
Abstract
A 36-year-old woman sustained a Grade 2 ankle sprain at work. Two days after the injury, the ankle and foot became red and she complained of “intense burning pain.” First diagnosed with complex reflex sympathetic dystrophy, the employee was prescribed medications that provided some pain relief; a subsequent temporary nerve block provided additional relief. However, the symptoms returned and she was treated unsuccessfully with surgical sympathectomy. The employee was referred to a neurologist and diagnosed with primary erythromelalgia, a rare pain disorder that can be mistaken as complex reflex sympathetic dystrophy.
Keywords
SW is a 36-year-old woman who sustained a left Grade 2 ankle sprain at work. SW, an electrocardiogram (EKG) technician, tripped over a cord, twisted her ankle, and reported to employee health. The occupational health nurse noted mild swelling and tenderness on the medial aspect of the left ankle. Pulses were present and an X-ray was negative for fractures. SW had an unremarkable health history. She did, however, report a 15-pack-year smoking history and used nicotine patches to eliminate the habit. Family history consisted of cardiovascular disease in both paternal and maternal sides of the family. SW was prescribed ibuprofen, placed on light duty, and encouraged to wear shoes that provided support. A sitting job was available for light duty. A second appointment was made for 1 week.
Three days later, SW reported to employee health reporting an intense burning sensation in her left ankle and foot. Upon physical examination, the left ankle and foot were exceptionally warm and of an “intense red color” compared with the right ankle and foot. Tenderness without swelling was documented on the entire left ankle and foot. SW reported no new injuries; however, she did report that she had bought a new pair of athletic shoes after her appointment so that she would have the support needed for her ankle injury. The shoes were very tight due to the swelling, but she wore them anyway with the expectation that the shoes would fit better when the swelling decreased. She also reported that the pain and redness “comes and goes” without a specific stimuli.
Due to the intense pain, the intense erythema, and unsure of the diagnosis, SW was referred to an orthopedist the same day. The orthopedic surgeon prescribed Vicodin and Ibuprofen. SW had full range of motion in the ankle and pulses present; however, there was a decrease in sensation upon light touch. In addition, SW continued to experience erythema and an intense burning sensation. Once again, SW was given sitting duties with no weight bearing on the left foot. The orthopedic surgeon referred SW to pain management suspecting complex reflex sympathetic dystrophy (CRSD).
SW reported that the Vicodin and Ibuprofen provided little pain relief. The pain management physician prescribed Oxycontin and Ibuprofen. He also ordered electromyography and nerve conduction studies to measure nerve and muscle damage and confirm the diagnosis of CRSD. However, these tests results were inconclusive. SW was also prescribed Pregabalin for the neuropathic pain and was scheduled another appointment in 2 weeks.
SW reported mild pain relief from Pregabalin. The pain and redness continued to spontaneously appear but she did notice that smoking precipitated these symptoms. She also reported that elevation and a cooling fan also provided some pain relief. The pain management physician scheduled her first for a nerve block, which provided some relief, and 2 months after the initial injury, scheduled a surgical sympathectomy, which provided additional relief.
However, SW continued to experience spontaneous burning pain and redness. She continued Pregabalin and Ibuprofen as prescribed, and Oxycontin as needed. During this time, SW was unable to work due to the pain and filed disability. SW was referred to neurology for further evaluation.
Four months after the initial injury, SW was evaluated by neurology. SW showed the neurologist pictures of her ankle and foot during acute attacks. The neurologist reviewed the electromyography and nerve conduction studies as well as the pain management notes. Thermal studies that measured heat production when provoked by various stimuli were ordered. The tests revealed increased sensory threshold that resulted in higher temperature and redness. SW was diagnosed with primary erythromelalgia and referred to inpatient services for plasmapheresis.
Erythromelalgia
Erythromelalgia is a neuropathy caused by a mutation of the voltage-gated sodium channel (Cregg, Cox, Bennett, Wood, & Werdehausen, 2014). This mutation causes hyperexcitability of the sodium channel, so the nerves are more susceptible to stimuli which results in an intense burning sensation and erythema (Kist et al., 2016). Erythromelalgia is categorized as a small fiber neuropathy disorder (Brouwer et al., 2014). Small fiber neuropathy results from damage to peripheral nerves, either small myelinated (Aδ) or unmyelinated C fibers (Hovaguimian & Gibbons, 2011). Small fiber types involve both somatic and autonomic nervous systems that affect thermal and pain perception of cutaneous tissues (Brouwer et al., 2014).
The patient usually reports episodic burning pain, intense heat, and erythema, which are relieved by cooling the extremity (Kist et al., 2016). Usually, both extremities are affected, but the affliction can also be unilateral (Blake, Mortimore, & De Ambrosis, 2016). An episode of erythromelalgia may be triggered by mild exercise, temperature change, or wearing clothes (Kist et al., 2016). Alcohol, caffeine, and spicy foods may also be triggers (U.S. Department of Health & Human Services, 2016). Another trigger may be leg dependence while sitting (Tang, Chen, Tang, & Jiang, 2015).
Erythromelalgia is either primary or secondary. Primary erythromelalgia is the most common, an autosomal dominant neuropathy present in diverse populations (Tang et al., 2015). The onset of primary erythromelalgia is unclear other than genetics (Tang et al., 2015). Secondary erythromelalgia is usually associated with a myeloproliferative or autoimmune disorder such as diabetes mellitus, vasculitis, or lupus (Blake et al., 2016).
Diagnostics
The diagnosis of erythromelalgia is based on health history and physical examination (Hovaguimian & Gibbons, 2011). Thermal studies, such as quantitative sensory testing (QST) and thermoregulatory sweat testing, can be used to detect heat and heat-evoked potentials (contact heat evoked potentials [CHEPs]). These tests measure rapid cycles of heat that may be used to confirm the diagnosis of small fiber neuropathy (Hovaguimian & Gibbons, 2011). However, electromyography and nerve conduction studies are often used to detect larger myelinated sensory motor fibers, not small fiber neuropathies (Hovaguimian & Gibbons, 2011). Genetic testing may detect 20 mutations in SCN9A that have been linked to erythromelalgia (Kist et al., 2016). Imaging may be used to diagnose other underlying diseases (U.S. Department of Health & Human Services, 2016). A skin biopsy may show inflammation (U.S. Department of Health & Human Services, 2016).
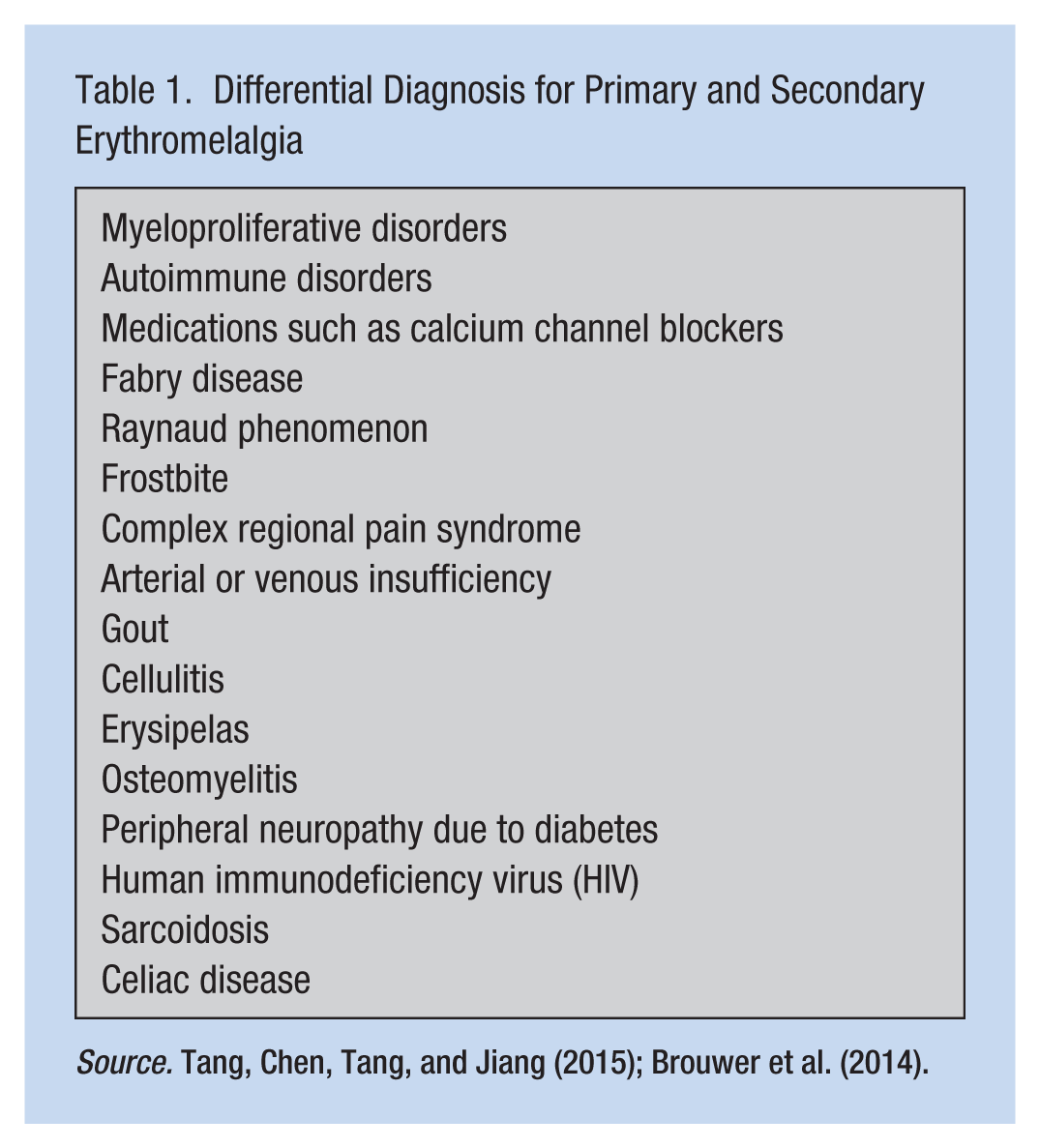
Underlying disorders (e.g., autoimmune disorders) should be noted to differentiate between primary and secondary erythromelalgia, and the underlying disease treated as appropriate. Differential diagnosis should be considered as well (Table 1). A complete blood count and metabolic panel may be used to assist in differential diagnoses. Other than genetic testing, no other biologic markers exist (Tang et al., 2015).
Differential Diagnosis for Primary and Secondary Erythromelalgia
Treatment Options
Several different classes of medications are commonly used to treat neuropathic pain; however, their effectiveness for the treatment of erythromelalgia may be limited (Tang et al., 2015). Narcotics may be used for breakthrough pain but, due to their addictive nature, should be avoided. For secondary erythromelalgia, the underlying disease should be treated. Some treatment options may include plasmapheresis or prednisone in the case of autoimmune diseases (Paticoff, Valovska, Nedeljkovic, & Oaklander, 2007).
Medications that block sodium channels, such as topical Lidocaine or Lidocaine patch, may be used for breakthrough pain. Oral medications such as Carbamazepine and Mexiletine may be effective by decreasing voltage dependence and resulting excitability (Tang et al., 2015). Topical Capsaicin may be used as well (Paticoff et al., 2007).
Pregabalin is an oral medication used to block voltage-gated α2δ calcium channels and is a presynaptic inhibitor of the release of glutamate, substance P, and calcitonin gene–related peptide. Gabapentin acts on the voltage-gated α2δ calcium channel as well, and in addition, it limits the release of excitatory neurotransmitters.
Nonpharmacologic options may be considered as well. Some workers may benefit from a cool environment; soft socks and foot tents may relieve pain or precipitate an episode by decreasing stimuli (Tang et al., 2015). However, thermal cooling may lead to ulcerations and possible gangrene due to constant exposure to low temperatures (Tang et al., 2015). Workers may need to avoid triggers, including Niacin, which may also precipitate an episode (Paticoff et al., 2007).
Erythromelalgia Versus CRSD
Erythromelalgia may be mistaken for CRSD; CRSD Type 1 usually presents after an injury or trauma such as surgery, and Type 2 is usually due to peripheral nerve injury as in the case of herpes zoster (U.S. Department of Health & Human Services, 2016). Type 1 usually occurs approximately 3 months from the initial trauma (National Organization for Rare Diseases [NORD], 2017). Complex reflex sympathetic disorder involves both small unmyelinated and small myelinated sensory and motor nerve fibers. Eventually, the central nervous system is affected, resulting in circulatory and temperature changes in the affected limb (Kim et al., 2017). Changes in the central nervous system involve the somatosensory cortex, insula (the part of the limbic system that relays and integrates bodily sensations such as pain and emotions), and some areas of the cortex and subcortex (Kim et al., 2017).
A history of smoking may be a risk factor. Constant and prolonged pain is a key indicator of CRSD, the result of vasoconstriction as well as vasodilation, and the inflammatory response (NORD, 2017). The inflammatory response secretes cytokines, which cause further damage and pain (Bharwani et al., 2017). Other signs and symptoms are hyperalgesia, edema, allodynia, and skin changes. The constant pain is thought to be due to sustained sympathetic nervous activation (NIH, 2017). The affected limb may become red, white, or blue. Swelling and impaired motor function occur as well. Eventually, atrophy of the skin may occur with the skin appearing to be thin, shiny, cool, and hairless (NORD, 2017).
Diagnostics that reflect the inflammatory response such as complete blood count, erythrocyte sedimentation rate, or C-reactive protein may be inconclusive. Imaging diagnostics such as a magnetic resonance imaging (MRI) may reveal excessive bone demineralization but is not conclusive of CRSD (Kim et al., 2017). A literature search using PubMed, MEDLINE, and CINAHL did not reveal a genetic component.
Treatment options may be the same medication regimen as erythromelalgia; however, sympathetic nerve blocks and surgical sympathectomy may also be considered. Surgical sympathectomy procedures should only be considered if temporary nerve blocks are successful (NORD, 2017). Ibuprofen may relieve the pain due to its anti-inflammatory properties (NIH, 2017).
Implications for Occupational Health Nurses
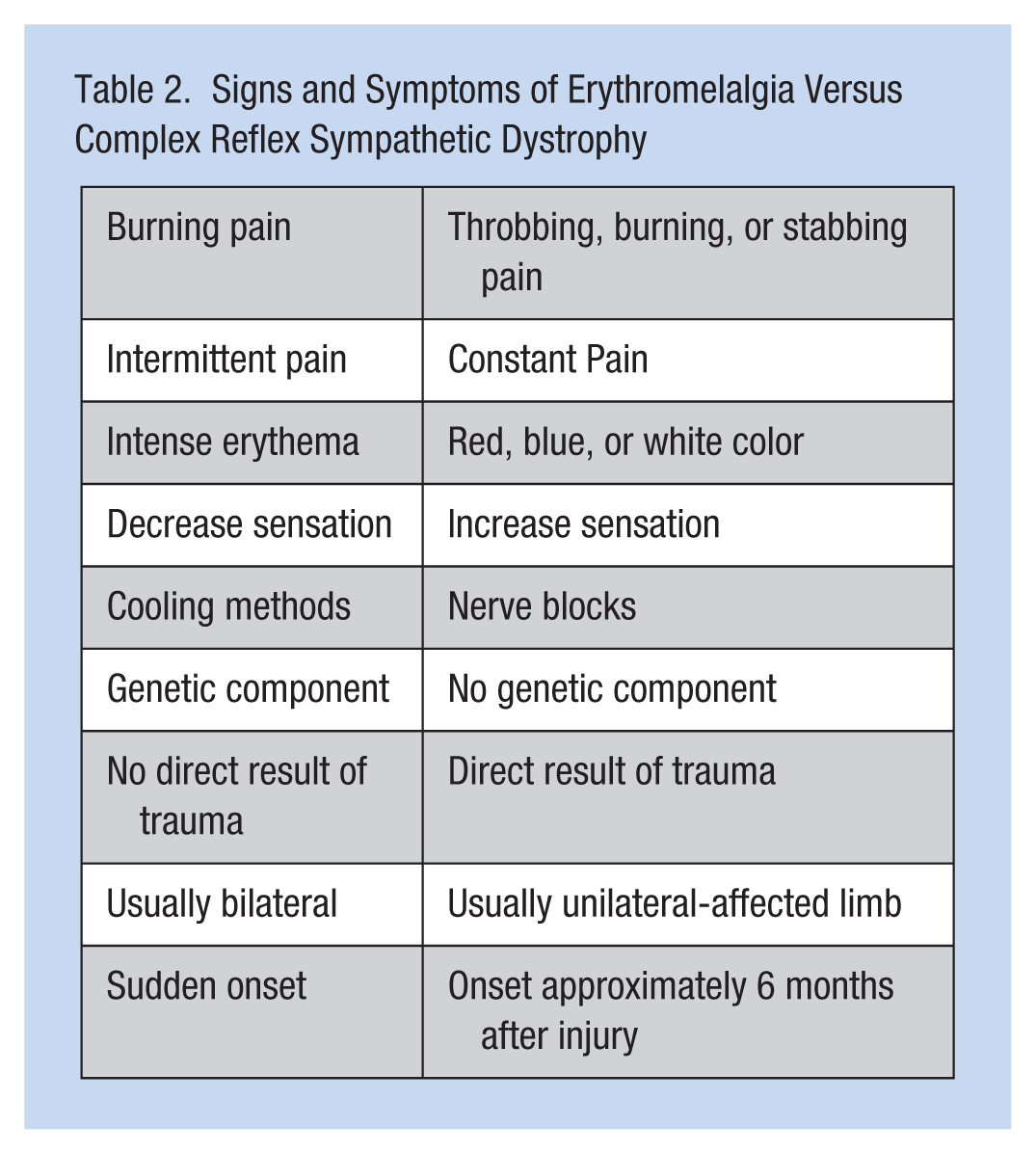
It is very difficult to differentiate between erythromelalgia and CRSD (Table 2). Episodic pain versus constant pain may be used to differentiate between the two disorders. A family history and underlying disorders may assist in the diagnosis. Erythromelalgia usually is not a result of trauma and bilateral. Complex reflex sympathetic disorder usually has a hypersensitive response to stimuli, whereas erythromelalgia may decrease sensation. The timing of each disorder may differ as well.
Signs and Symptoms of Erythromelalgia Versus Complex Reflex Sympathetic Dystrophy
Lifestyle modifications can decrease acute episodes of primary erythromelalgia. Special accommodations in the workplace may be recommended. Providing a cool work environment is optimal. If these employees sit for most of the workday, providing a fan and the opportunity to elevate the affected limb or limbs may help. The employee should be encouraged to itemize stimuli that provoke attacks. Exercise may be a challenge for these employees; it may be necessary for employees to engage in yoga exercises or Pilates because these exercises promote circulation and may not provoke attacks. Prolonged walking may be a challenge, so these employees need opportunities to sit. Some employees may need to avoid tight shoes and instead wear open sandals with no socks. The use of tobacco products should be eliminated due to the negative cardiovascular effects. Ice packs may be offered but should be limited due to adverse vasoconstriction effects.
Conclusion
SW was positive for the mutation of SCN9A. The neurologist suspected that the injury precipitated the episode of primary erythromelalgia. SW discontinued smoking. Her left ankle injury and the complication of erythromelalgia were covered under workers’ compensation. However, due to the positive genetic test, the primary erythromelalgia was considered to be a preexisting condition, and future care was paid for by private insurance. SW returned to work and avoided stimuli that could precipitate an attack. She assumed a job in telemetry, and was provided a fan and the opportunity to elevate her legs as needed. She continued with Pregabalin as scheduled and discontinued the use of Oxycontin.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann Regina Lurati is a nursing lecturer at California State University, Monterey Bay.