
Abstract
A dearth of practical resources is available for evaluating ergonomic risk factors in dynamic health care work environments. Of particular need are tools for inspecting patient care environments for hazards. The goal of this study was to describe the development and application of an inspection tool and a process for identifying hazards inherent in the modifiable aspects of the physical environment to reduce injury risk to hospital workers. Through an iterative and participatory process, the tool and inspection process were developed with three purposes in mind: (a) create a framework for the inspection of physical work environments and physical conditions of work associated with injury risk (hazards), (b) document the physical conditions, and (c) provide feedback to decision makers. The tool and process were used by an ergonomics researcher on four patient care units as part of the Be Well, Work Well Total Worker Health® intervention. The resulting inspection process provided a structured method for recognizing hazards in the dynamic modifiable physical work environment and reporting both observations and recommendations to decision makers. The development and implementation of the inspection tool provided guidance to modify the physical work environment by implementing ergonomic solutions. The tool allowed the organization to plan and prioritize ergonomic hazard abatement (e.g. resource allocation and tracking trends). Within a Total Worker Health® framework, this tool can measure work practices which can then be used to inform organizational programs and policies within a health care setting.
Keywords
In dynamic hospital environments, the relationship between the physical demands of work, and workplace policies and practices and the occurrence of occupational injuries, especially work-related musculoskeletal disorders (WMSDs), are well documented (Burdorf, Koppelaar, & Evanoff, 2013; Hopcia, Dennerlein, Hashimoto, Orechia, & Sorensen, 2012; Koppelaar, Knibbe, Miedema, & Burdorf, 2013). Moreover, ergonomic practices aimed at reducing physical work demands appear to be associated with health care worker self-reported ergonomic factors (i.e., pain, injuries, ergonomics practices; Dennerlein et al., 2012). However, often not realized is the modification of the physical environment that can be controlled through ergonomic programs targeting the prevention of WMSDs (Caspi et al., 2013).
Hazard recognition and control are essential and fundamental elements of successful injury prevention programs (Cohen, 1997; National Institute for Occupational Safety and Health [NIOSH], 2008; Occupational Safety and Health [OSHA], 2012). These successful programs use hazard recognition tools and practices to identify and anticipate workplace hazards. In dynamic work settings (e.g., acute care hospitals), new hazards can materialize quickly as patient rooms are reconfigured to fit the arrival of new patients requiring a variety of equipment. Likewise, patient acuity and census levels can change daily, thereby changing the pace and physical demands of work. Hence, for such environments, regular assessments and control of hazards are often used through a continuous improvement safety model. Identification of modifiable ergonomic risk factors is essential due to the dynamic nature of these settings (Manuele, 2006).
Workplace inspections are a classic tool used to identify and anticipate hazards in the work environment, and implement corrective action. Higher inspection rates have been associated with more safety policy and regulation compliance and fewer injuries in the workplace (Hinze, Hallowell, & Baud, 2013; Mischke et al., 2013). This phenomenon is the result of long-term commitment to inspections and resulting feedback to workers and supervisors (Fang & Wu, 2013; Sparer, Herrick, & Dennerlein, 2015).
Reviewing available literature and online resources revealed a need for published methodologies and inspection tools with a practical focus on ergonomic factors in the physical work environment of healthcare facilities. Many existing tools are extensive, covering many factors within the work environment; because the tools are extremely detailed, complex, and time-consuming, only trained ergonomists can use them (Baumann, Holness, Norman, Idriss-Wheeler, & Boucher, 2012; Janowitz et al., 2006; OSHA, n.d.-b; Szeto et al., 2013). For example, the OSHA Hospital eTool addresses 15 areas of the hospital requiring extensive information regarding potential health and safety hazards and accompanying solutions (OSHA, n.d.-b). Although comprehensive, the tool requires significant time investment and the tool’s guidelines for reducing or eliminating hospital ergonomic risk factors may be too generic for users to identify specific potential hazards in the physical work environment and outline specific processes for mediating the hazards. Other processes have used either sophisticated musculoskeletal injury hazard assessments (e.g., Rapid Entire Body Assessment) or involved extensive training of staff; both of these approaches require advanced ergonomics training and experience (Baumann et al., 2012; Janowitz et al., 2006; Szeto et al., 2013).
The overall goal of this article was to document the development and description of an inspection tool and process that could be used to guide a portion of an intervention study implemented on acute care hospital patient care units. The authors intended to use a process that was comprehensive, and that the hospital occupational health team could easily use with minimal training. Tool questions must be easy to answer without an ergonomics background so that a hospital could use the tool without hiring a vendor or creating a position requiring extensive ergonomics training. Most hospital health and safety inspections are completed at the unit level so this tool is unit specific. Given the dynamic nature of hospitals, simpler tools that require less time and resource commitment are needed if continuous ergonomic hazard monitoring and resulting plans for potential abatement are to be completed.
Method
The need for a simpler ergonomic inspection tool based on empirical analyses arose from a larger proof-of-concept trial of a Total Worker Health® intervention as part of the Harvard T.H. Chan School of Public Health Center for Work, Health, and Wellbeing. This study was approved by the Harvard Chan School’s Institutional Review Board. The intervention was delivered to four patient care units in greater Boston area acute-care hospitals that participated in the Be Well, Work Well (BWWW) intervention. The proof-of-concept trial is described in full elsewhere (Sorensen et al., 2015). In brief, the BWWW intervention included consultation for nurse managers to implement changes on patient care units and educational programming for patient care staff to facilitate improvements in safety and health behaviors. The units participating in BWWW provided clinical care to patients formally admitted to medical, surgical, or intensive care units in the hospital. The four units that received the BWWW intervention were a medical intensive care unit (ICU), a thoracic surgery ICU, a medical oncology unit, and a neonatal ICU.
Ergonomics Inspection Tool and Process Development
The inspection tool was developed to provide feedback to the units (i.e., nurse directors and patient care workers) on ways the physical conditions of work could be modified to mediate ergonomic risk factors. Combining this purpose with the goal of identifying low-to-no-cost recommendations provided a useful and meaningful process for practitioners and researchers to address ergonomic factors related to the physical work environment on these select units. The tool was developed using an iterative process that included the following steps: conducting a general inspection, identifying a framework, drafting a tool, and piloting the inspection tool.
General inspection
First, a team of experts, including three ergonomic researchers, a registered nurse, and a hospital ergonomist conducted inspections of a wide variety of unit types in two major Boston hospitals. The entire team moved from unit to unit working together to gain a general understanding of the units, observe the physical and social organization of the units, look for visible hazards that could contribute to WMSDs and acute injuries, and engage available unit staff in impromptu, short, open-ended interviews about job-specific hazards experienced in their respective work environments. The open-ended interviews with unit staff were focused on understanding the type and scope of work on each type of unit. The 17 units observed included the following specialties: medical, cardiac, neonatal, and thoracic ICUs; orthopedics; labor and delivery; post anesthesia; general surgery; postpartum; urology; postoperative surgical; and endoscopy. All units were acute care, inpatient units. One unit was in a building constructed within the last 5 years while the other three were in older buildings. Observations were made about features of the physical environment that increased the risk for injury.
One of the key aspects of this approach to developing the tool was to focus on the modifiable physical environment. The purpose of this focus was to ensure that any observations could be modified (e.g., storage space was not assessed). In the urban Boston hospital setting, space is at a premium, and units often do not have adequate storage space. Tool development was focused on understanding the aspects of the physical environment that could be altered to make the unit work environment safer for patient care workers.
After the inspections were completed, the ergonomic researchers compiled a report outlining each of the units they observed including the type of care provided, observed and potential ergonomic hazards, and any other notes from the inspection or discussions with staff. The team of experts then distilled the report into a list of common issues and themes that recur from unit to unit. These themes became the basis for creating a tool applicable to all hospital units in an acute care inpatient facility.
The general inspections identified physical features common across all units and some features unique to unit type. As part of the inspection, the team also determined to what extent specific unit features were modifiable. An example of an identified modifiable feature was the placement of the bed in patient rooms. Oftentimes, the placement of beds can be changed, still allowing for access to the patient for care. Features considered fixed included aspects of the physical environment that could not be modified by hospital staff (e.g., flooring material). When aspects of these “fixed” features posed ergonomic risks, they were noted in the inspection tool along with recommendation for changes to be considered as part of future renovations.
Identifying a framework
The researchers used OSHAs Safety and Health Program Assessment Worksheet (Form 33) as a template for the tool framework (OSHA, n.d.-a). The Assessment Worksheet was designed to assess organizational policies and programs for OSHA, and was scored 0 through 5 (i.e., does not apply at all, somewhat, frequently, often, almost always, fully applies) in regard to how well each statement applied to the observation. Another beneficial aspect of the Assessment Worksheet was the inclusion of space for notes in each section. This structure allowed users to provide more than a simple “yes/no” answer and opportunities to track scores, and thus progress, over time.
Drafting a tool
After choosing the structure of the tool, the researchers assembled a list of the most important features and common themes of the modifiable physical work environment identified in the general inspection. Common features included nurses’ stations, storage areas, and patient rooms. Themes from the general inspection process were grouped into the common hazard categories of manual materials handling, safe patient handling, slips trips and falls, working with your hands over your head, and excessive bending and twisting while working (National Research Council & Institute of Medicine, 2001; Washington State Department of Labor and Industries, n.d.).
After the creation of a list of modifiable risk factors based on the inspections, the researchers sought input from the BWWW intervention working group responsible for designing and implementing the overall intervention. The working group included a registered nurse, multiple research assistants, intervention effectiveness researchers specializing in ergonomics and wellness initiatives, and multiple health professionals from the acute care hospital for which the tool was being designed. This team guided researcher efforts to define modifiable aspects of the physical unit work environment and to refine the tool to be more applicable to the acute care environment. The team made comments about and fine-tuned the original list of modifiable risk factors. Finally, the researchers asked staff from hospital occupational health to further refine the tool and align listed targets with hospital-wide initiatives. This step resulted in a draft of the final inspection tool, ready to be vetted and piloted within the hospital setting.
Piloting the inspection tool
The tool was used by a small team consisting of two ergonomic researchers and a staff member from the occupational health group to pilot the inspection process on two units in the hospital. These units were not selected for the BWWW intervention study and thus represented an ideal setting to understand and refine the tool and process prior to implementation as part of the intervention study. After the pilot studies, minor revisions (e.g., phrasing of statements and tool questions) were incorporated to enhance tool utility. Overall, no changes to the substantive content of the tool were made.
The Inspection Process
The inspection tool was used as part of a process of informing workers, managers, and researchers about WMSD risk factors in the physical work environment. The process involved several components including accessing and inspecting the unit, communicating immediate observations, compilation of the observations, review of inspection findings with occupational health staff, and communicating the observations back to the unit leadership and staff. These steps and processes were developed with the hospital occupational health staff. The researchers wanted to ensure that the process could be easily integrated into other health care environments with little to no interference with existing work flow, policies, and practices on the units.
Accessing and inspecting the unit
Access required planning and scheduling a convenient time for the inspection to occur. The individuals involved in the inspection process (Figure 1) included a member of the research team serving as the inspector as well as a combination of Nurse Director, Clinical Nursing Specialist, Resource Nurse, and assorted nurses and patient care assistants depending on staffing and availability on the particular unit during the inspection. Throughout the inspection, the tool was used to guide the inspector and document specific observations. The inspection lasted approximately 1 hour on each unit, providing ample time to observe the entire unit.

Flowchart of the inspection process including planning, meeting with occupational health, and final feedback to the units.
Communicating immediate observations
A key component of this process was the ability to communicate certain immediate observations to staff members. Oftentimes, this communication included the inspector answering questions and concerns posed by staff members encountered during the inspection. The inspector in this case was a member of the research team but inspectors in other settings would not need extensive ergonomic training to fulfill this role. Oftentimes, the immediate feedback consisted of identifying how to adjust equipment (i.e., office chairs or display monitors) or reminding staff that most equipment in patient rooms was on wheels (i.e., able to be maneuvered to provide better access to patients without added strain on workers). Providing immediate feedback was well received resulting in unit leadership and staff trusting the inspection processes and sometimes in immediate modifications that had been identified.
Review of inspection findings
Working with a staff member from occupational health familiar with in-house resources, the researchers developed a list of recommendations to address ergonomic-related issues in the work environment. The staff member aided the research team in focusing the list of observations to include only those observations that were considered modifiable and paired with a recommendation. All recommendations were designed to be actionable with a description of the recommendation accompanied by appropriate contact information (i.e., phone number and contact for the office chair vendor to repair broken chairs covered under warranty). This was a collaborative, in-person discussion that lasted approximately 30 minutes per unit.
Communicating findings with leadership and staff
Recommendations were then communicated with the unit’s Nurse Director via a report consisting of observations from the inspection and associated recommendations. This report was ideally communicated during an in-person meeting lasting between 15 and 30 minutes which allowed nurse directors to ask questions about the observations and recommendations. Unit leadership then disseminated results and action items to staff through staff meetings and email.
Results
The resulting inspection tool was comprised of two parts, one part for the inspection itself (Appendix A) and the other part to guide a short interview with unit nurse management (Appendix B). When combined, the two parts provided a complete overview of and a structured method for recognizing hazards in the modifiable physical environment.
The final inspection tool included three domains (housekeeping, awkward postures, and safe patient handling and mobilization) which addressed the fundamental hazards of manual materials handling, safe patient handling, slips trips and falls, working with your hands over your head, and excessive bending and twisting while working. The major component of housekeeping was cord, cable, and tubing management including placement of equipment carts. The “Awkward Postures” section in Appendix A focused on accessibility of materials in storage rooms, placement of equipment (i.e., sharps boxes within patient rooms), and computer workstations. The “Safe Patient Handling and Mobilization” section in Appendix A was of particular concern for the hospital. This section focused on ceiling lift and sling availability. Virtually all patient rooms in the hospital had ceiling lifts and thus this was an essential aspect to include in the process, evaluating compliance and aligning with hospital initiatives.
The research team generated a feedback and recommendations report, a simple, meaningful, actionable, two-column table (Figure 2). The left column included the final list of observations from the inspection and the right column included associated recommendations. Each recommendation included the name of an employee or department to contact along with a phone number or email address. If the recommendation could be accomplished without outside resources, the directions were explicit and thorough so the recommendation was truly actionable. If the recommendation required purchasing a product, then the recommendations included a website, company name, and approximate price. Wherever possible, pictures were added to increase the utility of the report and reduce confusion over products or observations. The report then contributed to further discussions with the nurse directors in subsequent management level BWWW intervention activities focusing on leadership development.
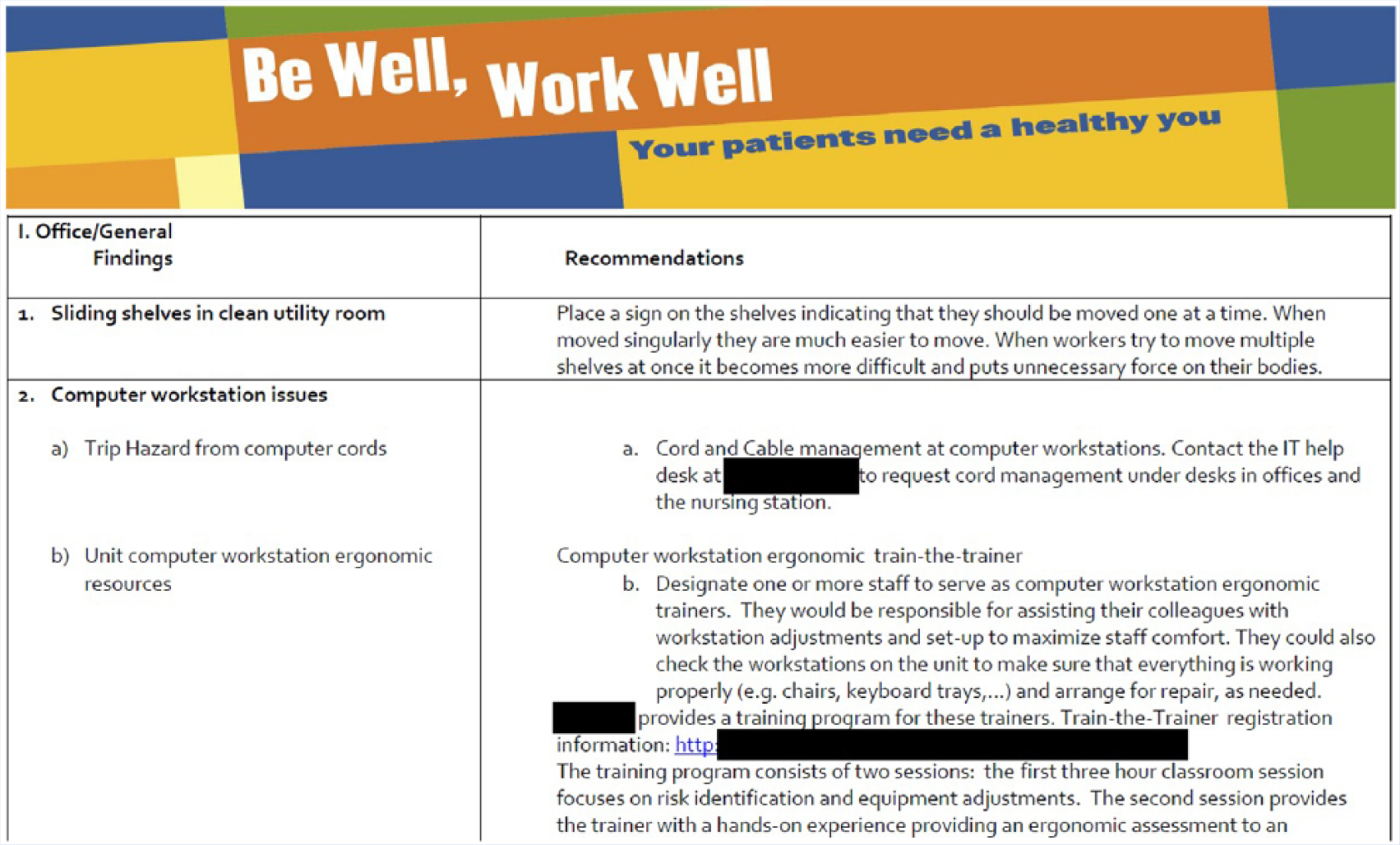
Snapshot of the inspection tool report for unit leadership.
Discussion
The overall goal of this article was to document the development and description of an inspection tool and process that could be used to guide an intervention study for acute care hospital patient care units. The tool could then be used in other patient care environments to evaluate and identify needed improvements in the modifiable physical environment.
The development and implementation of the ergonomic inspection tool showed that inspections of the modifiable physical work environment can be useful and productive. The process of inspection, part of an integrated intervention, was feasible and meaningful to both intervention efforts as well as to the units involved in the intervention. The researchers identified low-to-no-cost recommendations and even used internal resources to address many of the identified needs. One major finding of the study was the importance of involving internal personnel with organizational knowledge. Working closely with the hospital occupational health department, users quickly and efficiently identified resources across hospital departments to address needs.
This study has several limitations. First, the differences in work organization by unit prevented direct comparison across units. Units sometimes had distinctive patient acuity and work demands. For example, a worker in the neonatal ICU might assume static postures at the bedside frequently during a 12-hour shift. Although this observation could affect comparisons to other units without prolonged static postures (i.e., a thoracic ICU), the inspection tool was designed to examine an individual unit. A valuable strength of this tool is the ability to track unit observations longitudinally. Tracking inspections can determine unit compliance with and sustainability of recommendations made after an inspection.
Second, inspections were limited to a single day and time that worked well for the unit. As a result, the researchers may not have observed the unit on a typical day during a typical time. In addition, the conditions and practices on a given unit may have been significantly different on different shifts that were not observed during this inspection process, a common weakness of inspections in general and highlights the need for repeated evaluations both over time and over shifts. A constraint of any inspection process is the potential for the inspector to miss particular events, activities, and even staff depending on the day and time the inspection is scheduled. One way to address this issue is to increase the frequency with which inspections occur, which is especially important in dynamic work environments such as health care. Although access to the units was restricted during the study, the tool can be utilized as frequently as the organization desires to address this limitation.
The level of involvement by occupational health staff impacts the generalizability of this tool to other health care facilities. However, the tool was designed to capture modifiable aspects of the physical work environment in acute care hospital and the researchers do not expect that the physical work environment in other inpatient acute care hospitals would differ significantly from the study hospital. Thus, using this tool in an acute care inpatient environment will likely require only minor adaptations. The researchers recommend that a member of the occupational health department review and modify the content of the tool as needed prior to implementation to ensure that all tool statements align with the physical work environment.
One aspect of the hospital environment that is particularly difficult to quantify or overcome is the deeply engrained beliefs and attitudes surrounding environmental health and safety practices. Specifically, it is difficult for patient care staff to devote time and effort toward any activity other than those activities related to patient care (Sorensen et al., 2015). These beliefs can impede change to new unit policies and practices. In this study, it was difficult to address practices related to safe patient handling and mobilization, particularly the use of mechanical patient lifts.
This study did not use one of the more sophisticated musculoskeletal injury hazard assessment tools (e.g., Rapid Upper Limb Assessment [RULA], the Strain Index, or the NIOSH lifting equation) by design. The intervention was intended to be used by hospital occupational health personnel with minimal training.
This study also has several strengths. First and foremost, the inspection protocol was designed to be meaningful and useful for all units. The researchers incorporated the needs and wants of the organization wherever possible. The occupational health department was involved in nearly every step of the process, from design and process development through the evaluation and feedback steps. The researchers wanted to ensure that unit needs were met and they were focusing on issues that would benefit the hospital.
Another strength of this process was its ability to track progress over time. Basing the inspection tool on the OSHA Form 33, the researchers assigned a “score” to each unit. These metrics tracked trends for individual units over time with an inspection protocol that included additional inspections at regular intervals.
An effort was made to ensure that unit management received actionable and meaningful feedback so that it was easy to respond to inspection findings, given the busy schedules of nurse directors and limited unit resources. Most recommendations required in-house services from other departments; often the units were unaware of these services. The researchers were not able to contact the units to determine whether any of the recommendations were followed or how well they were received.
Although intended as a component of the BWWW intervention and designed for use by an occupational health and safety professional, others could potentially use the tool in the health care community. The physical environment is often overlooked when assessing overall quality and occupational health criteria for both patient and worker safety. This tool and process could be integrated into routine systematic assessments of nursing units by nurses and other clinicians.
Dynamic work environments like health care benefit from strong organizational programs, policies, and practices surrounding hazard identification. Total Worker Health® is a useful framework for designing interventions in dynamic work environments like health care. The tool and process developed in this study can measure work practices and inform organizational programs and policies within a health care setting. The ergonomic inspection tool can identify areas for improvement in existing patient care environments to reduce the likelihood of musculoskeletal pain and injury.
Implications for Practice
Given the dynamic nature of hospitals, simpler tools that require less time and resources are needed for continuous monitoring of the physical work environment and planning hazard abatement. This process and tool identified areas for improvement in existing patient care environments to reduce the likelihood of work-related musculoskeletal pain and injury. The tool provides workplace intervention programs with data to effectively prioritize resource allocation and intervention efforts and identify low-to-no-cost recommendations to address ergonomic hazards in the physical work environment. Occupational health practitioners, ergonomists, or insurance companies working for or consulting with acute care hospitals can use this tool and process to inspect the modifiable physical work environment, identify hazards, provide recommendations, and track trends and progress over time.
Applying Research to Practice
Hospitals require simpler tools for continuous monitoring of the physical work environment and planning hazard abatement to address ergonomics hazards. The dynamic nature of the hospital environment requires tools needing less time and resource commitment. This tool and process can be used by occupational health practitioners working for or consulting with acute care hospitals to inspect the modifiable physical work environment, identify hazards, provide recommendations, and track trends and progress over time.
Footnotes
Appendix A
Appendix B
Acknowledgements
This study would not have been accomplished without the participation of Partners HealthCare System and leadership from Dennis Colling, Sree Chaguturu, and Kurt Westerman. The authors would like to thank Partners Occupational Health Services including Marlene Freeley and Dean Hashimoto for their guidance, as well as Elizabeth Taylor, Elizabeth Tucker O’Day, and Terry Snyder. Additionally, we wish to thank Evan McEwing and Julie Theron, Project Directors.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institute for Occupational Safety and Health (U19 OH008861) for the Harvard School of Public Health Center for Work, Health and Well-being and in part by the National Institute for Occupational Safety and Health Education and Research Center at Harvard University (T42 OH008416).
Author Biographies
Michael P. Grant is an industrial hygienist with the National Institute for Occupational Safety and Health where he performs health hazard evaluations. His research has involved designing, implementing, and evaluating integrated workplace interventions through the Center for Work, Health and Wellbeing at the Harvard T.H. Chan School of Public Health.
Cassandra A. Okechukwu investigates how work and working conditions influence health and health behaviors. Her occupational health studies have included epidemiological as well as intervention research.
Karen Hopcia is the associate director for Shared Services, Budget and Data Analysis, Partners HealthCare Occupational Health Services. She is also an investigator working with the Center for Work, Health and Wellbeing at the Harvard T.H. Chan School of Public Health.
Glorian Sorensen is professor of social and behavioral sciences at the Harvard T.H. Chan School of Public Health, director for the Center for Work, Health and Wellbeing, and was the Principal Investigator for the Be Well–Work Well Study, for which this study was conducted.
Jack T. Dennerlein is professor of physical therapy, movement, and rehabilitation science at Northeastern University and co-principal investigator for the Center for Work, Health and Wellbeing at the Harvard T.H. Chan School of Public Health. His research aims to prevent work-related injuries and musculoskeletal disorders through multiple research approaches that in general examine how the design of the environment, both built and organizational, affects worker health outcomes.