
Abstract
Work-related musculoskeletal disorders (WMSDs) persist as the leading occupational injury, accounting for nearly half of nurses’ total occupational injuries. Musculoskeletal pain is a known cause of sleep disruption, and individuals with WMSDs that interfere with sleep often report more pain. Evening chronotype has been associated with poor sleep among nurses. However, the associations among chronotype, sleep, and WMSDs are still unclear, and were explored in the present study. A cross-sectional survey was administered to 397 nurses, with 47.4% reporting WMSDs. Robust Poisson regression modeling suggested that evening type (PR = 1.32, p < .05), prolonged sleep onset latency (PR = 1.37, p < .05), and using sleep-promoting substances (PR = 1.35, p < .01) were associated with increased risk of WMSDs among nurses, after adjusting for shift work, regular exercise, body mass index, and other covariates. This study suggests that well-designed evidence-based nonpharmacological interventions to improve sleep may reduce the risk of WMSDs among nurses.
Work-related musculoskeletal disorders (WMSDs) persist as the leading occupational injury in the United States. In 2014, WMSDs accounted for 32% of all occupational injury cases, with an incidence rate of 33.8 cases per 10,000 full-time employees, resulting in over 360,000 days away from work and long-term worker pain and disability (Bureau of Labor Statistics [BLS], U.S. Department of Labor, 2014). It is estimated that the direct expenditures in health care costs and indirect expenditures in lost wages resulting from WMSDs were US$849 billion, or 7.7% of the national gross domestic product (GDP) in the United States (United States Bone and Joint Decade, 2008).
Health care is one of the largest sectors in the U.S. economy, with 14.3 million employees (BLS, U.S. Department of Labor, 2010-11). Among more than 300 U.S. industries, the hospital industry ranks as the third most expensive due to occupational injuries and illnesses, with nursing personnel reporting the highest costs (Waehrer, Leigh, & Miller, 2005). Hospital nurses are particularly vulnerable to low back pain and other WMSDs due to patient handling responsibilities. In 2015, more than 10,000 registered nurses (RNs) sustained WMSDs that resulted in missed workdays, with an incidence rate of 48% in private sector, state, and local government facilities (BLS, U.S. Department of Labor, 2016). Hospital nurses also provide care 24 hours each day; as a result, they are at risk for impaired sleep quantity and quality, sleep disturbances, and long-term sleep deficiency (Caruso, 2014; Geiger-Brown et al., 2012). In addition to irregular and long work hours, many other factors may contribute to nurses’ poor sleep (e.g., physical and psychosocial work strain; Geiger-Brown & Lipscomb, 2010; Zhang, Punnett, PhillipsMcEnany, & Gore, 2016). These work stressors may conflict with family responsibilities (e.g., child care and elder care) further contributing to poor sleep (Jacobsen et al., 2014; Zhang et al., 2016). A bidirectional relationship may exist between poor sleep and WMSDs (Koffel et al., 2016). Compromised or disrupted sleep is a known consequence of chronic pain (Kelly, Blake, Power, O’Keeffe, & Fullen, 2011), and individuals who have experienced WMSDs that interfere with sleep are reported to perceive pain as more intense and have worse musculoskeletal outcomes (Schrimpf et al., 2015; Takahashi, Matsudaira, & Shimazu, 2015). This cycle of impaired sleep and WMSDs, and the comorbidities associated with them, are critical issues for nurses considering the impact of work on their own safety and health, and how that in turn may impact the quality of care they provide to patients. Although these associations provide a focus for workplace safety and health interventions, the specific aspects of sleep (e.g., duration, onset latency, disturbance, timing, and/or medication use) associated with WMSDs are still unclear and warrant further investigation.
Chronotype refers to individual preferences regarding sleep and waking times, and is hypothesized to be a behavioral manifestation of underlying circadian rhythms. Morningness (early sleep timing; most active and alert in the morning) and eveningness (late sleep timing; most active and alert during the late evening/night) are the two extremes of chronotype. Chronotype has been increasingly recognized as significantly contributing to shift work adaptation or maladaptation, impacting workers’ ability to garner sufficient sleep and resulting in negative health and safety outcomes when sufficient sleep is not achieved (Gamble et al., 2011). Previous studies have reported that evening type, compared with morning type, is associated with poorer sleep quality (Yazdi, Sadeghniiat-Haghighi, Javadi, & Rikhtegar, 2014), and greater prevalence of shift work sleep disorders (Asaoka et al., 2013) among nurses. Jankowski (2013) reported that evening type individuals showed more sensitivity to pain than morning type individuals in a small group (n = 31) of healthy men. However, whether chronotype is associated with WMSDs has not been well studied, especially in shift workers.
In a related issue, although previous studies have reported that regular exercise and normal body weight are associated with less risk of chronic pain (Holth, Werpen, Zwart, & Hagen, 2008; Nilsen, Holtermann, & Mork, 2011), maintenance of a healthy weight and active lifestyle is problematic for nurses. Miller, Alpert, and Cross (2008) surveyed nearly 5,000 nurses from six U.S. states and reported the average body mass index (BMI) was 27.2 and almost 54% of respondents were overweight or obese. Nurses also face unique challenges (e.g., shift work) that negatively impact engaging in active lifestyles; nurses have more difficulty maintaining physical fitness. Albert, Butler, and Sorrell (2014) reported that 54% of nurses were active but at an insufficient level and 16% were inactive. Lack of regular exercise and overweight/obesity among nurses may potentially increase their risk of developing WMSDs. Therefore, these factors must be taken into consideration when exploring WMSDs among nurses. The objective of this study was to explore associations among hospital nurses’ chronotype, sleep characteristics, and WMSDs, after adjustment for shift work, regular exercise, BMI, and other sociodemographic factors.
Method
This study used cross-sectional data collected in March 2015 from a sample of 397 RNs and licensed practical nurses (LPNs) at a 430-bed, independent, not-for-profit community hospital in the northeast United States. A nonprobability convenience sampling method was used to recruit study participants. All RNs and LPNs over 18 years of age and working full-time, part-time, or per-diem at the hospital were eligible to participate.
Instruments
Dependent variable
Work-related musculoskeletal disorders were assessed by the severity of pain in six body regions (i.e., low back, shoulder, neck, wrist/forearm, knee, and ankle/feet) during the past week. Each region was rated on a 5-point Likert-type scale (1 = none; 2 = mild; 3 = moderate; 4 = severe; and 5 = extreme). Work-related musculoskeletal disorders were positive for participants reporting a moderate, severe, or extreme pain severity (≥3) in any body region (Zhang et al., 2016).
Independent variables
Sleep characteristics were assessed in five domains: sleep duration, onset latency (i.e., the length of time it takes to fall asleep after attempting to sleep), disturbances, number of episodes per day, and use of sleep-promoting substances (i.e., prescription, over-the-counter, and herbal medications, or alcohol to aid sleep). Sleep duration and onset latency were derived from the Pittsburgh Sleep Quality Index (PSQI; Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). Sleep duration was dichotomized as more than 6 hours or less than or equal to 6 hours per day (“short sleep duration”; Luckhaupt, Tak, & Calvert, 2010; Qiu, Gelaye, Fida, & Williams, 2012). Sleep onset latency was dichotomized as less than 30 minutes or more than or equal to 30 minutes. Sleep disturbances were assessed with the PROMIS Sleep Disturbance Short Form (SD-SF; Lanting, Saffer, Koehle, & Iverson, 2013), an 8-item scale to assess the severity of sleep disturbances among individuals age 18 and older. Each item was rated on a 5-point Likert-type scale (1 = never; 2 = rarely; 3 = sometimes; 4 = often; and 5 = always), with a range in total raw score from 8 to 40 with higher scores indicating greater severity of sleep disturbances. A T-score was calculated from the total raw score with a range of 28.9 to 76.5 based on the instrument scoring manual. A T-score of 60 or more indicates moderate to severe sleep disturbances. The Cronbach’s alpha, a measure of reliability, for this study sample was .9. Sleep episodes per day were assigned to one of three categories: all at one time, at two different times during the day, and at three or more different times; the data were dichotomized as all at one time or at two or more times. Use of sleep-promoting substances was assessed in five categories: not during the past week, 1 to 2 times, 3 to 4 times, and 5 or more times in the past week; the data were dichotomized as yes or no.
Chronotype was measured with the modified final question from the Morningness-Eveningness Questionnaire (Horne & Östberg, 1976). Chronotype was categorized as morning, intermediate, or evening type by self-description.
Covariates
The survey collected information on nurses’ sociodemographic characteristics, including age, gender, and race. Lifestyle factors included BMI and exercise. Body mass index was calculated from self-reported weight and height, expressed as weight/height2, and categorized as normal (<25.0 kg/m2), overweight (25-29.9 kg/m2), or obese (≥30 kg/m2). Exercise was measured in five categories (1 = none; 2 = less than once per week; 3 = between 1 and 2 times per week; 4 = 3 times per week; and 5 = more than 3 times per week). Regular exercise was defined as “exercise three or more times per week (for at least 20-minutes per session to work up a sweat)” (Resnick & Jenkins, 2000).
Work schedule was defined as the primary work schedule at this hospital and categorized as 8-hour day, 8-hour evening, 8-hour night, 12-hour day, 12-hour evening (i.e., 9:00 a.m.-9:00 p.m., 11:00 a.m.-11:00 p.m., and 12:00 p.m.-12:00 a.m.), and 12-hour night shifts. This hospital typically provides permanent shift schedules for employees.
Data Collection
A study recruitment flyer was posted at each nursing unit in the hospital 2 weeks before the onsite survey collection. Surveys were distributed and collected by the research team over 5 days at the Annual Nurse Skill Days, mandatory for all nurses, in March 2015. The study purpose and procedure, and potential benefits and risks, were explained to the participants in person, and they were asked to complete the survey onsite. Participants were reassured that their employers would not receive any identifying information, and that participating or not participating in the study would not affect their work status. Participants received compensation of US$5 for completing the survey. The study was approved by the Institutional Review Boards at the hospital and the University of Massachusetts Lowell (No. 2015-001).
Data Analysis
All analyses were conducted using SPSS software 22.0.0 release on a Windows 7 operating system. Work-related musculoskeltal disorders were first examined by sociodemographics (age, gender, and race), lifestyle (BMI and regular exercise), and shift work to identify possible confounders. Associations among chronotype, sleep characteristics, and WMSDs were examined using the chi-square test. Because the prevalence of WMSDs in the study participants was 47.4%, Poisson regression modeling with robust variance estimate was more conservative and accurate than logistic regression modeling, and therefore was used to calculate prevalence ratios among groups and investigate potential confounding (Burros & Hirakata, 2003). Multivariate modeling to identify factors associated with WMSDs was adjusted for sociodemographics, lifestyle, and shift work. Two-tailed significance level was set a priori at p < .05.
Results
Descriptive and Bivariate Analyses
A total of 397 RNs and LPNs completed the survey, primarily middle-aged women (Table 1). The survey response rate was 36% of the total nurse population in the hospital. More than half (55.6%) of the participants were overweight or obese, and 56.9% reported not regularly exercising (Table 1). Nearly half of the participants reported short sleep duration (≤6 hours/day), or a prolonged sleep onset latency (≥30 minutes). One third of the participants reported sleep disturbances, with 11.4% reporting moderate to severe sleep disturbances. Pain was reported in the following body regions: low back (63.0%), shoulder (42.4%), neck (50.6%), wrist/forearm (24.2%), knee (35.0%), and ankle/feet (39.3%). Nearly half of the respondents (47.4%) reported moderate, severe, or extreme musculoskeletal pain in one or more body regions, and 16.8% reported moderate, severe, or extreme musculoskeletal pain in three or more body regions (Table 1).
Sociodemographics, Sleep Characteristics, and WMSDs Among Nurses (N = 397)
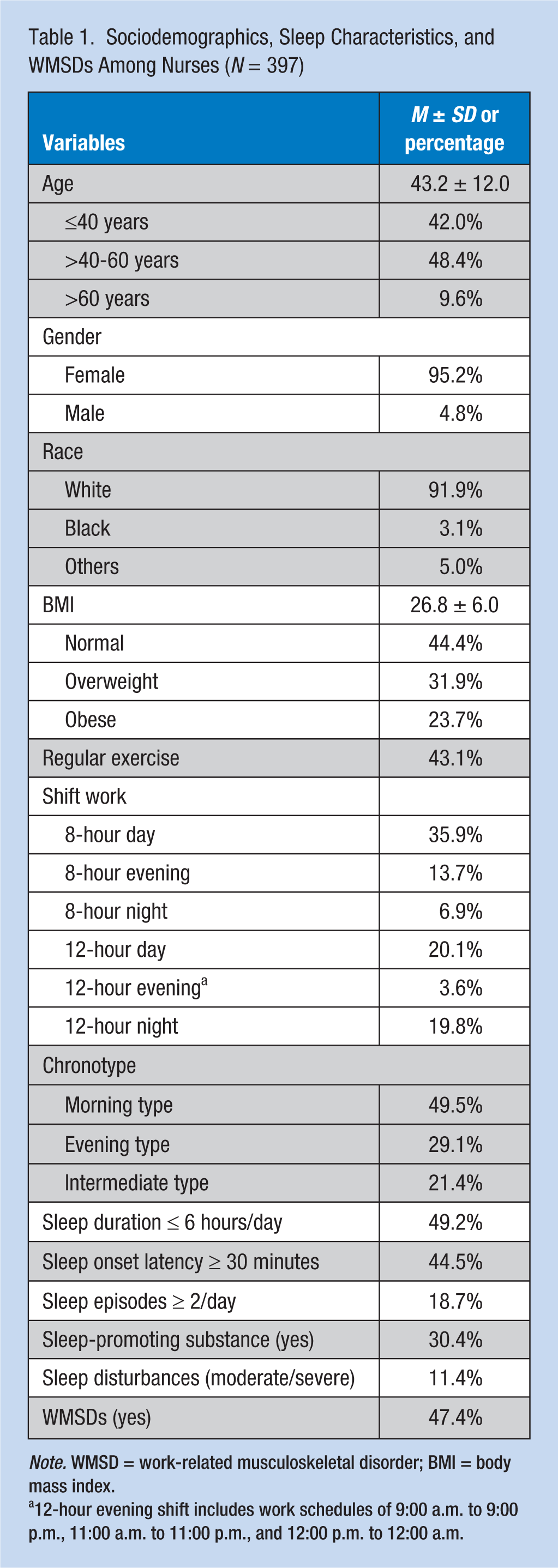
Note. WMSD = work-related musculoskeletal disorder; BMI = body mass index.
12-hour evening shift includes work schedules of 9:00 a.m. to 9:00 p.m., 11:00 a.m. to 11:00 p.m., and 12:00 p.m. to 12:00 a.m.
Cross-tabulation analysis using the chi-square test suggested that WMSDs were associated with evening type (χ2 = 9.1, p = .01), moderate to severe sleep disturbances (χ2 = 4.83, p < .05), sleep onset latency of more than or equal to 30 minutes (χ2 = 9.9, p < .01), using sleep-promoting substances (χ2 = 11.1, p < .01), and being overweight or obese (χ2 = 17.0, p < .01).
Multivariate Analyses
Multivariate robust Poisson regressions indicated that evening type (PR = 1.32, p < .05), sleep onset latency of more than or equal to 30 minutes (PR = 1.37, p < .05), and using sleep-promoting substances (PR = 1.35, p < .01) were associated with increased risks of WMSDs, after adjusting for age, gender, race, BMI, regular exercise, shift work, and other sleep characteristics (Table 2). Moderate to severe sleep disturbances, short sleep duration (≤6 hours/day), and more than or equal to two sleep episodes per day were not associated with WMSDs after adjusting for covariates. Overweight and obesity contributed to an increased risk of WMSDs (Table 2).
Multivariate Poisson Regression Models for Associations Among Chronotype, Sleep Characteristics, and WMSDs Among Nurses
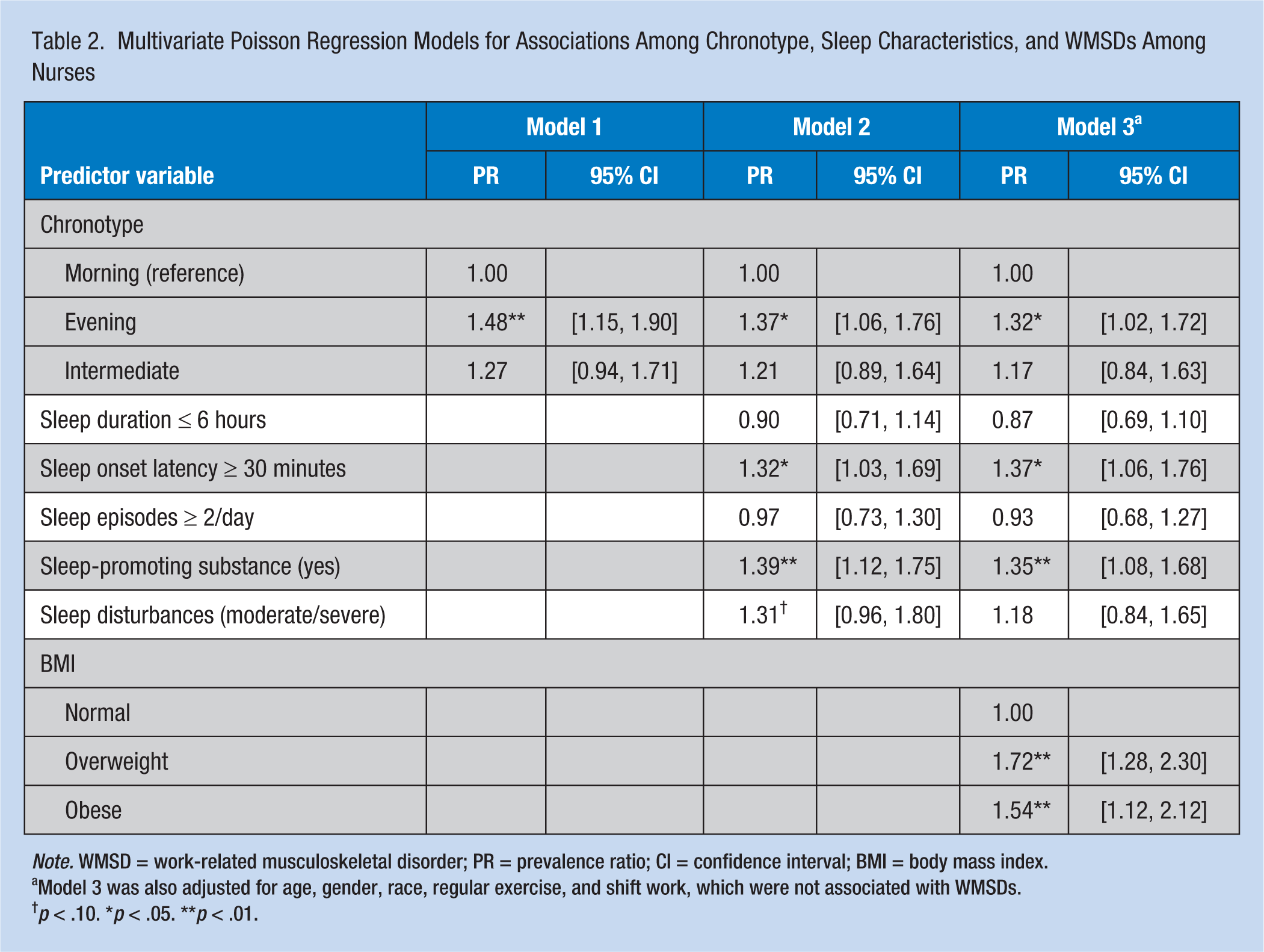
Note. WMSD = work-related musculoskeletal disorder; PR = prevalence ratio; CI = confidence interval; BMI = body mass index.
Model 3 was also adjusted for age, gender, race, regular exercise, and shift work, which were not associated with WMSDs.
p < .10. *p < .05. **p < .01.
Discussion
In this study of nearly 400 hospital nurses, a high prevalence of WMSDs and sleep problems (i.e., short sleep duration, long sleep onset latency, more than one sleep episode per day, sleep disturbances, and use of sleep-promoting substance) was reported. Similar to previous studies, the reported prevalence of WMSDs in nurses was greatest in the lower back, followed by the neck and shoulders (Davis & Kotowski, 2015). The reported short sleep duration (49.2%) among nurses in this study was greater than for all workers (30%) from the National Health Interview Survey (Luckhaupt et al., 2010) and for nurses (30%) from the U.S. National Nurses’ Health Study (Patel et al., 2004). These generally high rates of sleep problems among nurses are of critical concern because insufficient sleep is well-demonstrated to be a threat to the safety and health of workers, and for nurses it likely impacts the quality of care delivery and patient safety.
In addition to the economic costs of nurses’ long-term disability resulting from low back pain and other WMSDs, associations have been reported between sleep problems and WMSDs with intention to turnover among nurses (Fochsen, Josephson, Hagberg, Toomingas, & Lagerström, 2006; Kudo et al., 2006). Nationally, the turnover rates for bedside nurses are estimated to range from 8.8% to 37%, with an average turnover rate of 17.2% in 2015 (NSI Nursing Solutions, Inc., 2016). The cost estimates for each bedside nurse turnover range from US$37,700 to US$58,400, resulting in an average hospital losing US$5.2 million to US$8.1 million in 2015 (NSI Nursing Solutions, Inc., 2016). The replacement costs for nurse turnover can be twice a nurse’s annual salary (NSI Nursing Solutions, Inc., 2016), resulting in significant losses for health care facilities. Although these costs should inform hospital administrators, these losses should also point to ways in which interventions may reduce nurse turnover by addressing sleep and musculoskeletal issues.
More nurses in this study reported being morning types (49.5%) than evening (29.1%) or intermediate types (21.4%). In this study, evening type was significantly associated with an increased risk of WMSDs among the nurse respondents. This finding is similar to previous studies that reported higher risks for a range of health problems among evening type individuals (Merikanto et al., 2012; Merikanto, Lahti, Kronholm, et al., 2013; Merikanto, Lahti, Puolijoki, et al., 2013). Merikanto et al. (2014) reported that compared to morning types, evening types are at higher risk of articular and spinal diseases, especially related to backache, after adjusting for multiple covariates. Another study reported that evening chronotypes were more affected by perceived stress, memory failures, fatigue, depression, and fibromyalgia syndrome than morning chronotypes (Kantermann, Theadom, Roenneberg, & Cropley, 2012). Thus, evening type seems to predispose individuals to a wide range of health problems, including WMSDs.
In this study, sleep onset latency of 30 minutes or more was associated with a 32% increased risk of WMSDs. Similarly, those nurses who reported using sleep-promoting substances had a 39% increased risk of WMSDs compared with those nurses who did not report using any sleep-promoting substance. No significant associations between short sleep duration, multiple sleep episodes each day, or moderate to severe sleep disturbances (borderline significance disappeared after adjusting for covariates) with WMSDs were reported. The associations between specific characteristics of sleep and risk of WMSDs have not been well studied. However, in general, predictors of poor sleep seem to be associated with chronic pain. Finan, Goodin, and Smith (2014) summarized evidence from 2005 to 2014 and suggested that sleep impairments strongly and reliably predict new incidents and exacerbations of chronic pain. Buxton et al. (2012) reported significant associations of sleep deficiency with pain, functional limitation, and workplace interference among hospital health care workers. Mork et al. (2013) described dose-dependent associations between sleep problems and risk of pain in the low back and neck/shoulders from a national study in Norway. Future studies of the associations between different characteristics of sleep (with consistent and reliable measures of sleep duration and quality) and WMSDs among nurses are needed for the development of targeted evidence-based interventions.
Even though this study found associations among nurses’ chronotype, some features of sleep, and WMSDs, the causal relationships (if any) cannot be addressed based on these associations. One possible explanation is that evening chronotype and/or specific sleep problems induce a state of low-level systemic inflammation that contributes to sensitizing the nociceptive system, causing more intense perceptions of musculoskeletal pain (Mork et al., 2013). Future studies are warranted to navigate the mechanism of these associations.
The prevalence of overweight and obesity (55.6%) among nurses in this study is similar to the prevalence of these characteristics reported in previous studies (Han, Trinkoff, Storr, & Geiger-Brown, 2011; Miller et al., 2008). In this study, over half of the nurses reported lack of regular exercise. Consistent with Mork et al. (2013) and Nilsen et al. (2011), this study found that overweight and obesity were associated with increased risk of WMSDs. However, in contrast to Holth et al. (2008), Mork et al. (2013), and Nilsen et al. (2011), this study did not find an association between regular exercise and risk of WMSDs. Future studies with larger sample sizes are needed to examine whether regular exercise or overweight/obesity modifies the associations among chronotype, sleep characteristics, and WMSDs.
Strengths and Limitations
This study has several limitations. Although the study avoids some possible organizational confounders because all nurses were employed by a single not-for-profit hospital, the generalizability of the findings may be limited as a result. The response rate of the study was 36%, which may have caused some selection bias. Another study using a more nationally representative random sample would improve the generalizability of the findings. The lack of a standard full-scale measurement of chronotype may have biased the study results. However, the single question has been shown in previous studies to strongly correlate with the score from the overall 19-question Morningness-Eveningness Questionnaire. Future studies should use standard instruments to measure chronotype to verify any association with WMSDs. The cross-sectional design of this study did not allow the researchers to draw causal inferences. Future analyses of longitudinal data are needed to verify study findings. Finally, although the researchers adjusted for multiple factors (e.g., sociodemographics, lifestyle, and shift work) related to sleep or WMSDs, the authors cannot exclude the possibility of residual confounding. For example, the authors did not include information on other factors that may affect nurses’ sleep, such as physical and psychosocial work strain, work–family conflict, and working other paid jobs, which is common among health care workers in the region. The strengths of this study include the comprehensive range of sleep characteristics and location of WMSDs assessed, and the consideration of potential confounders in the data analyses.
Implications for Occupational Health Practice
Occupational health nurses promote health behaviors and outcomes of nurses by assessing work-related hazards and providing tailored education and interventions to reduce work-related hazards. The findings of this study deserve special attention from occupational health nurses, because both sleep and WMSDs are major health and safety concerns for nurses. Work-related musculoskeletal disorders are responsible for over one third of all workers’ compensation claims in hospitals (Zurich, 2015). In addition, nurses have the most contact with and provide most of the direct care to patients in hospitals, so their ability to be present and functioning at a high level are essential to ensure patient safety and high quality care.
Beside workplace interventions designed specifically for WMSDs prevention and intervention, this study suggests that nonpharmacological interventions that improve nurses’ sleep may reduce their risks for WMSDs. Occupational health nurses should involve both the organization and nurses in reducing sleep problems to mitigate WMSDs. Sleep has been a long-standing problem for nurses and is closely associated with irregular and long work hours (Caruso, 2014; Geiger-Brown et al., 2012), and a diversity of physical and psychosocial work stressors, such as physical and psychological strain (Winwood & Lushington, 2006) and work-family conflict (Berkman et al., 2015). Effective workplace interventions are needed to reduce nurses’ sleep problems and improve their musculoskeletal health, such as limiting rotating and 12-hour shifts; structuring work schedules to allow sufficient time for sleep between shifts; increasing staffing to reduce workload; and establishing Employee Assistance Programs (EAP) to support nurses who experience high psychological strain and/or have difficulties balancing work and family life. Previous studies also suggested that the health effect of nonstandard shift work is less severe if it is chosen by employees (Buessing, 1996); therefore, increasing nurses’ control over their work shifts may reduce the negative health and safety consequences that result from demanding work schedules.
Occupational health nurses could also initiate workplace education or training programs to address healthy sleep practices among nurses, for example, providing education on healthy sleep hygiene, coping strategies related to shift work and work stress, lifestyle changes to adapt to shift work and promote sleep, as well as complementary approaches to sleep promotion, such as relaxation techniques, meditation, and yoga (Sarris & Byrne, 2011).
Conclusion
This quantitative cross-sectional study found that evening chronotype, prolonged sleep onset latency, and regular use of sleep-promoting substances were associated with increased risks of WMSDs among hospital nurses. With the high personnel turnover in the health care sector, the increased demand on nurses, and the focus on quality of care, more effort is needed to promote the safety and well-being of nurses. This study suggests that well-designed evidence-based nonpharmacological interventions that improve sleep, whether from the organization or the individual, may reduce the risk of WMSDs among nurses.
Applying Research to Practice
This study provides innovative information about chronotype, sleep characteristics, and WMSDs among hospital nurses, who have the most contact with and provide most of the direct care to patients. Both sleep and musculoskeletal health of nurses are essential to ensure patient safety and high quality care. Findings from this study can provide evidence for identifying work-related hazards, providing tailored education and interventions to address health risks, and promoting sleep and musculoskeletal health of nurses. This study can assist occupational health nurses in developing and implementing effective workplace education and training programs to address healthy sleep practices, improve coping with shift work and work stress, and promote use of nonpharmacological strategies for sleep promotion to reduce the risk of sleep impairments and WMSDs among nurses.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a University of Massachusetts Lowell Faculty Start-up Award to Y.Z. J.F.D. is supported in part by National Institute of Health (NIH) Grant R01 AG044416.
Author Biographies
Yuan Zhang is assistant professor of nursing at the University of Massachusetts Lowell. Her research focuses on the broader effect of work environment on sleep quality, physical and mental health, and turnover of health care workers, as well as workplace participatory interventions to improve employee health and safety.
Jeanne F. Duffy is an associate professor of medicine at Harvard Medical School and a neuroscientist at Brigham and Women’s Hospital. Her research focuses on understanding individual differences in sleep timing, duration, quality, and response to sleep loss and exploring ways to improve sleep so as to reduce the risk of accidents, errors, and adverse health outcomes.
Elizabeth Ronan de Castillero is a medical-surgical nurse educator at Lowell General Hospital. She has been actively involved in several research studies related to nurses’ shift work, working conditions, sleep quality, and safety and health outcomes.
Kefang Wang is dean and professor of nursing at Shandong University in China. Her research focuses on nurses’ health, especially nurses’ health behaviors and related risk factors, as well as tailored interventions to improve nurses’ overall health and well-being.