
Abstract
Retinal artery occlusion is an unusual phenomenon in younger patients without background of diseases leading to hypercoagulable states. COVID-19 infection is increasingly recognised as being associated with thrombotic conditions. We present a case of a young female who is otherwise fit and well apart from recent COVID-19 infection, who presented with a mixed cilioretinal artery and venous occlusion.
Introduction
Retinal artery occlusion is a potentially blinding condition leading to retinal ischaemia and vision loss. There have been several case reports and reviews in the literature of this condition associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.1,2
Patients who present with retinal artery occlusion of any kind are investigated for underlying causes or exacerbating factors for arterial occlusions. It is less common for it to occur in a younger population, especially those outside the typical age group associated with atherosclerotic diseases.3,4 We present a case of a young patient in their fourties who is otherwise fit and well presenting with a cilioretinal artery occlusion and combined central retinal vein occlusion to the eye emergency clinic during the COVID-19 pandemic.
Case report
A 47-year-old female complained of a 1–2 week history of blurred vision in the right eye. She had just returned from a short-haul holiday abroad 3 weeks previously.
She had no significant past medical history, there was no family history of any conditions of concern, she was not taking any medication and there was no social history of note.
Findings
On initial presentation, the patient felt generally well and denied any systemic symptoms. The initial examination revealed Snellen visual acuity of 6/12 in the right eye with pin hole to 6/9. The left eye acuity was 6/6. The anterior segment examination was unremarkable, pupil exam revealed a right relative afferent pupillary defect (RAPD). Extraocular movements and intraocular pressures were unremarkable, and the patient was phakic with clear and attached vitreous.
Dilated fundoscopy and optical coherence tomography (OCT) imaging of the right eye is shown below. Figure 1 shows an area of retinal ischaemia nasal to the fovea, likely secondary to a cilioretinal artery occlusion. In addition, there were diffuse blot and flame haemorrhage scattered through the entire retina of that right eye. Corresponding OCT images in Figure 1 show corresponding thickened inner retinal layers consistent with an acute ischaemic insult to the retina. Dilated examination of the left eye was unremarkable (Figure 2).
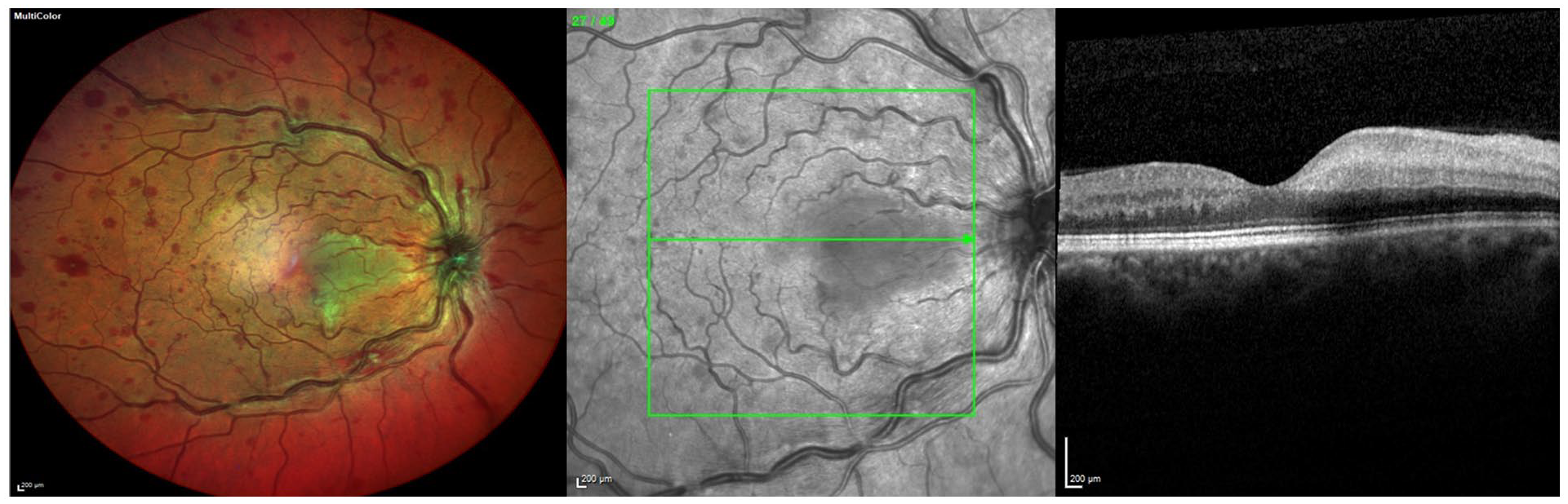
Posterior pole image and OCT of right eye at presentation.

OCT macular of the left eye.
Investigations
The patient was thoroughly investigated. A basic vascular occlusion screen including blood tests (Table 1) and magnetic resonance imaging (MRI) imaging of the head/orbits were carried out, and medical opinions were sought from the stroke team.
List of blood tests ordered.

In addition, carotid Doppler ultrasound and echocardiogram were performed.
The results of all investigations were unremarkable, with normal blood test results, no findings suggestive of an inflammatory or autoimmune vaso-occlusive disease, and no structural abnormalities identified on neuro-imaging.
On further enquiry at follow-up, the patient recalled that a week before the onset of ophthalmic symptoms she had suffered symptoms of a mild cough and fatigue with a low grade fever lasting a few days. A SARS-COV-2 antibody test subsequently confirmed that the patient had had exposure to the SARS-COV-2 virus.
Differential diagnosis
Patients with retinal artery occlusions are always thoroughly investigated for treatable underlying conditions. The differentials in a young patient include hypercoagulable states (such as polycythaemia, anti-phospholipid syndrome, etc.), cardiac abnormalities, autoimmune/inflammatory conditions, as well as systemic infectious causes.
As neither our investigations nor her history suggested any prior hypercoagulable state; we theorised that her COVID-19 illness which preceded this event was the most likely trigger.
Treatment and outcome
This patient was closely followed up and fortunately regained 6/6 vision in her affected right eye over a period of 5 months. On discharge examination there was no evidence of neovascularisation, with almost complete resolution of retinal haemorrhages and OCT showing classic thinning of affected inner retinal layers (Figure 3). As no treatable underlying condition had been identified, conservative management and active monitoring was all that was required in this case.

OCT macular of right eye at 5 months post presentation.
The patient did not develop any of the long-term COVID-19 sequelae, and at the time of discharge remained medically well and without any visual complaints.
Discussion and conclusion
Ocular complications associated with COVID-19 have been of interest in the past two years. COVID-19 is a condition that has been associated with thrombotic events and a hypercoagulable state.5,6 There have been a few reports of Central Retinal Artery Occlusion (CRAO) and other retinal manifestations such as paracentral acute middle maculopathy (PAMM) associated with COVID-19,1,7–10 but many of these were associated with severe COVID-19 infections. In our case, the patient suffered only very mild symptoms without being systemically unwell, yet still developed significant retinal pathology. This more insidious presentation is less commonly reported, and although incidental finding of this retinal appearance with COVID-19 infection has to be considered, there are other reports of similar scenarios in young patients. 2
Thankfully, our patient had a good visual recovery. Retinal artery occlusions can have devastating effects and impact on patients’ quality of life. Continued vigilance is required in making the correct diagnosis in these cases, and comprehensive investigations for underlying causes should be undertaken. This case adds to the body of evidence that COVID-19 and its systemic effects may stimulate enough of an inflammatory response and affect the coagulation system such that even otherwise healthy patients are at risk of unusual thrombotic disorders.
There is already great awareness of associations between COVID-19 and thromboembolic events in the media and medical community. We wish this case to add further to the understanding and knowledge that those presenting with significant visual symptoms, especially after recent exposure to COVID-19, should prompt an eye examination by a qualified optometrist or ophthalmologist, even if the symptoms initially seem mild. In atypical cases such as this one, it is important that enquiry about COVID symptoms or recent vaccination should be carried out, especially given that large numbers of fit and well young people are now being vaccinated (and over the coming months).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.