
Abstract
MJ is a janitor working in an office building for the past 5 years. He sustained a third-degree burn with a secondary infection and was sent to the county hospital. He was diagnosed with leprosy. The employees in the office building were concerned with the risk of transmission. This article reviews leprosy, and implications for occupational health nurses are discussed.
MJ is a 53-year-old man, employed by a subcontractor, who had worked as a janitor for the past 5 years cleaning sections of a five-story office building in northern California. He was well liked by his coworkers, often invited to join office parties. He ate lunch in various workplace breakrooms.
MJ was born in a small Central American village. He came to the United States when he was in his 30s. Even though he did not speak English when he arrived, he was hired for janitorial work and has worked for the same subcontractor. He has never missed a day of work.
MJ had noticeable areas of hypopigmentation on his skin. He would occasionally drop a broomstick or fall when walking up stairs. One day, while cleaning a stove, he placed his hand on a plate heated to 120 degrees, did not feel the heat, and sustained third-degree burns. The next day, MJ had black and red areas on his hand and was told to go to the county hospital for evaluation where he was admitted for burns and cellulitis. One of his coworkers reported that while he was being treated in the burn unit, he was diagnosed with leprosy.
The office workers in the building were concerned that they had been exposed to leprosy and wondered if they were at risk for developing the disease. This article reviews the signs and symptoms of leprosy and the risk of contracting the disease if exposed.
Hansen’s Disease
Hansen’s disease (leprosy) is caused by Mycobacterium leprae, an acid-fast aerobic rob-shaped bacillus classified as obligate intracellular mycobacterium. Due to its slow growth, it cannot be grown in a laboratory or in vitro. However, it can be grown in vivo, usually on the foot pads of mice and armadillos. In humans, the incubation period ranges from 5 years to 20 years (World Health Organization [WHO], 2015).
M. leprae replicates inside histiocytes and attaches to Schwann cells in the peripheral nervous system. M. leprae induces demyelization and a loss of axonal conductance which leads to nerve damage (Bhat & Prakash, 2012). The bacilli reproduce inside the macrophages at the site of entry, usually the skin or nasal cavity. The infection then induces T-helper lymphocytes, epithelioid cells, and giant cells to form patches of hypopigmentation on the skin accompanied by pain and loss of sensation in the area. Hansen’s disease has two phases. The first phase, tuberculoid leprosy, is characterized by a few skin lesions with some sensory changes but is confined to the peripheral nervous system and skin. Individuals lose hair and sweat glands in the skin lesions as well as develop hypersensitivity (Fauci et al., 2015).
The second phase, lepromatous leprosy, is characterized by nodules with raised plaques, often on the face. The skin becomes dry and scaly. Bacilli can be found in large numbers on the skin and in the blood. Degenerative myelination and axonal degeneration occur. A symmetric peripheral neuropathy develops that starts in the sacral region and descends distally. In this phrase, cellular immunity is impaired (Fauci et al., 2015). Workers may develop Lucio’s phenomenon in which ulcers develop on the extremities. A secondary infection may also occur and later sepsis (Fauci et al., 2015).
Epidemiology
According to the WHO, leprosy is endemic in 138 countries (WHO, 2015). The global prevalence of leprosy in 2015 was 0.2 cases per 10,000 individuals (WHO, 2015). The global incidence of leprosy in 2014 was 213,899 cases (WHO, 2015). Ninety-four percent of new cases originated in only 14 countries (WHO, 2015). In the United States, 178 new cases were reported in 2015 with 72% of these new cases in Arkansas, California, Florida, Hawaii, Louisiana, New York, and Texas (Health Resources and Service Administration [HRSA], 2015).
Transmission
Leprosy can be transmitted from person to person via droplets from the nose and mouth (Centers for Disease Control and Prevention [CDC], 2017), skin contact, or respiratory route (Bhat & Prakash, 2012). The bacilli are found in nasal and sebaceous secretions; early in the disease, the mycobacterium burden may be low with less risk of transmission (Bhat & Prakash, 2012). Any worker exposed to (e.g., handled or eaten) an armadillo should be evaluated because armadillos are natural carriers of the disease (Truman et al., 2011). The mycobacterium can also be found in contaminated soil (Fauci et al., 2015).
Workers living in poor conditions with contaminated water or limited diet may also be at risk for developing leprosy. Intimate contact with an infected individual may also increase the risk of transmission; leprosy can be transmitted during tattooing (Fauci et al., 2015). Immunocompromised individuals are at risk for leprosy (Bhat & Prakash, 2012). If an individual with HIV and subclinical leprosy begins antiretroviral therapy, subclinical M. leprae may be activated (Bhat & Prakash, 2012).
Hansen’s disease appears to have a genetic component to transmission (Alter, Grant, Abel, Alcais, & Schurr, 2011). Individuals with the nucleotide-binding oligomerization domain-containing protein 2 (NOD2) gene associated with Crohn’s disease, and individuals with the low lymphotoxin-α (LTA) gene associated with myocardial infarction appear at increased risk for contracting leprosy (Alter, Abel, Alcais, & Schurr, 2011). Other genetic variants (e.g., LTA-producing allele) can be major risk factors for leprosy (Bhat & Prakash, 2012).
Diagnostics
No laboratory tests can unequivocally diagnose leprosy. The best diagnostic is skin biopsy (CDC, 2017). To focus the diagnostician, it is essential to list the client’s signs and symptoms on the laboratory request as well as the possible diagnosis of leprosy (Table 1). Health care workers should be aware that sending a sputum sample for acid-fast bacilli may be misinterpreted as pulmonary tuberculosis (Fauci et al., 2015).
Differential Diagnosis of Leprosy
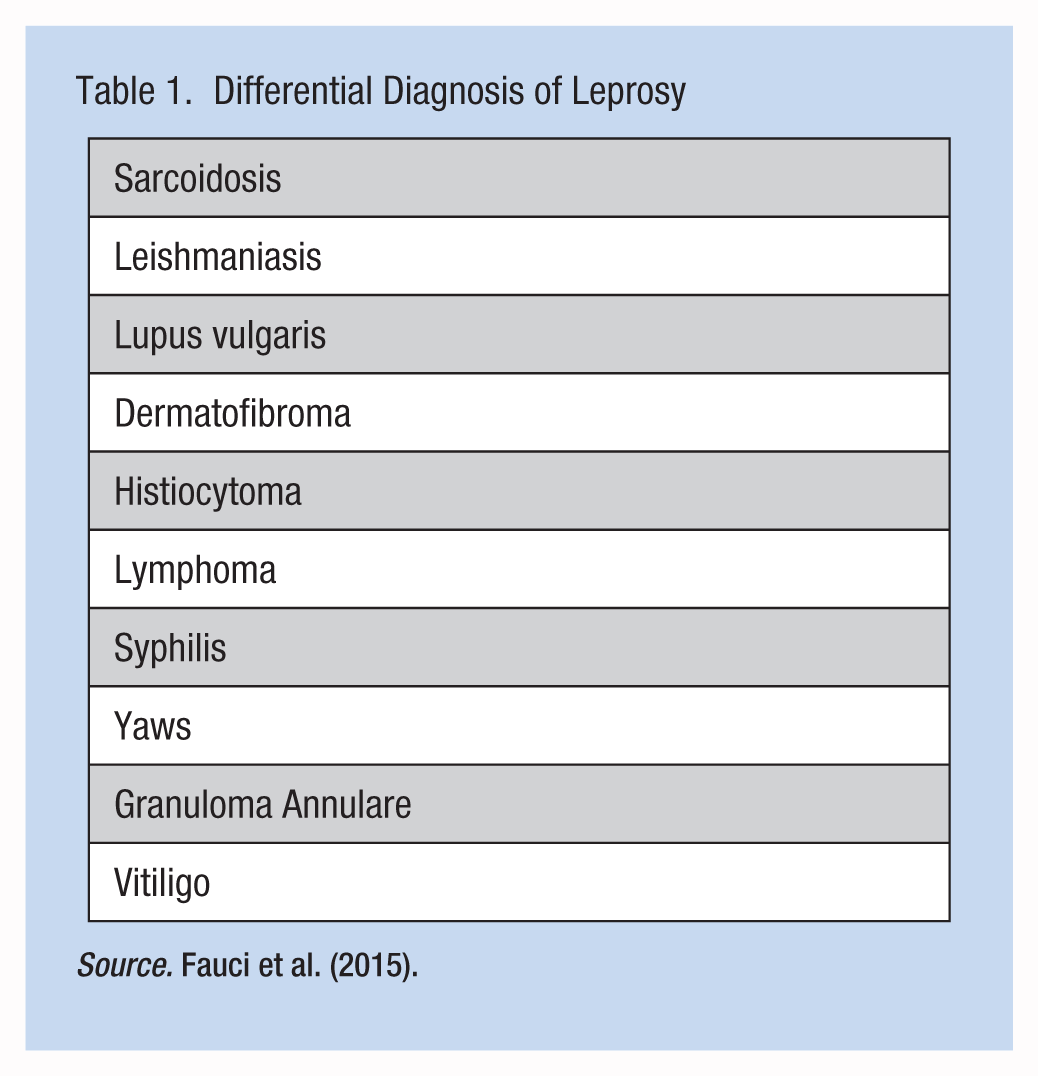
Source. Fauci et al. (2015).
Signs and Symptoms
Symptoms mainly affect the skin, nerves, and mucous membranes. Hypopigmented macules or papules are accompanied by sensory loss. The skin is very dry, thickened, and stiff. Neuropathy, both sensory and motor, develops slowly and can progress to paralysis. Blindness can occur as well as ulcers on the soles of the feet.
The physical examination should include testing for fine touch and vibratory sensation. Motor strength testing determines median nerve involvement, thumb opposition, and grip. Wrist drop may occur if the radial nerve is involved. Foot drop may occur as a result of damage to the peroneal nerve. Cranial nerve palsies, as well as corneal insensitivity, may cause ulcerations and secondary infections. Males may become impotent and sterile.
It is not uncommon for these individuals to experience injuries such as burns or fractures because they do not perceive pain. Other symptoms include fever, malaise, anorexia, and arthralgia. Signs may include enlarged lymph nodes, weight loss, and edema during the course of active disease.
Treatment
Because M. leprae cannot be grown in a laboratory or in vitro, it is challenging to conduct susceptibility testing (Fauci et al., 2015). Treatment requires multiple medications prescribed for 3 years to 5 years. Rifampin, an antibacterial, is taken for 3 years to reduce the number of bacilli. Dapsone inhibits folic acid synthesis in bacteria and is taken for 5 years. Individuals with tuberculoid leprosy may be prescribed Dapsone only; however, adults with lepromatous leprosy may be prescribed both Dapsone and Rifampin. Individuals prescribed Dapsone, which may restore skin to its natural pigmentation, may require testing for glucose-6-phophate dehydrogenase deficiency due to the risk of developing hemolytic anemia and methemoglobinemia (Fauci et al., 2015).
Other medications include streptomycin, ethionamide, prothionamide, aminoglycosides, or fluoroquinolones (Fauci et al., 2015). The choice of therapy is based on the bacterial burden and the level of cellular immune response (Fauci et al., 2015). Vaccines at birth, such as Calmette–Guérin, may prevent leprosy; however, results are variable (Fauci et al., 2015). The use of Dapsone for individual prophylaxis with household contacts varies depending on the phase of the patient’s leprosy. Prophylaxis may be effective in the tuberculoid phase but not in the lepromatous phase. The WHO provides treatment regimens for clinicians to follow.
Implication for Occupational Health Nurses
Workers with leprosy must comply with treatment. Injury prevention is a priority. The occupational health nurse should inspect hands and feet for ulcers. Affected workers should be instructed to avoid injuries and report to the occupational health clinic when an injury or accident occurs because these workers may not experience pain.
The damage to the peripheral nervous system is not reversible, and because of the peripheral neuropathy, these workers may be at risk for falls. Occupational and physical therapy consults may be needed. Occupational therapists may work with grip strength and appropriate equipment for eating and bathing. Physical therapists may be consulted for gait and balance training. These workers must be monitored by an infectious disease provider as well as an ophthalmologist for eye care. Pain management may be needed for the peripheral neuropathy.
Conclusion
Due to the low risk of transmission, MJ’s coworkers may not be at risk for developing Hansen’s disease. MJ may continue working; however, he may need a fit for duty evaluation because of neuropathy.
Footnotes
Conflict of Interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann R. Lurati is a nursing lecturer at California State University Monterey Bay School of Nursing.