
Abstract
Computers and other digital devices are commonly used both in the workplace and during leisure time. Computer vision syndrome (CVS) is a new health-related condition that negatively affects workers. This article reviews the pathology of and interventions for CVS with implications for the occupational health nurse.
H.O, a computer programmer for the past 30 years, is a 54-year-old woman who presents to employee health with complaints of eye fatigue and irritation. She states that she uses the computer during her 8-hour shift and uses the computer at home for leisure. She denies any history of smoking or alcohol use. Her past health history includes gastroesophageal reflex disease for which she is prescribed an over-the-counter proton pump inhibitor. She also states that during the past 10 years, she has taken Benadryl for sleep once a week, usually on Sundays.
HO states that she has been wearing sunglasses for the past 35 years and that her sunglasses have always provided ultraviolet (UV) protection. She developed visual problems in her late 30s. She could not read small print and started wearing “cheaters” that she bought in the supermarket. She had her first full ophthalmology examination at the age of 43. She had always had 20/20 vision but during this examination, her distance vision was 20/70 in her left eye, and 20/100 in her right eye. She was prescribed progressive lens for both reading and distance. It was recommended that she have a full ophthalmology examination every year.
When HO was 51 years old, she was diagnosed with bilateral narrow angle closure and received bilateral laser iridotomies. The surgery was uneventful and minimal change to her prescription glasses followed. During her last ophthalmology examination, HO complained of eye fatigue and irritation. She states that she feels a burning sensation in both eyes. The ophthalmologist diagnosed dry eyes and small cataracts developing in each eye. HO asked if her eye problems were related to her computer use and the ophthalmologist provided information concerning computer vision syndrome (CVS).
CVS
Computer use and the use of digital devices have become common both in the workplace and away from work. However, the use of computers and other visual display terminals (VDTs) may have negative effects on vision (Ranasinghe et al., 2016). Computer vision syndrome, a phenomenon associated with the use of VDTs, has symptoms of eyestrain, headaches, dry eye, diplopia, and blurred vision, and is also referred to as asthenopia (Rosenfield, 2011). The first component involves external sensations associated with dry eyes (e.g., burning and irritation); the second component involves internal symptoms (e.g., headaches or diplopia; Rosenfield, 2011).
Workers who spend more than 4 hours per day at continuous computer work are at risk of CVS (Gowrisankaran & Sheedy, 2015). Other risk factors that contribute to external symptoms of CVS are amount of glare and light exposure, font size, and gaze (Gowrisankaran & Sheedy, 2015). Other risk factors that contribute to internal symptoms are refractive errors such as near and far sightedness and astigmatism, excess convergence or reading at close distance, poor accommodation or the ability to focus, and age-related presbyopia (Gowrisankaran & Sheedy, 2015).
Musculoskeletal symptoms, neck and back pain, and shoulder, wrist, and finger discomfort can also be part of CVS. Postural demands of computer work as well as less static demand on the muscles contribute to eye fatigue (Gowrisankaran & Sheedy, 2015).
Dry eye syndrome or dysfunctional tear syndrome (DTS) may be the result of CVS as well as environmental factors, systemic disease (Sidebar 1), and medications (Sidebar 2; Moshirfar et al., 2014). Diseases (e.g., diabetes and vascular diseases) may damage ocular blood vessels; smoking not only damages blood vessels but may also act as an ocular irritant.
Risk Factors for Computer Vision Syndrome
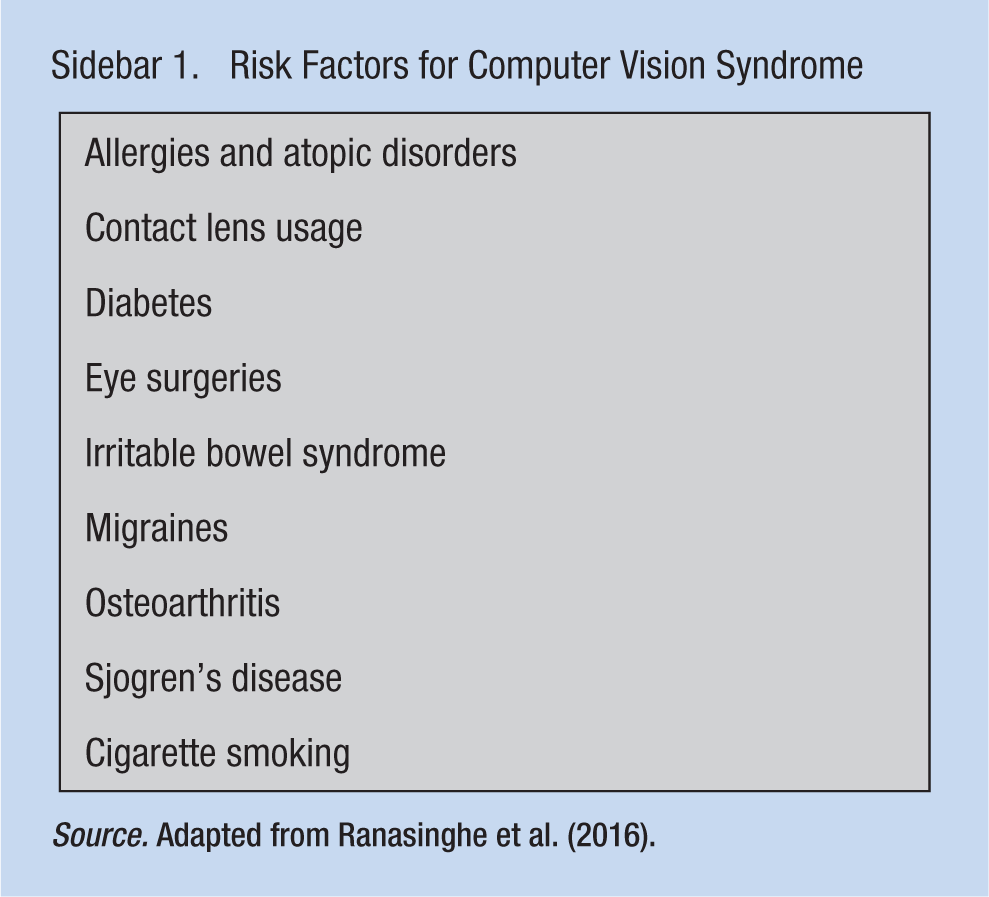
Source. Adapted from Ranasinghe et al. (2016).
Medications
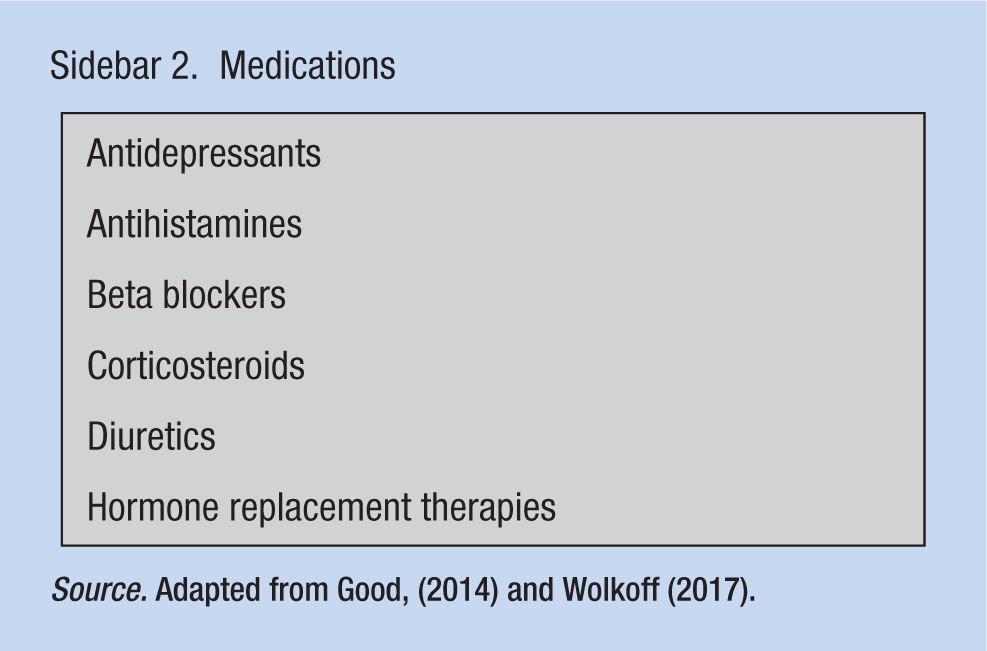
Source. Adapted from Good, (2014) and Wolkoff (2017).
Beta blockers can have negative effects on the eye by lowering lysozyme levels that protect the cornea, immunoglobulin A, and aqueous production. Diuretics reduce lacrimation. Antihistamines reduce mucous and aqueous production, especially when combined with anticholinergics, and can cause mydriasis and decrease papillary response in bright lights. Hormone replacement therapy is believed to decrease the aqueous component of precorneal tear film. Antidepressants may have anticholinergic effects. Nonsteroidals may cause refractive changes and narcotics decrease tear secretions. Vitamin A derivatives, used for acne treatment, may reduce oil production. Proton pump inhibitors may cause dry eyes due to H2 receptor antagonistic effects. Chemotherapy may cause less tear and oil production (American Optometric Association [AOA], 2017).
Dysfunctional tear production may lead to visual distortions and discomfort and limit work performance (Cohen, Martin, & Sall, 2014; Kawashima et al., 2015). Human tears consist of electrolytes, water, proteins (e.g., antibodies and lysozymes), and lipids that moisturize the surface of the eye and decrease the risk of damage to the cornea; less eye lubrication may increase the risk of eye infections and fibrosis (Moshirfar et al., 2014). Artificial lubricating tears may relieve symptoms of dry eye as well as provide eye protection.
Another aspect of CVS that contributes to DTS is the impaired blink reflex during computer use (Kawashima et al., 2015). Blinking provides constant lubrication that stimulates secretion of tears and an aqueous mucin glycoprotein that protects the eye (Wolkoff, 2017). During computer use, workers adopt a gaze angle that exposes a greater ocular surface which leads to greater tear evaporation and resulting DTS (Gowrisankaran & Sheedy, 2015). Heat generated by the computer may also lead to dry eyes (Agarwal, Goel, & Sharma, 2013).
Computer vision syndrome may be the result of hyperexcitability of the visual cortex (Evans & Allen, 2016). The use of computers has increased exposure to short-wavelength (450 nm to 495 nm on the high-energy visible light spectrum) light, which is mostly blue light, and can damage the retina and contribute to eye fatigue (Kuse, Ogawa, Tsuruma, Shimazawa, & Hara, 2014; Lin, Gerratt, Bassi, & Apte, 2017). Damage to the retina leads to the production of oxidative stress and a buildup of lipofuscin, a by-product of lysosomal activity, which increases the retina’s susceptibility to damage (Tosini, Ferguson, & Tsubota, 2016).
Blue light is considered phototoxic to the retina (O’Hagan, Khazova, & Price, 2016). Blue light exposure has been linked to such retinal diseases as age-related macular degeneration (Kuse et al., 2014). It is speculated that blue light causes degeneration of the retinal pigment epithelial cells that leads to oxidative stress, cell death and, finally, vision loss (Kuse et al., 2014).
Continuous exposure to blue, short-wavelength light may also disrupt circadian rhythms and affect sleep quality (Lin et al., 2017) by suppressing melatonin levels that interfere with sleep (Tosini et al., 2016). However, a lack of blue light during the day may also interfere with sleep quality (Tosini et al., 2016). Blue light exposure supports alertness, vigilance, and wakefulness, and for this reason, blue light should be avoided prior to sleep (Good, 2014). Finally, night shift workers should have blue light exposure before going home to increase their alertness when driving (Good, 2014).
Interventions
The use of colored filters may decrease the negative effects of computer use (Evans, Allen, & Wilkins, 2016). Each computer may be fitted with an antireflection filter to reduce eyestrain by reducing glare and improving computer imagery and operator comfort (Gowrisankaran & Sheedy, 2015). The brightness or luminance should be adjusted for the environment (Agarwal et al., 2013).
The use of short-wavelength blocking eyeglasses may decrease visual fatigue and discomfort (Lin et al., 2017). Specific blue light filtering glasses do not interfere with visual performance or sleep quality (Leung, Wing-hong Li, & Kee, 2017). When prescribing glasses, ophthalmologists may consider viewing distance and gaze angle (Gowrisankaran & Sheedy, 2015). Lenses made of polycarbonate and trivex are most effective in blocking UV-A and UV-B radiation (Good, 2014). Tinted lenses are recommended; gray-tinted lenses reduce light from the entire light spectrum (Good, 2014). Contact lenses that block the negative effects of light and radiation may provide more protection because they cover more ocular surface than glasses (Good, 2014).
Monitors should be placed at or below eye level to reduce eye fatigue (Kawashima et al., 2015). Workers may be instructed to take frequent breaks or look into the distance, away from the computer (Gowrisankaran & Sheedy, 2015). Larger display units as well as working at a comfortable distance, between 45 and 60 cm from the monitor, may improve CVS (Gowrisankaran & Sheedy, 2015). Working at a close distance requires greater accommodation, overworking eye muscles, leading to eye fatigue (Agarwal et al., 2013). High resolution improves readability (Gowrisankaran & Sheedy, 2015). Glare should be avoided by placing computers away from lighting sources. Diffuse reflections on the computer are contributing factors to CVS (Agarwal et al., 2013).
The work environment should have adequate humidity (Gowrisankaran & Sheedy, 2015); dust and other irritants, which may irritate the eyes especially for workers who have histories of dry eyes, must be minimized (Wolkoff, 2017). High altitudes and low pressure environments also can dry the eyes (Wolkoff, 2017).
Implications for Occupational Health Nurses
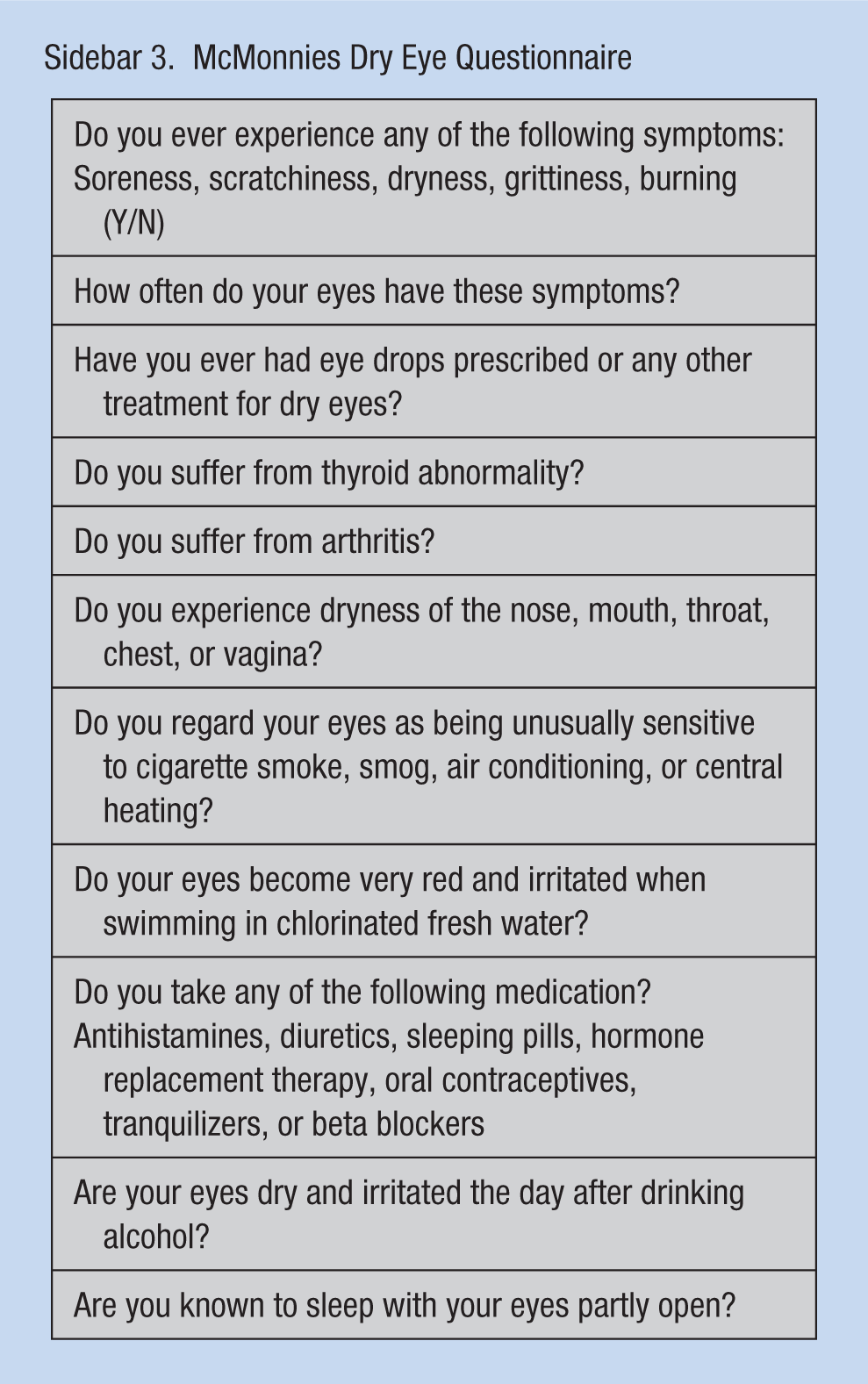
It is recommended that employees have annual ophthalmology examinations to assess both refractive status as well as binocular vision after the age of 40 (American Academy of Ophthalmology [AAO], 2014) because antioxidant mechanisms and protective enzymes begin to decrease at this age (Evans & Allen, 2016; Good, 2014). Computer vision syndrome is difficult to diagnose; however, underlying eye disorders that contribute to CVS can be treated (Evans & Allen, 2016). A questionnaire, such as McMonnies Dry Eye Questionnaire (Sidebar 3), may be administered to assess for DTS (Kawashima et al., 2015). The occupational health nurse may refer employees to their ophthalmologist for lubricating eye drop prescriptions to treat dry eyes. Those employees at risk for dry eyes should not wear contact lens while performing computer work (Wolkoff, 2017). All risk factors for CVS and DTS should be reviewed and employees counseled (e.g., to take breaks to alleviate musculoskeletal and eye strain).
McMonnies Dry Eye Questionnaire
Supplements (e.g., N-acetylcysteine and Vitamin E) may mitigate the negative effects of blue light (Kuse et al., 2014). N-acetylcysteine inhibits oxidative stress (Kuse et al., 2014). Another nutrient, lutein, is believed to reverse retinal damage (Tosini et al., 2016). Other nutrients that maintain retinal health include β-carotene, Vitamin C, and lycopene and are all considered antioxidative (Lima, Rosen, & Farah, 2016). A variety of over-the-counter nutrient supplements that support eye health should be discussed by ophthalmologist with workers along with avoiding alcohol (Wolkoff, 2017).
To improve sleep quality and reduce overall fatigue, it is recommended that workers avoid using a digital device prior to sleep due to excessive blue light exposure (Tosini et al., 2016). Untreated CVS may lead to chronic overall stress, so improving the symptoms of CVS is critical (Ostrovsky, Ribak, Pereg, & Gaton, 2012).
Air pollution (e.g., organic volatiles and particles that irritate the eye) can be reduced with high-efficiency particulate air filtering (Wolkoff, 2017). Humidifying the air (57%-74%) is recommended to maintain adequate moisture in the environment and room temperatures should be set to avoid extreme conditions (Wolkoff, 2017). Minimal cosmetic use and facial scrub elimination are recommended due to irritants in cosmetics and the drying effects of facial scrubs (Wolkoff, 2017).
Conclusion
A literature search of PubMed, Medline, and CINAHL databases used CVS, digital devices, blue light short wavelength, glaucoma, and cataracts key words and did not find any evidence that linked the use of digital devices to glaucoma and cataracts.
Osborne, Lascaratos, Bron, Chidlow, and Wood (2006) hypothesized that blue light could be a risk factor for glaucoma and other optic mitochondrial neuropathies. It is speculated that blue light damages the mitochondria in the retina, contributing to oxidative stress. The accumulation of yellow chromophores, specialized atoms that are responsible for absorbing light, occurs with aging and allows the lens to absorb shorter wavelengths thus damaging the mitochondria and associated retinal ganglion cells. Eventually, as with primary open angle glaucoma, optic atrophy occurs along with vascular changes that lead to an increase in intraocular pressure. Exposure to UV radiation may be a risk factor for cataracts (Lofgren, 2016). However, it is uncertain whether blue light exposure is a risk factor (Good, 2014).
Workers with cataracts absorb less blue light, which could explain why these individuals may experience diminished sleep quality, and then, when the cataract is removed and a new lens is in place absorb more blue light, sleep is improved (Youssef, Sheiban, & Albert, 2011).
Due to her past surgical history of bilateral iridotomies, HO was at risk for DTS, so she was instructed to use lubricating eye drops as needed. It is speculated that laser surgery to the eye increases the osmolarity as well as loss of conjunctival goblet cells that secrete lubricating oils and mucin which leads to dry eyes. Finally, laser surgery may change the shape of the cornea and interfere with the relationship between the eyelids and ocular surface that disturbs normal blinking patterns (Shtein, 2011). HO should continue with the proton pump inhibitor due to her severe reflex disease. She should discontinue antihistamines for sleep.
HO requested a filter for her computer and had an ergonomic evaluation so she can work sitting or standing with her monitor at eye level. She continues to wear her progressive prescription lens at the computer and prescription sunglasses with UV radiation and visible light protection. She was also encouraged to wear a wide-brimmed hat when outdoors to further block the effects of UV radiation and blue light.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann Regina Lurati is a nursing lecturer at California State University at Monterey Bay.