors. In health promotion, desired behaviors often include healthy dietary and exercise habits or smoking and alcohol cessation.
Outcomes
Health outcomes include physical and physiological indicators such as depression, anxiety, and quality of life (Ryan, Patrick, Deci, & Williams, 2008). Outcomes are the result of behavior change. For example, employees who perceive significant work-related stress can engage in stress reduction through an SDT-based intervention.
Relationships Between Concepts
Below are explicit relational statements between the concepts included in SDT (Deci & Ryan, 2000; Ryan & Deci, 2000; Ryan et al., 2008; Williams et al., 2002).
An autonomous supportive environment is positively associated with autonomous motivation, competence, and relatedness.
Autonomous motivation, competence, and relatedness are positively associated with positive behavior change.
Controlled motivation is negatively associated with positive behavior change and positive health outcomes.
Behavior change is positively associated with health outcomes.
Evaluation of Self-Determination Theory
A theory is composed of “relational statements that present a systematic view about a phenomenon and that are useful for description, explanation, prediction, and prescription or control” (Walker & Avant, 2011, p. 7). Through theory analysis, nurses can determine the theory’s strengths and weaknesses to support and guide their clinical or research practices. Using Walker and Avant’s (2011) strategies, the authors evaluated SDT for its logical adequacy, usefulness, generalizability, parsimony, and testability. Discussions continued between the authors until both were satisfied with their definitions, relationships among concepts, and application to a group of employees. A literature search of the theory produced several research examples that demonstrated its usefulness and testability. No study was found that used this theory for worksite smoking cessation.
Logical Adequacy
Logical adequacy requires examining the statements and concepts within the theory for structural and faulty reasoning (Walker & Avant, 2011). Self-determination theory has a logical structure. It flows from left to right, with arrows and +/– to indicate relationships. Logical predictions can be made from the theory (e.g., sufficient autonomy and competence can predict positive health behavior change; see Figure 1). A realistic model describing the association between concepts offers a visual representation of the structure and logical flow of the theory.
Usefulness
A theory is useful when nurses can practically apply the theory to predict or understand outcomes (Walker & Avant, 2011). This theory is useful because worker autonomy, competence to perform tasks, and relationships are concepts well known in nursing and easily applicable to multiple health behaviors. Self-determination theory can be used to study health promotion behaviors, self-care for chronic disease, or posthospital rehabilitation. Using SDT as a theoretical framework is a novel approach for worker smoking cessation.
Generalizability
Generalizability is demonstrated by applying the theory widely in various fields of studies or populations (Walker & Avant, 2011). Self-determination theory can be used to explain or predict human motivation and behavior across all cultures and populations. The framework can be broad (studied in many different fields) and behavior specific (e.g., medication adherence or smoking cessation).
Parsimony
Walker and Avant (2011) define a parsimonious theory as one that is succinct and easy to describe or outline. Self-determination theory is parsimonious with seven concepts that can be clearly defined and linked. It would be difficult to predict human motivation with fewer concepts. To provide a simple expression of the theory, the authors created a model to clarify the concepts and relational statements within the theory (see Figure 1). The visual representation aided in explaining the relationships between concepts and increasing the parsimony of the theory.
Testability
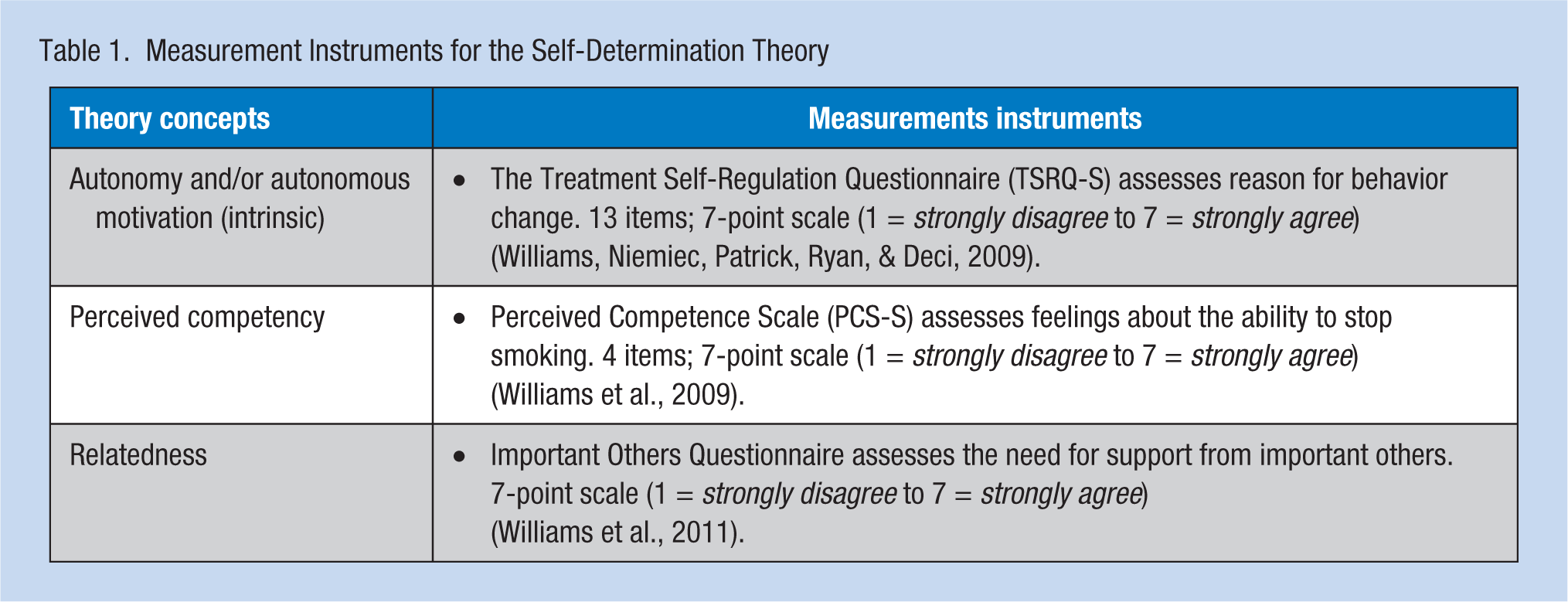
Testability is the ability of clinicians and researchers to use the theory to measure variables and generate hypotheses (Walker & Avant, 2011). A literature review identified conceptual and theoretical definitions for better understanding theory application. Self-determination theory can generate hypotheses that can be tested. The most commonly used instruments are listed (see Table 1). For example, the Treatment Self-Regulation Questionnaire (TSRQ-S; Williams, Niemiec, Patrick, Ryan, & Deci, 2009) has been used to measure long-term smoking abstinence in a large randomized clinical trial. The scale is reliable with acceptable internal consistency for autonomy related to smoking cessation (Cronbach alphas .85 at baseline and .89 at 6 months; Williams et al., 2009). The Perceived Competence Scale (PCS-S; Williams et al., 2009) also demonstrated internal consistency (Cronbach alphas .90 at baseline and .94 at 6 months).
Measurement Instruments for the Self-Determination Theory
Self-Determination Theory in Research
Williams et al. (2006b) applied SDT to smoking cessation and cholesterol-lowering interventions (Williams et al., 2006a). They enrolled 1,006 smokers from a community-based population of low income and less educated adults. Sample mean age was 45.5 years, and 64% were women. Participants were randomly assigned to treatment (n = 714) and comparison (n = 292) groups (Williams et al., 2006b). The comparison group received a booklet about smoking cessation, the results of cholesterol tests, and a list of smoking cessation programs in their geographic area. The treatment group received the same information but then met with study counselors 4 times over a 6-month period. Counselors supported participants in making clear, autonomous decisions about when and how to quit smoking.
At the end of the 6-month intervention, the treatment group was more likely to use medication (p < .001), had more days on medication (p < .001), had a higher point prevalence for smoking cessation (p < .001), and had a higher prolonged abstinence from smoking (p < .001; Williams et al., 2006b). Low density lipoprotein (LDL) cholesterol levels were also significantly reduced (p = .05; Williams et al., 2006a). In addition, the authors conducted structural equation modeling using study data to assess goodness of fit. They found that autonomous motivation predicted medication taking (.20, p < .01) and that perceived competence predicted smoking cessation (.24, p < .01). This theory-based study showed that the concepts in the theory can be measured and that the concepts significantly affect health outcomes in two health areas, smoking and cholesterol.
Pesis-Katz, Williams, Niemiec, and Fiscella (2011) examined the same smoking intervention based on SDT used by Williams et al. (2006b), focusing on the cost-effectiveness of the intervention (n = 737). They found a cost-effectiveness ratio of US$1,258 per quality-adjusted-life-year saved. They concluded that, among insured smokers, the SDT intervention was cost-effective compared with other smoking interventions.
Niven and Markland (2016) used the SDT theory to assess employees participating in a walking challenge in Scotland. Their sample size was 298, mean age 42 years, and 81% of the sample were women. They tested measurement tools for SDT constructs related to walking: the Behavioral Regulations in Walking Questionnaire, Psychological Needs Satisfaction for Walking Scale, and the International Physical Activity Questionnaire-long form (frequency and duration of physical activity in the domains of job-related, domestic, and leisure activity). The researchers found that the theory performed as expected but not for all forms of walking. Walking for leisure versus during work tested differently; walking at work demonstrated no significant relationships between the variables which suggested that workers require different motivation for this specific behavior. The authors concluded that SDT supports changes in walking, but instrument development is needed (Niven & Markland, 2016).
In summary, SDT has been used in several intervention studies with smoking cessation, cholesterol management, and walking behaviors. All studies included adult samples, with more women than men. Positive health outcomes were documented, and structural equation modeling was successful. All findings indicated continued use of SDT to understand motivating positive behavior change.
Application of Self-Determination Theory to Federal Employees Who Smoke
Self-determination theory can be applied to federal employee smoking cessation; both the theory and the problem have a human motivation component. Clinicians have smoking cessation tools in their arsenal, but motivating workers to use these tools remains a challenge. The U.S. Office of Personnel Management (U.S. OPM; U.S. OPM, Planning and Policy Analysis, 2014) surveyed the Federal Employee Health Benefits (FEHB) population about their tobacco use, accessing a random sample of 40,000 nonseasonal executive branch employees. Sixty-five percent of these employees reported having used tobacco products within the last 30 days. The U.S. OPM must continue to encourage these employees to reduce or eliminate tobacco products.
Autonomous Supportive Environment
Currently, the available on-site smoking cessation programs consist of two counseling sessions a year and nicotine replacement patches, a 4-week to 6-week supply of transdermal patches, nicotine lozenges, or nicotine chewing gum. According to SDT, if employees do not feel supported, they will not change their smoking behavior. Federal employers and supervisors need a supportive environment for employees who are ready to quit smoking. These employees also need choices regarding smoking cessation programming (e.g., choosing among cessation programs, when cessation will begin, and how programs will be accessed).
Competence
Smoking cessation competence refers to employees’ abilities to use nicotine patches, nicotine gum, or counseling to decrease tobacco use. When employees feel competent in their ability to use a product or participate in a program, they are more likely to maintain new behaviors. Clinicians must teach employees how to use products and provide advice and encouragement to employees. To further support competence, clinicians can provide relevant feedback, be positive about the process, and encourage employees to develop problem-solving skills (Williams et al., 2011). Perceived competence is positively associated with psychological and physical wellness (Deci & Ryan, 2000). Employees must learn to set small attainable goals and evaluate progress during health unit visits or counseling sessions.
Relatedness
Active smokers who develop relationships with other smokers who have similar desires to quit are more likely to engage in smoking cessation programs. These relationships can occur at the workplace during the workday. The addition of at-home supportive relationships is also essential, as family members and friends can sabotage cessation efforts if they are smokers themselves. When supporting relatedness, providers can develop interpersonal yet professional relationships with employees while remaining nonjudgmental. Developing trust and providing a warm and inviting relationship improve employee interactions.
Controlled Motivation
Employees are more likely to change smoking behaviors if the environment is not controlled by supervisors or health care personnel. The motivation to act must be internal. Employers can offer rewards for progress toward smoking cessation, but threatening punishment will not result in positive outcomes.
Behavior Change
Desired behavior changes include decreasing the number of cigarettes smoked daily, using nicotine patches or gum, calling a counselor, or eliminating smoking. The ultimate desired outcome is long-term smoking cessation. The more autonomy, competence, and relatedness employees feel within a supportive work environment, the more likely they are to persist in achieving cessation.
Policy Change
In 2003, federal employee health plans provided some coverage, but none provided comprehensive smoking cessation interventions (U.S. OPM, Planning and Policy Analysis, 2014). Some federal agencies offer on-site smoking cessation programs or interventions, but not all. Under the on-site employee sponsored smoking cessation program, prescription-based products such as Chantix (varenicline tartrate) and Zyban (bupropion hydrochloride) are not offered. The U.S. OPM should consider adding employee health benefits at all federal agencies and workplaces, including prescription medications. The more options offered to employees, the more likely these employees are to eliminate tobacco.
Future Research Questions
Self-determination theory suggests possible research questions for a federal employee population. Researchers could describe federal employees’ perceptions of management support for smoking cessation, their perceived autonomy to act, their sense of competence to engage in nonsmoking habits, and their degree of relatedness to others who smoke. The concepts within the theory could become items on an assessment or measurement tool to discover how ready an employee is to quit smoking. Interventions such as on-site smoking cessation programs and prescription-based products should be tested for their impact on cessation rates, motivation to seek professional assistance in quitting smoking, or employee engagement in smoking cessation programs within the federal employee population.
Conclusion
As theory creates the foundations of nursing practice, occupational health nurses can use their clinical and research skills to explain and confirm theoretical propositions to advance health outcomes and well-being of employee populations. Knowledge of the SDT, a motivation-based theory, can predict behavior change and promote health outcomes such as smoking cessation. As comprehensive smoking interventions are needed in employee health settings, it is occupational health nurses who can provide autonomous supportive environments and positive interactions with employees who smoke.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Brenda M. Ross is a regional nurse manager at the Federal Occupational Health agency. She is currently a PhD nursing student at the University of Texas at Arlington, studying smoking cessation in federal employees.
Donelle M. Barnes is an associate professor of nursing at the University of Texas at Arlington. She teaches nursing philosophy and theory to doctoral students every year.