
Abstract
Low back pain (LBP) remains one of the most common and challenging musculoskeletal conditions encountered by health care professionals and is a leading cause of absenteeism. Clinical guidelines are often considered best evidence in health care. The aim of this critical review was to assess the quality and recommendations of LBP guidelines using the Appraisal of Guidelines Research and Evaluation (AGREE) instrument. Electronic databases were used to identify LBP guidelines published between 2000 and 2015. Nine guidelines were selected for review from a total of 17. Only five guidelines effectively addressed the AGREE scoring. On the basis of the appraisal and domain scores, only four guidelines were strongly recommended. Improved translation of research evidence from guidelines to clinical practice is needed.
Low back pain (LBP) is one of the most common and challenging musculoskeletal conditions encountered by health care professionals and is the leading cause of absenteeism in developed societies (Lopez, Mathers, Ezzati, Jamison, & Murray, 2006; Woolf & Pfleger, 2003), accounting for almost 120 million days of certified absence from work each year and about 50% of individuals who are off work for more than 6 months and thus may never return to employment (Maniadakis & Gray, 2000).
The most frequently reported risk factors for LBP are heavy physical work; frequent bending, twisting, lifting, pulling, and pushing; and repetitive work, static postures, and vibrations (Walker, Muller, & Grant, 2004). Other risk factors are psychological and include stress, distress, anxiety, depression, cognitive dysfunction, and job dissatisfaction (Hoogendoorn, van Poppel, Bongers, Koes, & Bouter, 2000; Linton, 2000; Walker et al., 2004). The most common presentation of LBP is impaired spinal movements (National Health and Medical Research Council, 1999).
Considerable disability and significant costs have been linked to LBP of which the peak occurrence normally occurs between ages 35 and 55 years (Walker et al., 2004). According to van der Roer, Goossens, Evers, and van Tulder (2005), the economic costs of managing LBP are increasing globally as health care budgets are decreasing. The direct health care cost of LBP was estimated at £1.6 billion in the United Kingdom, and the indirect cost of informal care and lost productivity was estimated at £10.6 billion (Maniadakis & Gray, 2000). The total costs associated with LBP in the United States exceed US$100 billion per year, two thirds of which are the result of lost wages and less productivity (Katz, 2006). The lifetime prevalence of LBP (i.e., at least one episode of LBP in a lifetime) in developed countries is reported to be up to 85% (Walker, 2000). The prevalence of LBP is due in part to an aging population and higher obesity rates, and likely to affect almost everyone at some point (Deyo, Mirza, & Martin, 2006). A systematic review by Louw, Morris, and Grimmer-Somers (2007) indicated that the epidemiology of LBP in developing countries is comparable to reports of research in developed nations.
The substantial disability arising from LBP can affect activities of daily living (e.g., dressing, personal hygiene, eating, and work), sleep, mood, and concentration (Parahoo, 2000). Individuals with LBP tend to have lower health-related quality of life, and the longer complaints of LBP continue, the greater the impact psychosocial factors may have on disability, greater than either biomedical or biomechanical factors (Parahoo, 2000).
A long episode of LBP does not necessarily imply an unfavorable prognosis. The prognosis for LBP is generally favorable, with more than 65% of symptoms resolving spontaneously within 12 weeks (Borkan et al., 2002). However, recurrent LBP is common and associated with delayed return to work and low socioeconomic status (Iles & Davidson, 2006). The main aim of rehabilitation is overcoming physical, psychological, and sociological barriers (Berger, 2007), which includes supporting patients when the pain they are experiencing is disabling and interferes with their activities of daily living, educating patients who fear they will make their condition worse if they engage in exercise and physical activity, tailoring exercises so that they work for patients and encourage self-management, providing counseling for patients experiencing psychological symptoms, and encouraging social support.
At present, many intervention algorithms for LBP have been developed, but no single algorithm has been shown to be superior (Heymans, van Tulder, Esmail, Bombardier, & Koes, 2005). As a result, several discrepancies in the management of LBP exist among clinical health professionals’ practices, even among members of the same professional groups and providers in different countries. A lack of scientifically sound clinical guidelines and research recommendations can contribute to variability in LBP management (Louw et al., 2007).
This emphasis on quality clinical guidelines resulted in an international collaborative of researchers and policy makers using the Appraisal of Guidelines Research and Evaluation (AGREE) tool to improve the quality and effectiveness of clinical practice guidelines by establishing a shared framework for their development, reporting, and assessment (The AGREE Collaboration, 2003).
Clinical guidelines are systematically developed statements to improve practitioners’ and workers’ decisions about appropriate health care under specific circumstances (Louw et al., 2007) and are often considered the gold standard of best evidence in health care (Rothstein, 2001). Several guidelines for LBP have been developed to assist health care professionals in managing simple to complex physical, psychosocial, ethical, and regulatory concerns about the management of LBP. These LBP guidelines integrate key points from evidence-based to expert practice (Guzman et al., 2001). In spite of the substantial resources invested in the development of current LBP clinical practice guidelines, little has been done to address their quality, efficacy, and recommendations for AGREE to improve health care (Dagenais, Tricco, & Haldeman, 2010; Holohan, Deenadayalan, & Grimmer, 2006). The aim of this critical review was to assess the quality of LBP guidelines using the AGREE instrument.
Method
A search of the literature was undertaken to find relevant guidelines on LBP; Google Scholar, Medline, Embase, National Guideline Clearinghouse, and PEARLing databases were searched. The search terms used were low back pain, back pain, acute low back pain, chronic low back pain, and guidelines. To be selected, the guidelines had to meet the following inclusion criteria: (a) published or updated from 2000 to 2015, (b) major focus on LBP, (c) published in English, and (d) available electronically. Guidelines were excluded if they (a) focused on a single therapeutic intervention, (b) were copies or summaries of previous guidelines, (c) were limited to a treatment algorithm without additional explanations, or (d) were narrative reviews without evidence-based recommendations.
After reading the AGREE instrument training manual, the author completed a 2-hour training session online. The AGREE instrument was used to appraise key components of guideline quality including the rigorous process of development and impact on clinical practice. To validate the findings, an independent reviewer familiar with the AGREE instrument independently appraised the guidelines, which lead to discussions between the reviewers until a consensus was reached on relevant items. The AGREE instrument has been shown to be a reliable and valid generic instrument designed to assess the methodological quality of clinical guidelines (MacDermid et al., 2005; The AGREE Collaboration, 2003). The reliability of the AGREE instrument depended on the domain and number of appraisers (0.17-0.81 for single appraiser; 0.30-0.96 when scores were averaged between a pair of appraisers; MacDermid et al., 2005). The construct validity of the AGREE instrument has been supported; expected differences in domains have been observed between expert panels and reviewers with no or uncertain expertise (difference of 10%-21%, p = .09-.001; MacDermid et al., 2005).
The AGREE instrument includes 23 items organized into six domains, scope and purpose, stakeholder involvement, rigor of development, clarity and presentation, applicability, and editorial independence. Guidelines with clear scope and purpose specifically describe objectives and patient applicability. Stakeholder involvement is successfully addressed when all relevant groups, including patients, are included in the guideline development process, with the target users defined and guidelines piloted. Guidelines with rigor in their development use systematic methods to search and select evidence, with an explicit link between evidence and recommendation formulation. Guidelines must effectively address clarity and presentation, with specific and unambiguous key recommendations and management options, which should be easily identifiable. Applicability involves discussing cost and organizational implications of the guideline and providing monitoring tools. Editorial independence is effectively addressed when conflicts of interest and independence from funding bodies are clearly stated (The AGREE Collaboration, 2003).
The domain score is calculated by summing the scores of the domain items, expressed as a percentage. Domain scores greater than 60% are considered effectively addressed, which is the cutoff value used in the AGREE instrument for overall assessment. The guideline is strongly recommended if it rates three or four of four on the majority of items and the domain scores are above 60%, is recommended if it rates two or three of four on a similar number of items and the domain score is between 30% and 60%, and is not recommended if it rates one or two of four on the majority of items and most domain scores are below 30% (The AGREE Collaboration, 2003).
Results
Following the literature search, 17 LBP guidelines were retrieved, of which only nine met the inclusion and exclusion criteria and were selected for review. The nine guidelines selected, from least to most recent, are listed in the sidebar.
AGREE Description of the Guidelines
Table 1 presents the interventions and time period covered by the guidelines. Exercise and passive treatment were covered by all guidelines. Cognitive behavioral therapy (CBT; 1-3, 5-9), medication (1-2, 5-9), education (3-9), and surgery (1, 4, 7-9) were covered by most guidelines; equipment (1-2, 4-5) and injections (4-6, 8) were covered by a minority of guidelines.
Characteristics of the Selected Guidelines.
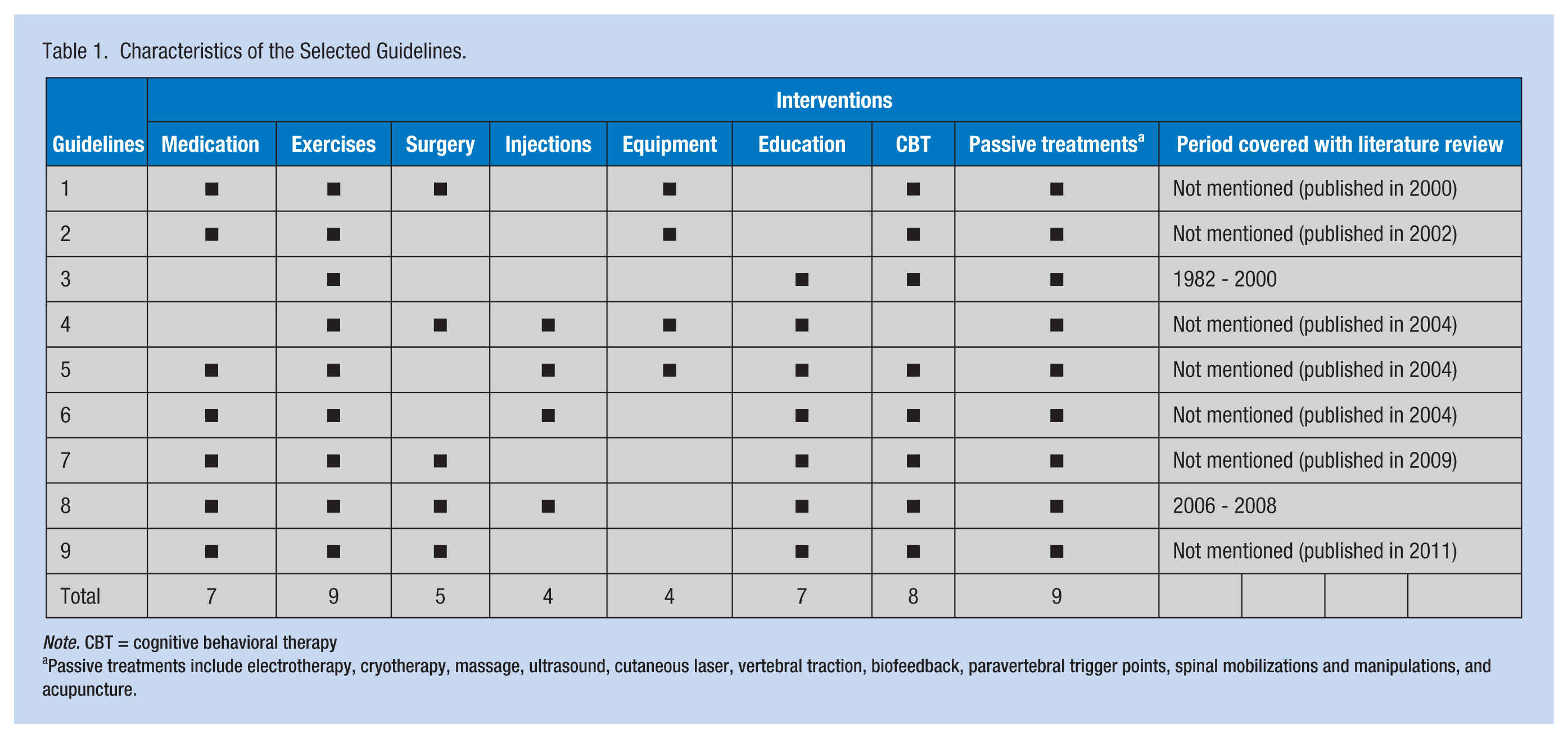
Note. CBT = cognitive behavioral therapy
Passive treatments include electrotherapy, cryotherapy, massage, ultrasound, cutaneous laser, vertebral traction, biofeedback, paravertebral trigger points, spinal mobilizations and manipulations, and acupuncture.
AGREE Grading of the Guidelines
All guidelines graded their recommendations based on the strength of available evidence. The grading ranged from randomized controlled trials to systematic reviews to expert opinions and formal consensus.
AGREE Evaluation of the Guidelines
Variability among guidelines in the domains was effectively addressed. Guidelines 5 and 6 effectively addressed five domains, Guidelines 3 and 7 effectively addressed four domains, Guidelines 1, 4, and 8 effectively addressed three domains, and Guidelines 2 and 9 effectively addressed two domains.
Guidelines 1 and 4 effectively addressed stakeholder involvement, rigor of development, and clarity and presentation, but poorly addressed editorial independence. Guideline 2 effectively addressed rigor of development and clarity and presentation, but poorly addressed editorial independence. Guidelines 3 and 7 effectively addressed scope and purpose, rigor of development, clarity and presentation, and editorial independence. Guidelines 5 and 6 effectively addressed scope and purpose, stakeholder involvement, rigor of development, clarity and presentation, and editorial independence. Guideline 8 effectively addressed rigor of development, clarity and presentation, and editorial independence. Guideline 9 effectively addressed scope and purpose, and rigor of development, but poorly addressed stakeholder involvement.
Guidelines 5 (72%), 7 (69%), and 6 (68%) had the highest domain scores; Guidelines 9 (48%) and 2 (45%) had the lowest domain scores. According to AGREE scoring, Guidelines 3, 4, 5, 6, and 7 were classified as effectively addressed. On the basis of appraisal and domain scores, Guidelines 3, 5, 6, and 7 were strongly recommended, Guideline 4 was recommended, and Guidelines 1, 2, 8, and 9 were not recommended.
AGREE Recommendations of the Guidelines
A recommendation summary, related to each intervention, is listed below for each guideline. A lack of consistency in the specificity of interventions recommended in the guidelines was identified, with some guidelines being more general and others more detailed.
Medication
Medication was recommended in seven (1-2, 5-9) of the nine guidelines. Paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDs) were recommended as initial pain treatment in seven (1-2, 5-9) guidelines. Nonsteroidal anti-inflammatory drugs can be used in conjunction with paracetamol, or independently if paracetamol had been prescribed previously. Alternatively, muscle relaxants were recommended in five (1, 5-6, 8-9) guidelines if the preceding medications were ineffective; however, muscle relaxants were recommended for short-term use only due to the danger of addiction, and this recommendation was emphasized in three guidelines (1, 5-6). The use of opioids for severe musculoskeletal pain was recommended in four (1, 5-7) guidelines. Codeine, tramadol, oral oxycodone, and morphine were only recommended in Guideline 2; tricyclic anti-depressants were only recommended in Guideline 7; and gabapentin was only recommended in Guideline 9.
Exercises
Exercises were recommended as an intervention in all nine guidelines. With regard to specificity of exercises, aerobic and trunk conditioning was mentioned in seven guidelines (2-4, 6-9), back exercise class in six guidelines (1-2, 4-7), encouraging normal activities in six guidelines (2, 4-8), and muscle conditioning in six guidelines (2-3, 5-7, 9). Mobility exercises were mentioned in five guidelines (3, 6-9).
Surgery
Surgery was recommended as an intervention in five guidelines (1, 4, 7-9). Surgery for herniated disc was recommended in four guidelines (1, 4, 7-8); for unsatisfactory reduction in nerve root pain (1, 8-9), progressive neurological signs (1, 7-8), and persistent pain (1, 7, 9) in three guidelines. Surgery was generally recommended in chronic pain patients with moderate to severe disability where conservative treatment had not been effective.
Injections
Injections were recommended as an intervention in four (4-6, 8) guidelines. Epidural steroids were recommended in four guidelines (4-6, 8), and facet joint injections were recommended in three guidelines (5-6, 8). The injections were generally recommended as second-line treatments, with relatively short-term benefits and associated adverse effects, although Guideline 5 reported adverse effects as rare.
Equipment
Equipment was mentioned as an intervention in four (1-2, 4-5) guidelines. Lumbar support belts (1-2, 5) and corsets (2, 4-5) were recommended in three guidelines. The use of the above equipment has not been found to have more effect than other measures as either a preventive or treatment measure.
Education
Education was mentioned as an intervention in seven guidelines (3-9). Information and advice were mentioned in seven guidelines (3-9), and back booklets or pamphlets were mentioned in five (4-8) guidelines. Coaching (3) and back books and videos (7) were the least recommended interventions.
Cognitive Behavioral Therapy
Cognitive Behavioral Therapy was mentioned as an intervention in eight guidelines (1-3, 5-9). Using cognitive models was the most recommended approach (1-3, 7-8). Other recommended approaches included multiprofessional cognitive approaches to communication, mentioned in four guidelines (1, 5, 7, 9). Group (1, 5, 7) and individual (1, 3, 6) CBTs were mentioned in three guidelines. Psychological screening or testing was the least recommended intervention. Generally, only if psychological factors retard recovery is a possible referral to a psychologist for screening or testing recommended.
Passive Treatments
Passive treatments were recommended as an intervention in all nine guidelines. Treatment with traction (1-7, 9), ultrasound (1-4, 6-9), and massage (1-7, 9) was recommended in eight guidelines. Acupuncture and transcutaneous electrical nerve stimulation (TENS; 1-2, 4-7, 9) were mentioned in seven guidelines. Hot and cold compresses (2, 4-6, 8-9) were recommended in six guidelines. Infrared was the least recommended intervention. Generally, most passive treatments were recommended during the initial visit but should be avoided as mono-therapy and not be used routinely because these therapies may increase the risk of illness behavior and chronicity. Prolonged passive treatments can also increase health-related costs substantially.
Discussion
Clinical guidelines have been developed for evidence-based practice (Louw et al., 2007). Although guidelines can improve health care and efforts to develop guidelines are continuous, the quality of guidelines is questionable (Louw et al., 2007). In addition, to ensure that only the best scientific evidence is used by health care professionals, assurances about the quality of recommendations regardless of origination are needed (Graham, James, & Cowan, 2000).
The AGREE appraisal demonstrated that the guidelines effectively addressed only a few domains. Rigor of development was the domain most effectively addressed, followed by clarity and presentation. The most poorly addressed domain was applicability, with no guideline effectively addressing this domain. It may be difficult for guideline developers to effectively address how they ensured that the guidelines were developed with rigor because they would have to account for organizational and financial barriers and piloting the guideline with service users. This process may be met with organizational resistance and the cost could be substantial.
Editorial independence was only effectively addressed in five guidelines. The other four guidelines did not mention editorial links so it is unclear whether an error of omission or actual conflicts of interest were in play. It is suggested that guidelines either mention their editorial links or simply state no conflicts of interest to ensure that health care professionals using LBP guidelines do not read the recommendations with apprehension and are assured that the recommendations are not biased by the views or interests of a third party (e.g., a funding source).
As for stakeholder involvement, only four guidelines effectively addressed this domain. Perhaps the developers of LBP guidelines do not understand the value of consulting relevant stakeholders, in particular patients. It has been suggested that involving stakeholders improves the applicability of the recommendations and facilitates compliance among patients (Fretheim, Schunemann, & Oxman, 2006). Involving stakeholders could be demonstrated by sharing power and responsibility. This finding may simply be a lack of understanding on the part of the developers regarding the advantages of stakeholder involvement. However, the lack of stakeholder involvement could potentially raise the ethical issue of beneficence, or lack thereof. It could be argued that in cases where no stakeholders are involved, the recommendations may not be made in the best interest of benefiting patient care, but with a hidden agenda to promote a particular intervention. The literature supports stakeholder involvement in guideline development, and collaboration with developers should be encouraged (Boyd & Bero, 2006; Fretheim et al., 2006).
The scope and purpose of the guidelines was only effectively addressed in five guidelines. It is suggested that guidelines clearly state their objectives and specific patient populations that could benefit from the recommendations to ensure that health care professionals easily and quickly select a guideline to answer their specific clinical questions, thereby reducing guideline selection ambiguity.
It appears that in following the AGREE appraisal, only four guidelines met the quality standards and were strongly recommended. However, even these guidelines failed to effectively address all the domains, which suggests that producing high-quality guidelines for LBP remains a challenge.
Interventions with the strongest evidence were back exercises, CBT, medication, and patient information and education; interventions with less evidence included injections and electrotherapy. Variability was found in the level of guideline detail for each intervention. This finding may have been influenced by the interests, requirements, and available resources of the development team, which could have influenced the types, extent, and various forms of the interventions addressed.
This critical review highlights the relatively large number of interventions available to health care professionals and workers when managing LBP in both the acute and chronic stages of the condition. The actual choice of intervention at each stage is mainly dependent on the health care professional’s judgment and intuition. Factors such as years of clinical experience, additional training, and patient preference can also influence intervention choices (O’Brien, 2001). Health care professionals must identify all possible treatments, be conversant about all interventions, make appropriate referrals to other health care professionals, and ensure a holistic approach to worker care.
The general advice for medication was simple analgesia for initial pain, and then more potent medications, if initial pain control fails. However, caution is needed to minimize side effects and possible drug dependency.
Interventions such as patient information and education, back exercises, and CBT were recommended during both acute and chronic stages, despite acute and chronic LBP being two distinct entities (Walker et al., 2004). The type of back exercises varied among guidelines, with the general consensus being to encourage normal activity, back exercise classes, and muscle conditioning. Although patient information and education was mentioned for both acute and chronic stages, the specific content of this education was not clear.
Conclusion
This critical review revealed that only four guidelines achieved quality standards according to the AGREE criteria. It is suggested that the interventions recommended should be more clearly specified with greater emphasis on differentiating interventions for acute and chronic LBP. Future LBP guidelines should specify patient information and education interventions more explicitly, as this would assist health care professionals in applying this intervention. A need to improve translation of research evidence to guidelines to clinical practice is clear.
Back Pain Guidelines
Guideline 1: The Norwegian Guideline (The Norwegian Back Pain Network, 2002)
Guideline 2: New South Wales Guideline (New South Wales Therapeutic Assessment Group, 2002)
Guideline 3: National Practice Guidelines for Physical Therapy in Patients with Low Back Pain (KNGF; Bekkering et al., 2003)
Guideline 4: The New Zealand Guideline (New Zealand Guidelines Group, 2004)
Guideline 5: The Australian Guideline (Australian Acute Musculoskeletal Pain Guidelines Group, 2004)
Guideline 6: The European Guideline (Van Tulder et al., 2006)
Guideline 7: National Institute for Health and Clinical Excellence (NICE; 2009) Guideline.
Guideline 8: The University of Michigan Guideline (University of Michigan Health System, 2010)
Guideline 9: Low Back - Lumbar & Thoracic (Acute & Chronic) Guideline (Work Loss Data Institute, 2011)
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Laran Chetty is a senior physiotherapist working in the Occupational Health Department at the Royal Free London NHS Foundation Trust. He has worked in the occupational health arena for more than 10 years in corporate and public sectors.