
Abstract
In industrial societies, work-related musculoskeletal disorders are common among workers, frequently resulting in recurrent injuries, work disability, and multiple compensation claims. The risk of idiopathic musculoskeletal injuries is thought to be more than twice the risk of any other health problem among workers in the health care sector. This risk is highly prevalent particularly among workers whose job involves frequent physical tasks, such as patient lifting and transfer. Workers with recurrent occupational injuries are likely to submit multiple work disability claims and progress to long-term disability. The objective of this study was to explore the influence of injury type and worker characteristics on multiple compensation claims, using workers’ compensation claims data. This retrospective study analyzed 11 years of secondary claims data for health care workers. Workers’ occupational groups were classified based on the nature of physical tasks associated with their jobs, and the nature of work injuries was categorized into non-musculoskeletal, and traumatic and idiopathic musculoskeletal injuries. The result shows that risk of multiple injury claims increased with age, and the odds were highest for older workers aged 55 to 64 (odds ratio [OR] = 3.5). A large proportion of those who made an injury claim made multiple claims that resulted in more lost time than single injury claims. The study conclusion is that the nature of injury and work tasks are probably more significant risk factors for multiple claims than worker characteristics.
Many workers who have been injured at work are at high risk for repeat work injuries and multiple compensation claims (Bohm, Gift, & Tao, 2009; Campolieti, 2001). It has been argued that first return to work does not always mean a successful end to workers’ disability and workers’ compensation claims (Baldwin & Butler, 2006; Butler, Johnson, & Baldwin, 1995). At least one third of injured workers are estimated to experience a new work injury after returning to work (Rossignol, Suissa, & Abenhaim, 1992; Ruseckaite & Collie, 2011). Sixty percent of workers who return to work after their initial injuries experience recurrent work-related injuries leading to work absences and multiple claims, and 40% are likely to become unemployed or apply for long-term disability (Butler et al., 1995). The risk of recurrent work injuries is believed to be higher in workers with work-related musculoskeletal disorders (WMSD; Duijn & Burdorf, 2008; Galizzi, 2013; Lipscomb, Cameron, & Silverstein, 2008). For instance, it has been estimated that about 10% of workers affected by spine disorders experience chronic health conditions (Garcy, Mayer, & Gatchel, 1996).
Previous studies have highlighted the need to consider multiple episodes of work injuries and workers’ compensation claims due to the serious consequences for the worker, employer, insurer, and society at large (Garcy et al., 1996; Lipscomb et al., 2008), which includes higher disability costs with frequent sick leaves, lost time which can affect productivity and output, wage replacement, increased demands on the health care system, rehabilitation, job retraining, and job modification to accommodate the needs of injured workers. Monitoring multiple episodes of work injuries and claim patterns is essential and should be a continuous process. As policies change, and new ergonomic designs and technology alter the ways work is performed, the nature and trends of work injuries are also impacted. In this changing environment, past knowledge of work mechanics and disability become ineffective for addressing current disability issues in the workplace. As such, studies such as this one that update knowledge of work disability are essential.
It is also important to understand the differences in characteristics of workers who experience recurrent work injuries and submit multiple compensation claims (Bohm et al., 2009; Campolieti, 2001). Several studies suggest that workers with histories of recurrent work injuries differ from those workers without recurrent injuries in demographic, psychosocial, and work history characteristics (Galizzi, 2013; Wasiak, Verma, Pransky, & Webster, 2004). Workers with recurrent work-related injuries are likely to have worse outcomes when they return to work, poorer health, and more work limitations than those workers with “sustained first return to work” (Bültmann et al., 2007). They are also more likely to progress to chronic illness or long-term disability (Pransky, Gatchel, Linton, & Loisel, 2005). It has also been reported that workers who have had more than one work-related injury have lower wages, earning losses, more pain, and limited job opportunities as they may be viewed as risky investments by employers, have less time to dedicate to improving their health, and experience lower life satisfaction and health outcomes overall (Galizzi, 2013; Galizzi & Zagorsky, 2009).
Work injuries also have a significant impact on the health care system itself. The relationship between disability, workers’ compensation, and health care costs has been studied extensively (Kuhnen, Burch, Shenolikar, & Joy, 2009; Ruseckaite & Collie, 2013; Wasiak, Kim, & Pransky, 2006). Some of the research has shown that recurrent work injuries are associated with longer work absence duration and higher costs than initial injuries (Lipscomb et al., 2008; Ruseckaite & Collie, 2011, 2013), making multiple work injuries a serious health and economic issue. In a study conducted in Victoria, Australia, researchers found total average cost for compensating workers with repeated injuries to be US$5,229 higher than workers with single claims (Ruseckaite & Collie, 2011).
Risk Factors for Recurrent Injuries and Multiple Claims
Many studies have looked at factors that constitute risks for second or multiple workplace injury claims (Cherry, Sithole, Beach, & Burstyn, 2010; Galizzi, 2013; Ruseckaite, Clay, & Collie, 2012). Findings on risk factors are diverse and complex; however, risk factors can be classified into the following categories: worker characteristics, workplace factors, industry characteristics, and nature of injury/disorder.
Worker characteristics are those factors associated with the physical, mental, and social aspects of the workers themselves. Several studies have looked at the relationship between worker characteristics such as gender, age, mental health, pain severity, duration of initial claim, job tenure, type of injury, education level, income, and recurrent work injury (Cherry, Burstyn, & Beach, 2012; Ruseckaite & Collie, 2011); however, the studies are not conclusive on the relative contributions of these worker factors to injury risks. Several studies have indicated that being male is a risk factor for multiple work injuries (Cherry et al., 2012; Lipscomb et al., 2008; Ruseckaite & Collie, 2013), but these findings were not consistent across all research studies. Age has also been identified as a risk factor for repeated work injuries. Younger workers, specifically those under the age of 35, were found to be more at risk for filing multiple claims (Cherry et al., 2010; Ruseckaite & Collie, 2011, 2013). This finding has been attributed to a lack of experience, high percentage of younger workers employed in high-risk occupations, and being employed in temporary or part-time work (Ruseckaite et al., 2012; Ruseckaite & Collie, 2013). Although younger workers may be at higher risk for multiple claims, older workers have poorer return to work outcomes (Turner, Franklin, & Turk, 2000) and longer work disability after both initial and recurrent injuries (Ruseckaite & Collie, 2013). Older workers with lower back pain were found to be at higher risk for filing multiple claims (Wasiak et al., 2004). The interaction between age and gender has also been found to impact risk of multiple claims. In a study by Cherry et al. (2010), the risk of men filing multiple claims decreased with age; however, filing multiple claims peaked between ages 35 and 44 for women. Workers with fewer years of service and lower incomes were also found to have more injuries than workers with greater tenure and higher pay (Cherry et al., 2010; Craig et al., 2013; Galizzi, 2013).
Workplace factors for multiple claims are related to the employer, facility, and work environment including occupation, job tasks, social support, organizational policies and practices, and scheduling (Cherry et al., 2010; Ruseckaite et al., 2012). Studies have reported a link between rates of multiple claims and workplace factors such as job accommodations provided to workers post first injury (Baldwin & Butler, 2006), quality and amount of safety training (Smith & Mustard, 2004), type of tasks performed (Lipscomb et al., 2008), work schedules (specifically nonstandard schedules involving long hours; Dembe, Delbos, Erickson, & Banks, 2007; Dembe, Erickson, Delbos, & Banks, 2005; Galizzi, 2013), and significant decline in safety (Wagstaff & Lie, 2011).
Industry characteristics (e.g., mining, manufacturing, construction and machining trades, and transportation) have been suggested in some studies to increase the risk of recurrent work injury and multiple claims (Cherry et al., 2010; Galizzi, 2013; Ruseckaite & Collie, 2011). Working in the manufacturing industry was found to have the highest risk for multiple claims, regardless of gender (Galizzi, 2013), suggesting that workplace factors could be more significant risks for multiple claims than individual worker characteristics (Cherry et al., 2010; Swaen, Van Amelsvoort, Bültmann, Slangen, & Kant, 2004). Greater risk for second injury claims has also been attributed to the size of the company; however, the connection between the two is also dependent on the type of industry and gender of workers. The study by Bena et al. (2006) found that for both genders, enterprises with three to 10 employees represented lower risk than smaller enterprises with only two workers, and the risk varied based on the interaction of gender and company size (Bena et al., 2006). Another study found that working for a larger employer increased the risk for a second claim (Cherry et al., 2010), but being employed in a high-risk industry was a more significant factor for recurrent injuries (Galizzi, 2013). These studies suggest that the risk of multiple or recurrent injuries and claims are higher in the two extremes of enterprises with very few employees (below three) and large numbers of employees (greater than 10). This finding is an area that needs further study to provide more clarity on how and why multiple injury claims vary by size of enterprise.
Nature of injury/disorder and recurrence has been linked in some studies, though findings are mostly inconclusive. Work-related musculoskeletal disorders, often involving lower back or upper extremities, or cumulative trauma disorders (CTD) are more likely to lead to multiple work-related injuries and work absences than other types of injuries (Baldwin & Butler, 2006; Ruseckaite & Collie, 2011; Wasiak et al., 2006). Other studies have implicated musculoskeletal injuries, surface wounds, and traumatic injuries (Cherry et al., 2010; Lipscomb et al., 2008) in recurrent and multiple claims. Bültmann et al. (2007) found that 38% of workers who experienced a WMSD had multiple injury-related work absences. In addition, 26% of workers who experienced a CTD of the upper extremities, 18% of those with low back pain, and 12% with fractures reported a second injury-related work absence (Baldwin & Butler, 2006).
Higher risk of repetitive injury has also been associated with specific health conditions such as stroke, impaired sight or hearing, and a history of mental illness (Cherry et al., 2012; Galizzi, 2013; Jansson, Stenbacka, Leifman, & Romelsjö, 2004). The study by Galizzi (2013) reported the relationship between severity of initial injury and risk of multiple claims, but Lipscomb and colleagues (2008) did not find such a link. However, multiple studies (Lipscomb et al., 2008; Wasiak et al., 2004) have shown that the length of time on work disability at initial injury is a risk factor for recurrent injury. The period between claims varied based on worker factors and nature of injury, indicating a complex interaction among the various factors (Cherry et al., 2010).
Approaches to Studying and Analyzing Recurrent Injuries
The definition of recurrent injury or claims varies significantly in the literature. Injury recurrence has been defined as “the filing of a new worker’s compensation claim” (Lipscomb et al., 2008, p. 833). However, many studies examining multiple claims defined recurrence as the re-opening of the initial claim, filing a new claim, or re-starting benefits (Gross & Battié, 2005). Ruseckaite and Collie (2013) defined recurrent claim as “a second or any subsequent claim of a worker during the study period, and it could have occurred for the same as an initial or a completely different reason” (p. 2). The approach to looking at multiple claims varies across studies due to the inconsistency in definition of recurrent injury. Some studies treat each claim as a separate event (Smith, Chen, Hogg-Johnson, Mustard, & Tompa, 2011; Wasiak et al., 2006); other studies focused on the relationship between initial and recurrent claims (Ruseckaite & Collie, 2011, 2013). The approach used by Lipscomb et al. (2008) differentiated between incidence and prevalence of injury, and reported injury recurrence in terms of “prevalence percent.”
Studies on recurrent work injuries are commonly based on workers’ compensation data (Bena et al., 2006; Cherry et al., 2010), and some have used indemnity payments to determine start and end date of a claim (Wasiak, 2006). The way workers’ compensation board data is reported complicates strictly identifying recurrent injuries or establishing the exact relationship between initial and subsequent claims (Evans, Mayer, & Gatchel, 2001); hence, the approach that treats a multiple claim as an injury unrelated to the initial injury (Smith et al., 2011; Wasiak et al., 2006) is particularly beneficial for studies using workers’ claims data. In addition to workers’ compensation databases, studies have used information from health care providers regarding treatment to identify recurrent injuries (Wasiak et al., 2006; Wasiak et al., 2004).
Another challenge with multiple claims studies is specifying the time gap necessary for a claim to be considered a new claim. In the study by Rossignol et al. (1992), each subsequent injury after the first injury was considered a new injury as long as one workday separated each claim. In another study, both recurrences in health care and work disability were used to establish whether a repeated claim had occurred (Wasiak et al., 2004). Recurrence in health care was defined as having a minimum of a 45- to 60-day gap in treatment, and recurrence in work disability was defined as having 1, 3, or 8 days if indemnity payments were used, indicating a period when the worker resumed job duties. A gap in indemnity payments of 3 days for work disability and a 45-day gap for treatment were used as an indication of recurrence (Wasiak et al., 2006). In the current study, the term multiple claims refers to any claims after the initial claim, which avoids the pitfall of determining a recurrent injury or claim from the Workers Compensation Board (WCB) data. Moreover, the number of cases identified as recurrent injuries in this WCB data set was too small for stratified analysis, similar to the approach used by Ruseckaite and Collie (2013), which considered both injuries related to earlier occurrence and those that were not related.
Compensation Board data provide useful information regarding risk factors for multiple claims, and support comparisons with studies that have used similar databases (Bena et al., 2006; Cherry et al., 2012; Cherry et al., 2010). Although several studies have examined recurrent injuries and illnesses in workers, studies that used workers’ compensation claims data to examine multiple claims are few (Cherry et al., 2010; Ruseckaite et al., 2012; Ruseckaite & Collie, 2011). In Canada, one study explored characteristics of workers who filed second claims using 1995 to December 2004 WCB data from Alberta (Cherry et al., 2010), but to the author’s knowledge, no previous study has reported risks of multiple claims or recurrent injuries in Manitoba workers. No specific study has been conducted in the context of health care workers, where WMSD are known to be high, and no studies have linked these claims to the physicality of work tasks. Continuously monitoring claim risk trends is essential because these issues are dynamic and influenced by several factors, many of which are localized or context specific. The purpose of this study was to understand the risk of multiple claims among workers in the health care sector by considering the nature of their injuries, and determine if the risks vary by worker characteristics and the physicality of their work tasks.
Method
This retrospective study used secondary data from WCB Manitoba collected between 2002 and 2012. The data for this study included workers’ compensation claims for two previous regional health authorities of Brandon and Central Manitoba, before the recent restructuring of the regional health authorities from 11 to five. A total of 2,223 claimants were included in the analysis. The data were anonymized to remove personal information that could identify participants in the data, such as address and phone number. Claimant’s identification (ID) was substituted by a dummy ID number for purposes of analysis. This process allowed findings to be reported in aggregated form.
Data Preparation and Analysis
Injury classification
Using the standardized z code on nature of injury, one pair of investigators independently classified injuries as musculoskeletal or non-musculoskeletal. The musculoskeletal injuries were further divided into traumatic and idiopathic types, in accordance with previous work-related musculoskeletal injury classification (Canadian Centre for Occupational Health and Safety, 2016; Kumar, 2001).
Occupational classification
Ninety-five different occupations were identified in the data. These occupations were organized into initial groups by the study team of four researchers, based on whether workers were clinical or non-clinical staff, and then by the nature of physical tasks they performed. The frequency and intimacy of interaction with patients were considered in grouping participants within the clinical staff category; the physical nature of work was the primary consideration for grouping non-clinical occupations. Groups were revised until consensus was reached among the four investigators, and in consultation with experts in health care research and services. The following seven occupational groups were created: (a) Administrative and Management Staff, (b) Clinical Staff: Frequent Patient Contact With High Physical Contact, (c) Clinical Staff: Frequent Patient Contact, but Less Physical Contact, (d) Clinical Staff: Infrequent Patient Contact, (e) Non-Clinical Staff: Frequent Patient Contact, (f) Technical and Support Staff With High Physical Task Demands, and (g) Technical and Support Staff With Low Physical Task Demands.
Statistical Analysis Software (SAS Version 9.4) was used to analyze data. The nature of injury was compared across participants’ ages, gender, marital status, work absence measured by lost time or no lost time, and whether workers had single or multiple injury claims by using frequencies and percentages. Univariate analysis using chi-square was used to determine the significance of the association between claims and worker characteristics. Logistic regression modeling was used to determine risk of multiple claims by nature of injury (traumatic, idiopathic, and non-WMSD), lost time injury, and specific worker characteristics.
Results
In this study, 2,223 workers filed a total of 8,016 claims within the 11-year period under study. Of the total claims, 29.4% were single claims and 66.4% were multiple claims (two to 10); 4.3% ranged from 11 to 24 claims, which represents an average of one or more claims per year. The majority of participants in this study were female (90.9%), possibly reflecting the population distribution of workers in the health care sector. A large number (n = 1,449, 65.2%) of the participants were in the direct patient-care occupation group, mostly dominated by nurses (average age was 41.98, SD = 11.1). Most of the claimants (72.7%) were 45 years of age and older, with higher numbers of injury claims occurring in this age category compared with younger workers. In the data set, 1.4% (n = 31) of the 2,223 claimants were identified as having injury recurrence; 98.6% (n = 2,192) were identified as having no injury recurrence. Injury recurrence (n = 31, 1.4%) was quite small for a stratified analysis and comparison, so the analysis focused on multiple claims rather than injury recurrence.
The percentage of female participants in this study was 90.9%; males constituted 9.1% of the sample. However, Table 1 shows some percentage differences in number of claims by female and male workers. Compared with males (10.1%), the percentage of females with single claims (89.9%) was less than their proportion in the population demonstrating that fewer females than expected made single claims. On the contrary, all the workers who filed the highest number of claims (24 times) were females. In the category of claimants who filed an average of at least one claim per year (11-24 times), 10 of the 95 claimants were males, representing 10.5% of the study sample, which proportionately is an over representation of the male population in these data. Overall, male workers were more likely to file single claims than their female counterparts.
Distribution of Injury Claims by Gender
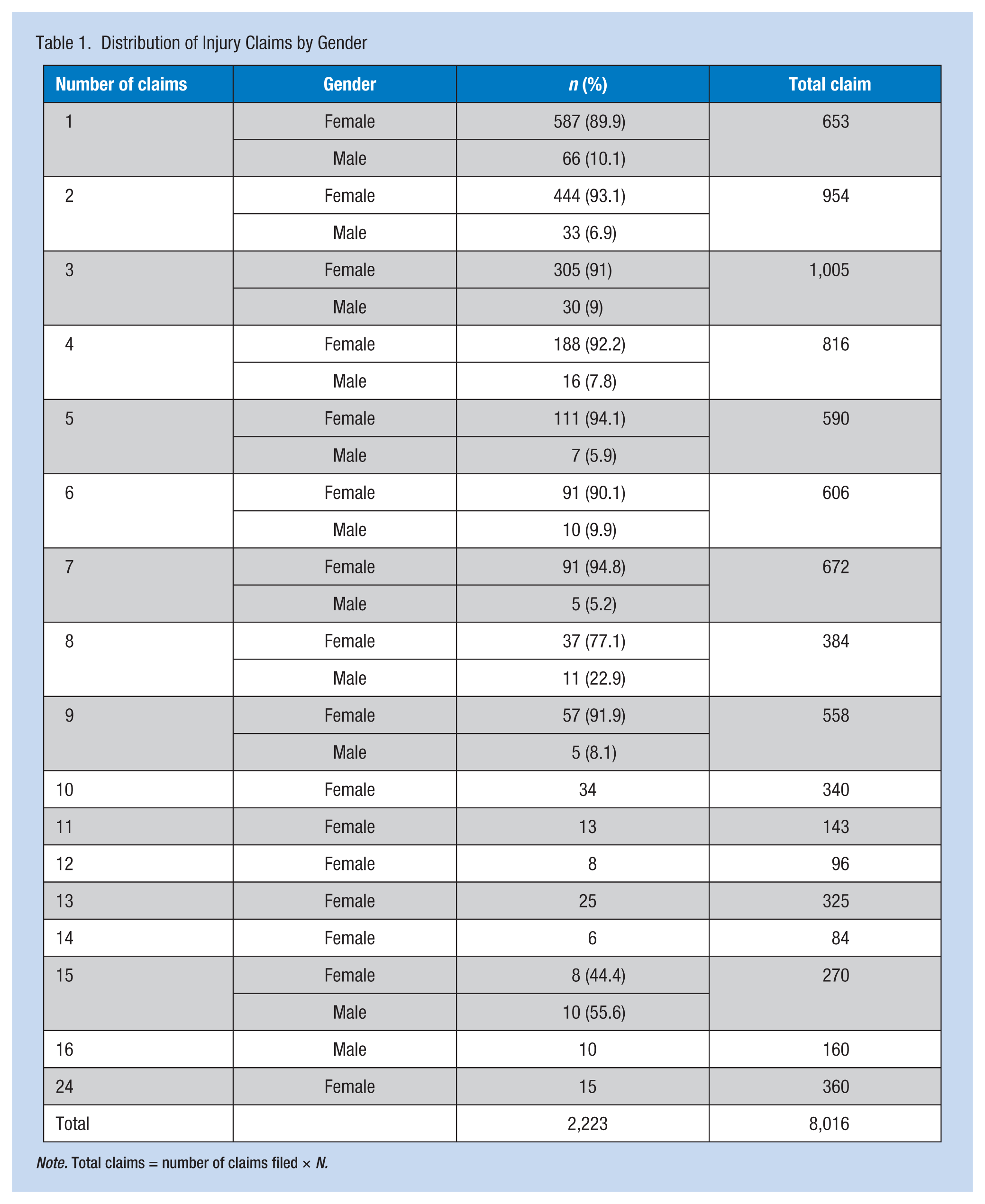
Note. Total claims = number of claims filed × N.
Table 2 presents information on nature of injury and its distribution by key participants’ characteristics. The work injuries were classified as idiopathic WMSD, traumatic WMSD, and non-WMSD. Most of the claims (74.6%) resulted from idiopathic WMSD; 11.6% and 13.8% resulted from traumatic and non-WMSD, respectively. Because idiopathic WMSD is the most common type of work injury in this study population, the following analysis focused on comparing the percentage distribution of this injury type across key participant characteristics. Among workers with a single injury claim, 70% were due to idiopathic injuries, but for workers with fewer multiple claims (two to 10) and more multiple claims (11 to 24), the percentages attributable to idiopathic injuries were 76.2% and 82.1%, respectively. This difference demonstrates that the nature of injury is a risk factor for multiple injury claims. Similarly, the majority of workers (78.9%) who lost time from work had idiopathic injuries. The number of females who reported idiopathic injuries (74.9%) was almost equivalent to the population with idiopathic injuries (74.6%), but less than the percentage of males (71.4%). However, more males (15.8%) than their proportion in the population (11.6%) had traumatic injuries, which suggest that males were more likely to have traumatic injuries and females were more likely to have idiopathic WMSD. With respect to age, the percentage of workers with idiopathic injuries was higher among younger workers than older workers. Some differences in the nature of injury were found across marital groups.
Description of Nature of Injury and Worker Characteristics
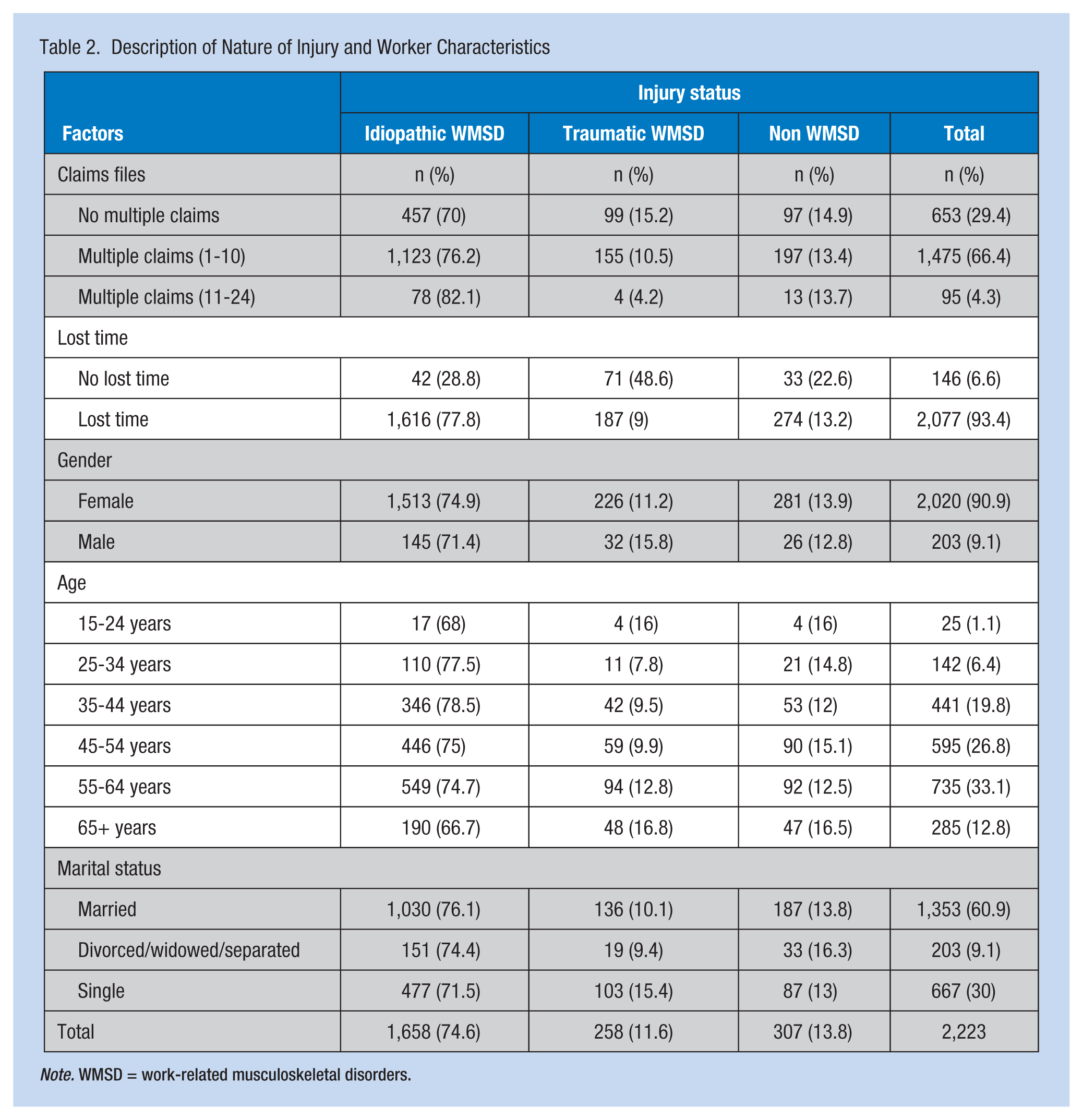
Note. WMSD = work-related musculoskeletal disorders.
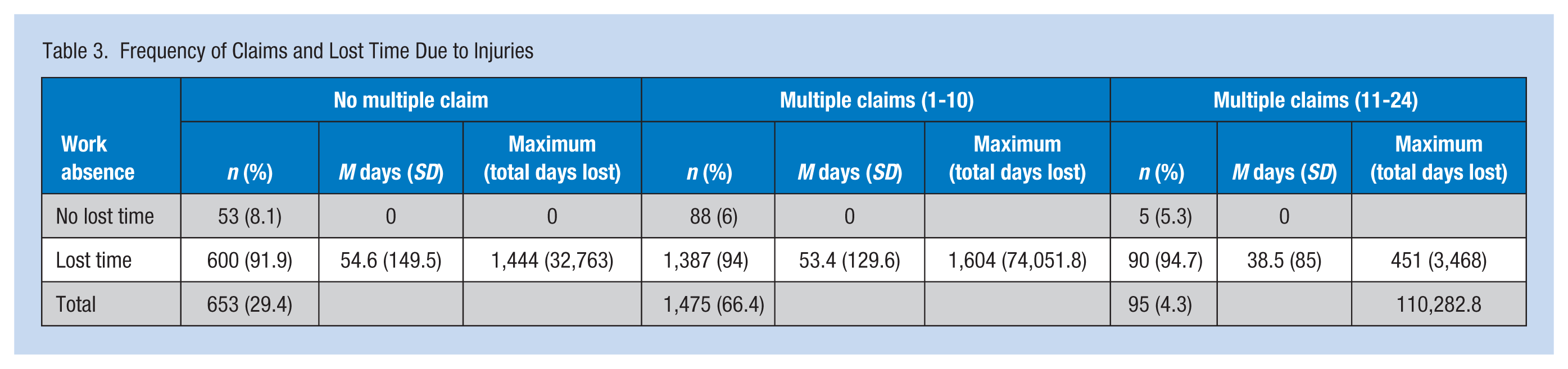
The majority of workers made multiple injury claims, and most of the claims led to lost time from work. Table 3 shows 66.4% of claimants made multiple claims ranging from 2 to 10 times, while 4.3% of the workers made 11 to 24 claims during the period. About 94% of the multiple injury claims resulted in lost time, compared with 91.9% of single injury claims. Overall, 70.7% of the claims cases were either due to recurrent or multiple injuries. A smaller proportion (29.4%) of the total claims were single claims. The average lost time days for single claims was approximately 55 days, with a total of 32,763 lost days. The total number of lost time days for multiple claims (2-24 times) was 77,519.8 days, accounting for 70.3% of total days lost during the period covered by this study. Ninety-five workers with 11 to 24 claims accumulated 3,468 lost time days.
Frequency of Claims and Lost Time Due to Injuries
Univariate Analysis
A univariate analysis using chi-square statistics compared the number of workers who had single claims with those workers who filed multiple claims by key worker factors. The results in Table 4 show significant differences in claims with respect to the nature of workers’ injuries (p = .0012), occupational group (p < .0001), age of workers (p < .0001), and marital status (p < .0001), but no significant difference was found with respect to gender. The lack of significant difference by gender may have been confounded by the small number of males in the data set, but could also be a reflection of the gender distribution by claims as shown in Table 1. The majority of workers made multiple claims; however, workers with idiopathic WMSD filed more multiple claims (72.4%) than other injury types. Both men and women filed more multiple than single claims, but the percentage of females with multiple claims was greater. In occupational groups, workers in the Clinical Staff Frequent and Intimate Patient Contact, and Technical and Support Staff Physical filed the highest number of multiple claims compared with other groups. The jobs of workers in these two categories were identified as having more physical tasks. Younger workers, age 15 to 24 years, filed the lowest percentage of multiple claims; the percentage of multiple claims increased with age. Workers who were either divorced, widowed, or separated had the highest percentage of multiple claims compared with other marital groups.
Differences in Multiple and Single Claims by Worker Factors
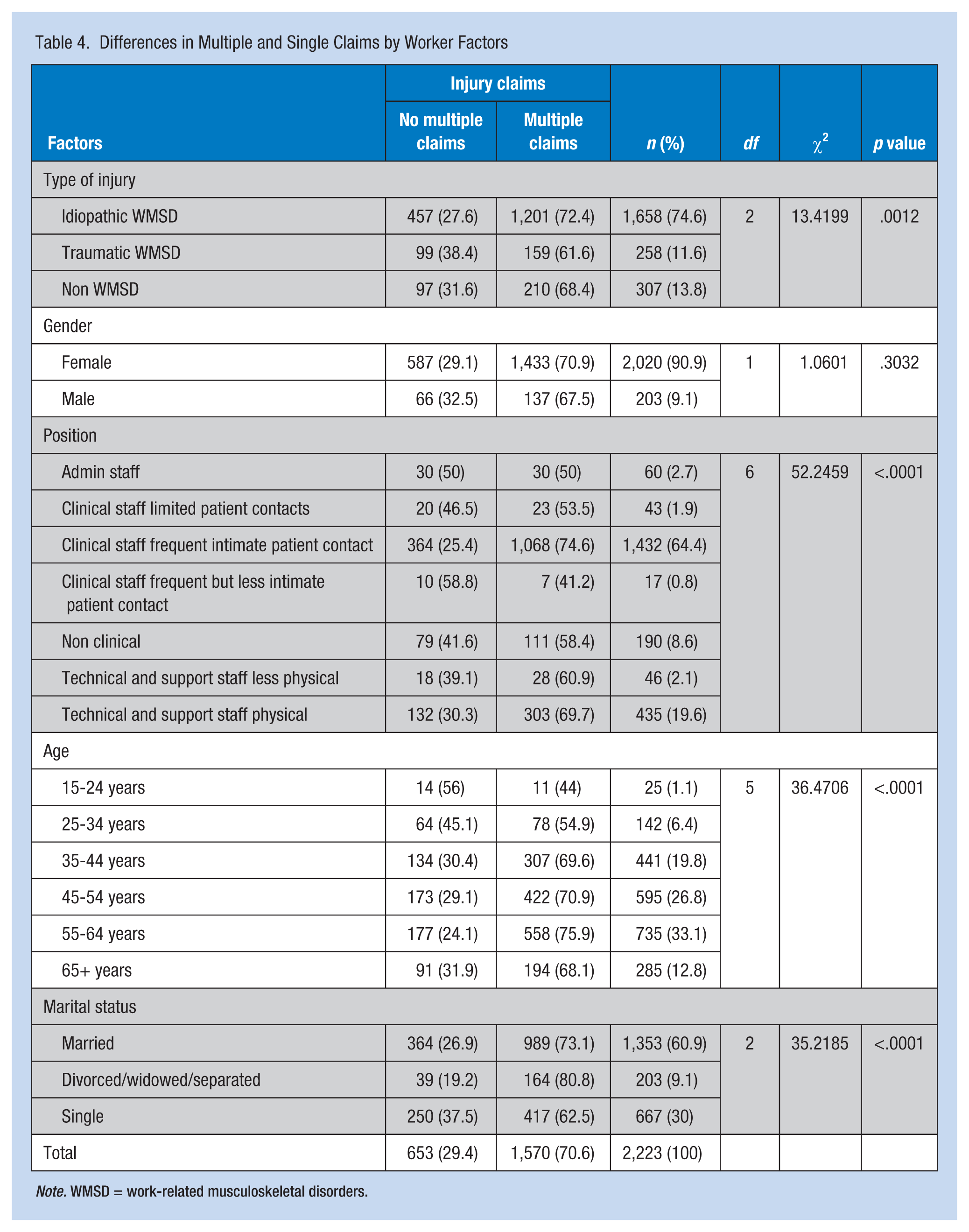
Note. WMSD = work-related musculoskeletal disorders.
Multivariate Analysis
The results of logistic regression in Table 5 show significant p values for the intercept, multiple claims (11 to 24 times), implying that the level was significant in the model. The following interpretation focuses on the odds ratios (OR) and the chi-square p values. Compared with workers who were single the odds of filing multiple claims was 2.2 times greater among workers who were divorced, widowed, or separated, and about 1½ times greater for married workers. The chi-square values for the two marital status levels were significant (p < .0001) in relation to the reference group (single marital status). The odds of having multiple injury claims were higher for all age groups compared with younger workers (15-24 years), although this finding was not significant for age group 25 to 34 years (OR = 1.407, confidence interval [CI] = [0.592, 3.349]). Overall, the odds for filing multiple claims increased with age. For occupational groups, the odds of multiple injury claims were higher for clinical staff with frequent and intimate physical contact with patients and for support staff whose jobs were associated with frequent physical tasks compared with support staff with less physical tasks. The common factor between these two high-risk groups is the high degree of physical tasks associated with their jobs. This finding supports the earlier premise that the physical nature of tasks presents a risk for injuries and multiple claims. Workers with lost time injuries were 1.3 times more likely to file multiple claims than those workers whose injuries did not lead to lost time.
Predictors of Risks of Multiple Claims
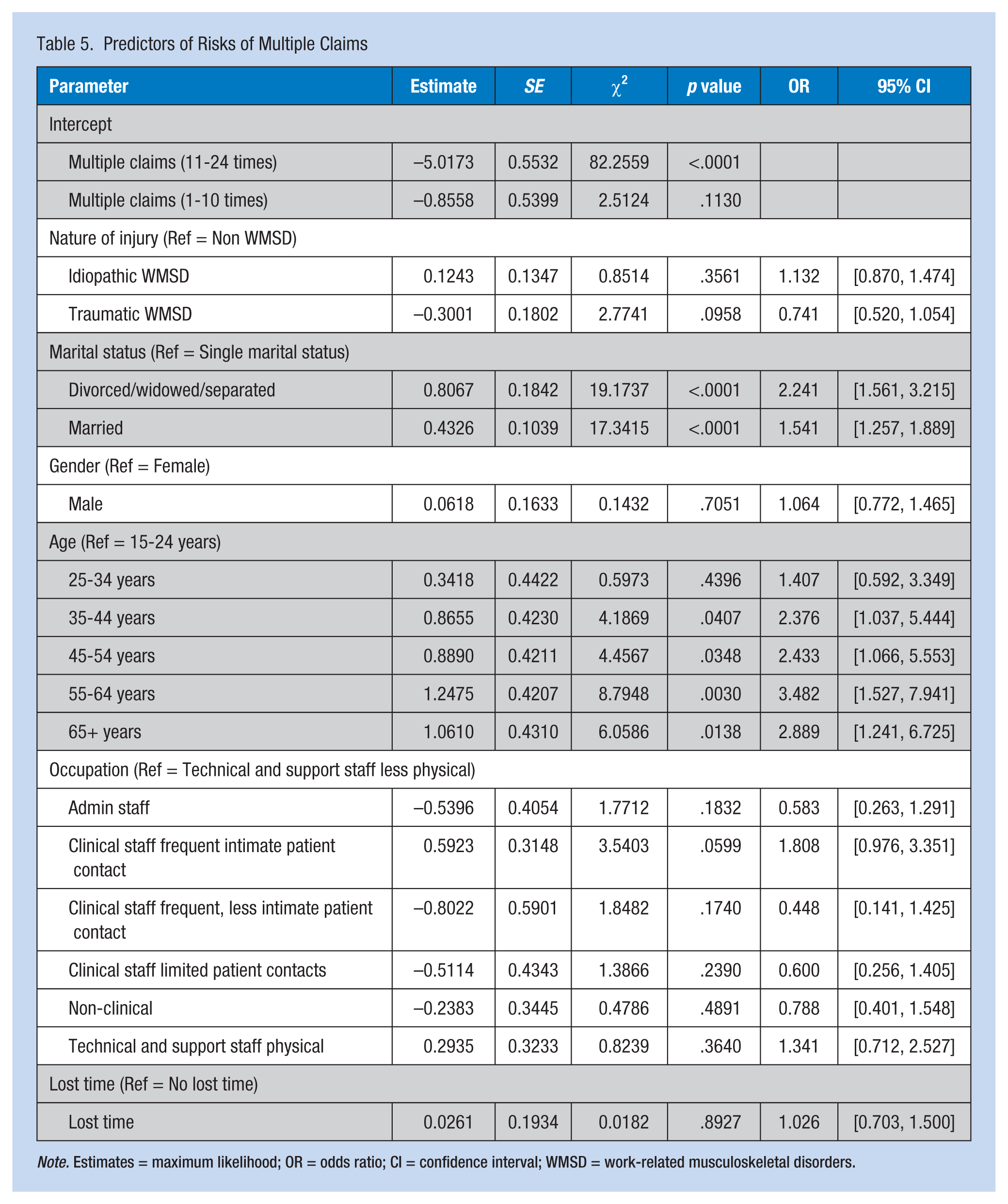
Note. Estimates = maximum likelihood; OR = odds ratio; CI = confidence interval; WMSD = work-related musculoskeletal disorders.
Table 6 displays the evidence of risk for multiple claims by comparing standardized risk estimates for selected factors. The cumulative logit model was developed using Fisher’s Scoring for Optimization Technique. The probabilities modeled are cumulated over the lower ordered values. The chi-square statistics were significant for all categories except gender and lost time. The risk of a worker filing multiple claims was assessed based on the nature of injury, marital status, gender, age, and whether the claimant had a lost time injury. The result of the standardized estimate showed the concomitant change in the risk of multiple claims resulting from one standard deviation increase in the explanatory factors of injury (having a WMSD), age, marital status (being married, divorced, or separated), gender (being male), and lost time injury. The standardized estimate indicated that although marital status may be the strongest predictor of multiple claims followed by age (p = .0001), gender and lost time contributed the least to understanding the risk of multiple claims.
Standardized and Non-Standardized Estimates of Multiple Injury Claims
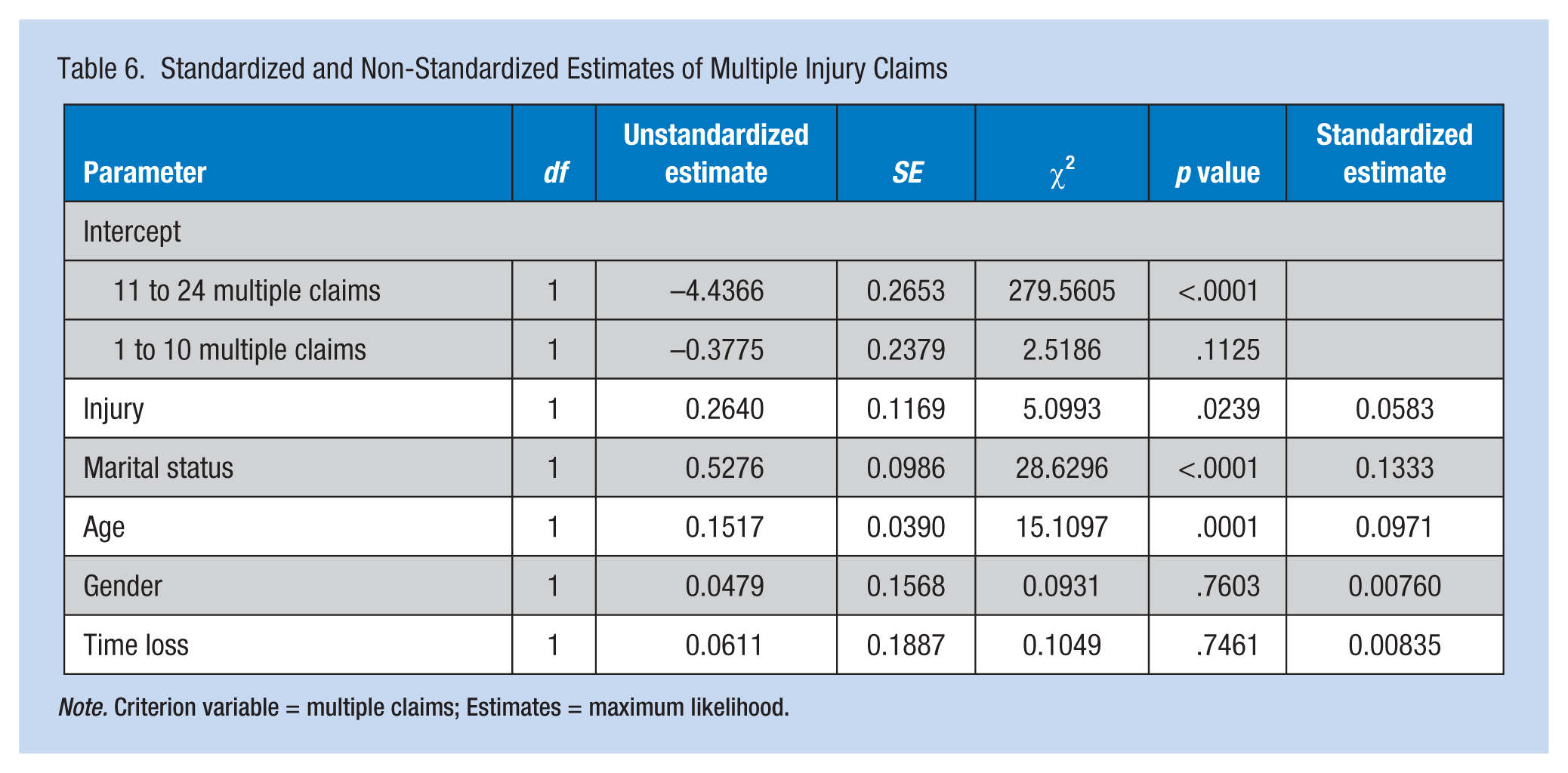
Note. Criterion variable = multiple claims; Estimates = maximum likelihood.
Discussion
Recurrent or multiple injury claims present a serious challenge to work disability management, the employer, workplace insurer, workers themselves, and workers’ families. Work disability is costly, in terms of number of days lost, workers’ health, and financial implications for employers and insurers. The majority of workers who filed a first claim in this study were more likely to file second or multiple injury claims. This finding is supported by previous studies (Bohm et al., 2009; Campolieti, 2001), which show that many workers who have initial work injuries are at high risk for repeat work injuries. In this study, 8,016 claims were made by 2,223 workers, a ratio of approximately four claims per worker. The total number of workdays lost due to work disability was 110,282.8, which is approximately 302.14 years of work time lost. The number of workdays lost due to single injury claims was slightly more than half (57.6%) of the days lost due to multiple claims.
In this study, the nature of work injuries was classified into idiopathic and traumatic WMSD and non-WMSD categories. Idiopathic WMSD most often led to lost time, compared with the other two injury categories. As such, studies of multiple or recurrent work injuries should pay particular attention to idiopathic types of musculoskeletal injuries. With respect to the nature of injuries, a clear difference was found between male and female workers. Male workers were likely to suffer traumatic injuries, and female workers were more likely to experience idiopathic WMSD and non-WMSD injuries. A significant difference was also found with respect to marital status; married workers were more likely to have idiopathic injuries than any other type of injury compared with those workers who were single, divorced, widowed, or separated. Overall, traumatic injuries were higher among workers who were single.
Knowledge of the nature of the injury is important for understanding the risk of recurrent or multiple injuries and injury claims among workers. Several previous studies have identified WMSD, often involving lower back or upper extremities, and traumatic injuries as major risks for recurrent work injuries, multiple claims, and work absences (Cherry et al., 2010; Lipscomb et al., 2008; Ruseckaite & Collie, 2011). In this study, 70.7% of the workers (n = 1,570) filed multiple injury claims; of these claims, 86.6% (n = 1,360) were due to WMSD. Similarly, previous studies (Baldwin & Butler, 2006; Ruseckaite & Collie, 2011) have also reported a greater risk for recurrent claims due to musculoskeletal injuries compared with other work-related injuries.
A number of worker characteristics related to recurrent or multiple work injuries have been identified in previous studies (Cherry et al., 2012; Campolieti, Goldenberg, & Hyatt, 2008; Harcombe et al., 2014). Confirmed in this study, the age and marital status of workers were identified as predictive of multiple injury claims. However, this study also strongly pointed to occupational characteristics related to the nature of tasks performed as significant risk factors for multiple work injuries and claims. Apart from age and marital status, the univariate analysis using chi-square showed a strong association between occupational group and multiple injury claims (p < .0001), with workers whose jobs involved more physical tasks (e.g., physical patient lifting and transfer) being disproportionately overrepresented in multiple claims. This evidence is strongly supported by the logistic regression model with higher odds of multiple claims in the two occupational groups with more physical job tasks. This evidence corroborates a previous study which points to industry factors increasing the risk of repeat injuries and claims (Ruseckaite & Collie, 2011), which by extension suggests that risk of recurrent injury probably lies more with work conditions than individual worker characteristics.
The majority of workers in this study were female (90.9%); however, it is unclear whether one can conclude that female workers are more likely to have work injuries and file compensation claims than male workers, or whether the gender distribution of injury claims reflects the population of male and female workers in the health care sector. Given what is known about gender characteristics of health care workers in this region, the high number of females is likely a reflection of the population. Some studies have reported that being male is a risk factor for multiple work injuries (Cherry et al., 2012; Lipscomb et al., 2008; Ruseckaite & Collie, 2013). However, this study did not find any significant difference between male and female workers in terms of multiple injuries and injury claims. It does appear that female workers were more likely to file multiple claims compared with male workers. A few female workers filed the highest number of multiple claims in this study. Results from this study also differ from Cherry et al. (2010), who reported “that men have a higher rate of claims than women, younger workers than those over 45 years” (S53). In fact, the multiple regression analysis did not find any significant difference between female and male workers with respect to multiple work injuries or multiple claims (p = .7190).
An analysis of age differences in injuries and multiple claims in this study also differed from some previous studies (Cherry et al., 2010; Ruseckaite & Collie, 2011, 2013). The multiple logistic regression revealed that the odds of filing multiple work injury claims were higher in older age groups (see Table 5) compared with younger workers, age 15 to 24 years, and suggests an increasing risk of multiple injury claims with increasing age of the worker. This difference could be attributed to the way data analysis was conducted in some studies. For example, Cherry et al. (2010) compared workers above 45 years of age and those below. This categorization of widely dispersed age groups can obscure or blur differences. The analysis by Wasiak and colleagues (2004) of workers with low back pain found older workers to be at higher risk for filing multiple claims, which is in agreement with the results of this study. The interaction between age and gender has been found to impact the risk of multiple claims. Cherry et al.’s (2010) analysis indicated that the risk of filing multiple claims by men decreased with age, but the risk peaked in the 35 to 44 age group for women. Controlling for possible confounders or interactions between factors, or a lower unit level of age analysis over a broad comparison of young and old, could decipher the differences. Other possible confounding factors of age differences in multiple injury claims have also been reported. Workers with fewer years of service and lower levels of income were found to have more injuries than workers with greater tenure and higher pay (Cherry et al., 2010; Galizzi, 2013; Ruseckaite & Collie, 2011). In this study, the proportion of workers with traumatic injuries declined with age, but peaked for the very young (15-24 years) and very old (65+ years); idiopathic injuries also varied among age groups.
Theoretical Interpretation of Multiple Injury Claims
Theoretically, several competing viewpoints have tried to explain why some workers file multiple injury claims and others do not. Some have argued that the nature of the injury could be a determining factor (Bültmann et al., 2007; Ruseckaite & Collie, 2011; Wasiak et al., 2006). This study identified the nature of injury as a significant risk factor for multiple work injury claims. Several studies, including this one, have focused on worker characteristics as risk factors for multiple injury claims. Workers with fewer years of service and lower levels of income were thought to have a higher probability of work injuries than workers with greater tenure and higher pay (Cherry et al., 2010; Craig et al., 2013; Galizzi, 2013). Younger workers (specifically those under the age of 35) were reported to have higher risk of filing multiple claims (Cherry et al., 2010; Ruseckaite & Collie, 2013), which was attributed to lack of experience, employment of high number of younger workers in high-risk occupations, or higher number of temporary or part-time workers (Ruseckaite & Collie, 2013; Ruseckaite et al., 2012). In this study, the percentage of workers with idiopathic injuries was found to be higher in younger age groups, suggesting a relationship between age, nature of work injury, and compensation claims.
Despite the various explanations for multiple injury claims, much is still unknown and researchers have not reached consensus based on study findings. An alternative approach to understanding why some workers file multiple injury claims and others do not could be found in the compensation system itself and how the system encourages or reinforces work disability behaviors such as injury claims (single or multiple) and sick leave claims. Vroom’s (1964) expectancy theory may provide insight into how and why particular categories of workers may be predisposed to file multiple injury claims.
Vroom’s expectancy theory has been widely applied in studies of work motivation (Latham & Ernst, 2006; Scaduto, Lindsay, & Chiaburu, 2008), a psychosocial factor. According to Vroom (1964), expectancy is “a momentary belief concerning the likelihood that a particular act will precede a particular outcome” (p. 17). The theory assumes that human beings are rational thinkers and that most human behaviors result from conscious choices among alternatives to maximize pleasure and minimize pain. The motivation to engage in a specific behavior (disability behaviors) is related to the expected outcome of rewards. If the outcome is expected to be adverse, rational beings likely avoid such behavior. Yamnill and McLean (2001) have described individual’s motivational effort to action as “a function of the value of the potential reward for the [individual] . . . and the perceived effort-reward probability (an expectancy)” (p. 198). Rewards to the individual might be intrinsic, intangible, or extrinsic, such as compensation pay or sick leave. From this perspective, worker motivation to engage in a specific behavior is linked to the expectations of reward. Workers’ satisfaction with specific rewards influences how they perceive the value of future rewards for the action, and as such influences the potential of undertaking the same action or behavior in the future. In this study, very few of the claims were identified in the data as recurrent injury cases; so, it is not clear if most of the multiple claims were new or due to recurrent injuries.
Limitation of This Study
Limitations of this study are common to studies that use secondary claims data, including the absence of specific variables such as years of work experience and work status (full time or part time). This study included only workers who had reported at least one work injury claim with the Manitoba WCB, so no comparison group of non-injured workers or those without injury claims was available. Underreporting of work injuries is prevalent in North America, particularly for psychological and social reasons (Ruseckaite & Collie, 2011), and this phenomenon could be true for the data used in this study. This study also does not take into account pre-injury worker or workplace factors.
Conclusion
Many workers who report occupational injuries suffer multiple injuries and file multiple claims. This problem is most common among workers with musculoskeletal-related injuries, which are prevalent among health care workers. Multiple injury claims increase disability costs due to sick leave, lost time, and disability costs such as wage replacement, health care, rehabilitation, job retraining, and worker replacement. Despite the high costs of recurrent work injuries to both workers and their employers, the understanding of risk factors that contribute to recurrent injuries is limited, and findings from current studies are often inconsistent. This study found that the nature of the injury (idiopathic or traumatic WMSD, and non-musculoskeletal), nature of physical tasks associated with an occupation, marital status, and age are associated with multiple injury claims. However, distinguishing among the risk factors for multiple claims is complex (Galizzi, 2013), given the interaction among worker and workplace factors. Further studies that incorporate more risk factors and consider their interactions could provide a better understanding of this phenomenon.
Applying Research to Practice
Workers in the healthcare sector, particularly those with high physical task demands, are disproportionately at high risk of experiencing idiopathic work-related musculoskeletal disorders (WMSDs) compared to traumatic WMSD and non-WMSD. Idiopathic WMSDs are linked to the mechanics of job performance, but can vary significantly with occupational groups, and sociodemographic characteristics. Workers who experience WMSD are also at higher risk of making multiple injury claims and incurring lost time injuries than other workers in the same sector. Multiple injury claims occur more in workers with idiopathic WMSD, and are the most significant drivers of disability cost. The implications of these results for disability management (particularly at the injury prevention stage) and facilitating sustained return to work are huge. Frequent and multiple injury claims could be due to the nature of occupational tasks or related to workers’ characteristics or a combination of factors; as such, injury case managers should always run a diagnostic analysis of the workplace before applying interventions.
Footnotes
Acknowledgements
The author wishes to acknowledge the contributions of Jayson Benneth, James Abbey, and Kyra McCubbin of the Master of Occupational Therapy program who worked with him during the data cleaning and grouping of occupational groups. The author is also thankful to Dr. Karen Schwartz of the Faculties of Education and Social Work, University of Manitoba, for providing editorial support. A special thank you to the Workers Compensation Board of Manitoba that gave permission to use their data for this study and also the Human Research Ethics Board of University of Manitoba for providing the ethical clearance for this research.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Nelson Ositadimma Oranye is an assistant professor in the Department of Occupational Therapy, University of Manitoba, where he coordinates and teaches Contemporary Issues in Work Disability at the MSc level. He has previously taught in universities in Nigeria and Malaysia. Dr. Oranye specializes in population health and is particularly interested in researching work-related disability issues.