
Abstract
In this study, the authors determined the effect of a structured Internet-delivered Mantram Repetition Program (MRP) on burnout and stress of conscience (SOC), stress related to ambiguity from ethical or moral conflicts among health care workers (HCWs) within the Veteran Affairs (VA) Healthcare System. A secondary purpose was to determine whether practicing meditation prior to the study combined with MRP affected burnout or SOC. The MRP teaches the mindful practices of repeating a mantram, slowing down, and one-pointed attention for managing stress. Thirty-nine HCW volunteers who provided direct patient care completed the Internet-delivered MRP. The outcomes of burnout (i.e., exhaustion, cynicism, and professional efficacy) and SOC (i.e., frequency of stressful events and troubled conscience about those events) were measured at baseline (T1), postintervention (T2), and 3-months postintervention (T3). Repeated measures ANOVA indicated that exhaustion significantly (p < .05) declined between T1 and T3; professional efficacy and cynicism did not change during the study. The same statistical model also indicated the frequency of stressful events significantly declined between T1 and T2 and troubled conscience declined between T1 and T3. Secondary analysis demonstrated that individuals who did not practice meditation at baseline (n = 16, 41%) significantly decreased exhaustion, frequency of stressful events, and troubled conscience between T1 and T3, and improved professional efficacy between T1 and T2. Individuals who practiced meditation at baseline (n = 23, 59%) did not demonstrate significant change on any study outcomes. An MRP intervention may reduce burnout and SOC in those individuals who are naïve to practicing meditation.
Work-related stress and burnout are major concerns among health care workers (HCWs). Stress is defined as the physiological and psychological response to a situation that creates physiological arousal and mobilization of psychological coping mechanisms (Cannon, 1929/1957; Lazarus & Folkman, 1984). Burnout is used to describe workers’ response to prolonged stress and, for the purposes of this study, the term is defined as a syndrome in which individuals suffer from exhaustion, cynicism, and reduced professional efficacy (Maslach, Jackson, & Leiter, 1986). In 2012, it was reported that HCWs are significantly more likely than general U.S. workers to report symptoms of burnout, 38% versus 28% respectively, and overall dissatisfaction with work–life balance, 42% versus 23% respectively (Shanafelt et al., 2012). Furthermore, the current literature indicates that HCW burnout may adversely affect their personal relationships, frequency of alcohol use, and suicidal ideation (Shanafelt, Sloan, & Habermann, 2003). Moreover, the negative effects of workplace stress and burnout may contribute to less patient satisfaction, compromise patient safety, and increase costs for health care organizations.
Review of Literature
The potential psychological sequella of health care work coupled with severe staffing shortages and predictions of increasing acuity of hospitalized patients may lead to an overall loss of qualified workers in the field, and ultimately, further jeopardize patient care and safety (Juthberg, Eriksson, Norberg, & Sundin, 2007). Moral and ethical issues frequently emerge in health care workplaces, creating additional worker stress. Examples of this type of stress include real or perceived personal limitations, and barriers to complete tasks or attend to patients’ needs. In turn, these stressors may occupy the thoughts of HCWs and create a “stress of conscience.” Stress of conscience (SOC) is defined as stress related to ambiguity from ethical or moral conflicts (Juthberg et al., 2007) and has been positively associated with perceiving one’s conscience as a burden, emotional exhaustion, and depersonalization (Åhlin, Ericson-Lidman, Ericsson, Norberg, & Strandberg, 2013). The current literature identifies perceived stress emanating from a health care workplace, stress and burnout as leading contributors to SOC among HCWs (Åhlin et al., 2013; Åhlin, Ericson-Lidman, Norberg, & Strandberg, 2015). Stress of conscience is linked to serious health care concerns for HCWs. When considered all together, these workplace stressors may contribute to HCWs’ moral stress and impaired sense of mastery, and lead to alcohol misuse, depression, and suicidal ideation (Shanafelt et al., 2012; Shanafelt et al., 2003; Tuvesson, Eklund, & Wann-Hansson, 2012).
Providing interventions to assist HCWs in coping with stress and burnout has been the focus of a number of studies. One approach to decreasing burnout is for HCWs to gain control of their negative thoughts and learn techniques (e.g., mindfulness) to prevent unrelieved stress overload. Mindfulness increases awareness and skillful responses to mental processes that contribute to emotional distress and maladaptive behavior (Bishop et al., 2004). Strategies that increase mindfulness include mind–body courses to reduce perceived workplace stress and burnout (Cohen-Katz, Wiley, Capuano, Baker, & Shapiro, 2004). Kemper and colleagues (2011) found that nurses have positive attitudes about mind–body therapies to reduce stress. A feasibility study reported 15 minutes of mindfulness once or twice a day for 4 weeks reduced stress and anxiety, and improved quality of life among employees working in a health clinic (Prasad, Wahner-Roedler, & Cha, 2011). A small group of nurses who participated in an 8-week program of Reiki, yoga, and meditation reported less stress, better coping, fewer examples of burnout exhaustion, and more mindfulness (Deible, Fioravanti, Tarantino, & Cohen, 2015). A more recent study with a larger group of pediatric intensive care nurses revealed that a 5-minute mindfulness meditation before each work shift resulted in less stress, and this benefit was maintained up to 1 month after the intervention (Gauthier, Meyer, Grefe, & Gold, 2015).
The Mantram Repetition Program (MRP) is one type of mindfulness intervention that consists of three specific practices: (a) mantram (also called mantra) repetition, (b) slowing down, and (c) one-pointed attention. Mantram is the term preferred by the founder of the method, Eknath Easwaran (2013; www.easwaran.org). A mantram is a self-selected sacred word or phrase to be repeated silently and intermittently throughout the day to train an individual’s attention and redirect unwanted thoughts. Mantram repetition is supported by intentionally slowing down and developing single mindedness. Slowing down means being intentional during the present moment. One pointed attention is being focused without distraction on a self-selected task; one-pointed attention is the opposite of multitasking. Research on the MRP in a variety of patient populations has shown positive health-related benefits such as less stress and improved quality of life (Bormann et al., 2014).
Studies of the MRP have shown significant improvements in reducing stress and improving quality of life and spiritual well-being for Veterans Affairs (VA) employees and Korean nurse managers (Bormann, Becker, et al., 2006; Bormann, Oman, et al., 2006; Yong, Kim, Park, Seo, & Swinton, 2011). The transactional model of stress and coping (Lazarus & Folkman, 1984) supports the potential of MRP to reduce stress and burnout. This model depicts an individual’s reaction to stress, which is dependent on perceptions of both stressful events and the individual’s ability to cope with stressful events. By practicing MRP techniques, individuals may be better able to cope with stressful events. The current study hypothesized that burnout and SOC are types of maladaptive coping, and practicing the tools of MRP provides individuals emotion-focused adaptive coping.
One internal means of decreasing burnout is for HCWs to gain control over their negative thoughts and learn techniques to prevent an overload of unrelieved stress. One strategy is the use of mind–body courses to reduce perceived workplace stress and burnout (Cohen-Katz et al., 2004). The practice of mantram repetition requires intentional, one-pointed focused attention that can slow down, interrupt, or redirect ruminating, stressful thoughts, and encourage a mental pause leading to purposeful directed behaviors instead of impulsive reactions to stress. The MRP practices could be classified as emotion-focused coping or emotional self-regulation (Kemeny et al, 2012). Moreover, by limiting negative thoughts, the incidence of burnout and SOC may decrease.
Mantram repetition also initiates a physiological relaxation response (Friedman, Myers, Krass, & Benson, 1996). With continued application of all three MRP skills, the ability to concentrate improves by activating the brain’s neural networks that govern attention and arousal. Brain imaging studies further explain how repetitive speech (e.g., mantram repetition) results in psychological calmness (Berkovich-Ohana, Wilf, Kahana, Arieli, & Malach, 2015), and has also been shown to slow respirations and heart rate (Peng et al., 2004).
Empirical evidence suggests that burnout is a significant problem for HCWs (Browning, Ryan, Greenberg, & Rolniak, 2006; Komala & Ganesh, 2007). Reducing burnout improves HCWs’ well-being, which is significant during an HCW shortage and when the entire industry is focusing on safe, effective patient care (Poghosyan, Clarke, Finlayson, & Aiken, 2010). In spite of research in the area, significant gaps in the literature exist about HCWs’ stress management and occupational burnout. Of previous studies on fostering coping strategies among HCWs, only one directly evaluated the impact of an MRP intervention on burnout. In that study, the intervention was delivered in a traditional classroom face-to-face setting, which limited its application in clinical environments.
The purpose of this study was to determine the effect of a structured Internet-delivered MRP on burnout and SOC among HCWs within the VA. A secondary purpose was to determine whether regular practice of any kind of meditation prior to the study had a differential effect when combined with MRP on burnout or stress of conscious within the targeted group. These purposes were addressed by testing the hypotheses listed in the “Study Hypotheses” sidebar.
Method
This study used a one-group, repeated measures design comparing outcomes within participants at three time points: baseline (T1) following consent but prior to starting the MRP; posttreatment (T2), immediately following completion of the 3-month MRP intervention; and 3 months following completion of the MRP intervention (T3). For this study, analyses were conducted on data from 39 participants who completed the three data collection protocols over the 6-month study. This sample size was adequate for repeated measures ANOVA over three measurement points with a greater than .80 statistical power to detect a medium effect (f = .25) when the type I error was set at .05 and within-subject correlation of scores was conservatively set at r = .50.
Sample
The sample was recruited nationwide via flyers and blinded group emails from within the VA Healthcare System for a 3-month structured Internet-delivered MRP. The study protocol, including recruitment materials, were approved by the facility’s institutional review board (IRB #08251) that operates in accordance with the Helsinki Declaration of 1975 as revised in 2008. Inclusion criteria consisted of full- or part-time employment providing direct patient care within the VA Healthcare System. Participation was voluntary, and consent was implied by submitting the initial online survey. Participants received up to 6 hours of continuing education credit for completing the six online MRP sessions.
MRP Intervention
The structured Internet-delivered program consisted of six 50-minute classes (the “Program Topics” sidebar). The classes were offered every other week over a 3-month period. During these classes, participants were given examples of where and when to practice with MRP tools and encouraged to practice as much as possible every day during the 3-month study. Participants were sent a downloadable training manual and a course text book, Strength in the Storm (Easwaran, 2013). The Internet-delivered MRP classes included lectures, discussions, and instruction in mantram repetition, including slowing down and one-pointed attention as stress reduction strategies. Each 50-minute class consisted of a lecture and discussion, facilitated synchronously using an interactive virtual meeting format that allowed participants to hear live audio and view PowerPoint presentations on their computers. Information was exchanged when participants asked questions using live meeting technology or telephone conference calls.
Outcomes
All data were collected through an online portal within the VA. Participants completed a brief demographic questionnaire at T1 that queried age, gender, employment tenure, highest academic degree, and current job description. The demographic questionnaire also asked the workers, “Do you currently practice any other types of meditation or mindfulness practice?” with response options of “yes” and “no.” If the employees answered “yes,” they were asked to write in the type of meditation or mindfulness they practiced. Participants completed the burnout and SOC instruments at T1 and again at T2 and T3. Burnout was measured using the Maslach Burnout Inventory–General Survey (MBI-GS), a 16-item questionnaire with a six-point Likert-type response scale. This instrument measured the frequency of three characteristics of burnout: (a) feelings of exhaustion (EX), (b) cynicism (CY) or distancing attitudes toward their jobs, and (c) professional efficacy (PE) or the frequency of negative feelings because of not performing tasks adequately (Maslach, Jackson, & Leiter, 1996). Higher scores on the EX and CY subscales and lower scores on the PE subscale corresponded with higher levels of burnout. The MBI-GS has been shown to be a reliable and valid instrument (Maslach et al., 1996). In this study, internal consistency reliability for the EX subscale was α = .88; for the CY subscale, α = .84; and for the PE subscale, α = .68.
Science of conscience was measured using the SOC Questionnaire (SCQ) that assesses the frequency of nine stressful occurrences and the degree of troubled conscience (defined as conflicts related to one’s basic values and sense of what is right and wrong) resulting from the stressful occurrences (Glasberg et al., 2006). Each stressful occurrence was scored by the participant using a six-point Likert-type scale based on the frequency of the occurrence (1 = almost always to 6 = almost never). The Frequency of Stressful Events (FS) score was the sum of these nine items. In addition, each stressful occurrence was scored by the participant using a similar six-point scale to grade the degree to which the stressful occurrence (0 = no, not at all to 5 = yes, it gives me a very troubled conscience). The Troubled Conscience About Stressful Events (TC) score was the sum of these nine items (Glasberg et al., 2006). The SCQ has been shown to be a reliable and valid instrument for the measurement of SOC in HCWs (Glasberg et al., 2006). In this study, internal consistency reliability for FS was α = .79, and for TC was α = .92.
Analysis
Data were transferred from the online portal where participants completed the demographic, MBI-GS, and the SCQ to SPSS spreadsheets. The data were assessed for violations of parametric testing assumptions by calculating descriptive statistics on all outcome variables at each data collection point. Hypotheses 1 and 2 were addressed by calculating one-way repeated measures ANOVA (R-ANOVA) to determine whether the measures of burnout or SOC changed within the sample over the three data collection points. Two-way repeated measures ANOVA (two-way R-ANOVA) were calculated to assess Hypotheses 3 and 4. This analysis determined whether the proportion of the sample who did (n = 23) or did not (N = 16) practice meditation at baseline had different burnout or SOC over the course of the study. Significant main or interaction effects (p < .05) detected by the R-ANOVA or two-way R-ANOVA were further analyzed with Tukey’s least significant difference post hoc comparisons.
Results
The flow diagram of study participation displayed in Figure 1 indicates that of the 54 participants who initially consented to be part of the study, 39 (72%) supplied data at all three time points. The demographic characteristics of the entire sample and comparisons between the proportion of the sample who did (n = 23) and did not (N = 16) practice meditation at baseline are presented in Table 1. This analysis indicated that the mean age of the entire sample was 51 years; respondents had been employed in their current positions for an average of 6.5 years and employed in the VA system for just above 10 years. The majority of respondents were female (87%) with postgraduate degrees (77%); 36% of the sample were nurses.
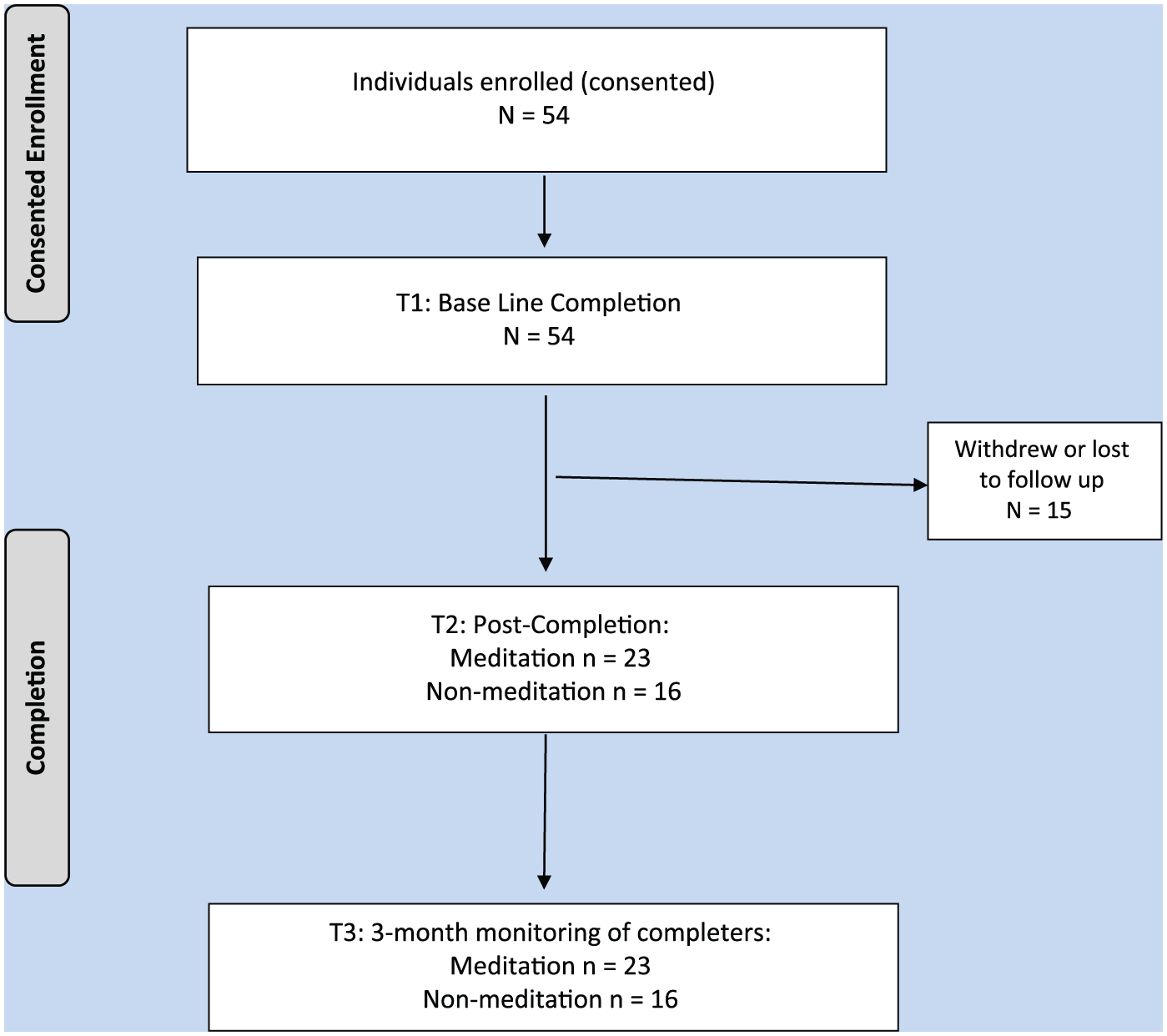
Study flow diagram.
Demographic Comparison of Participants With and Without Meditation Experience
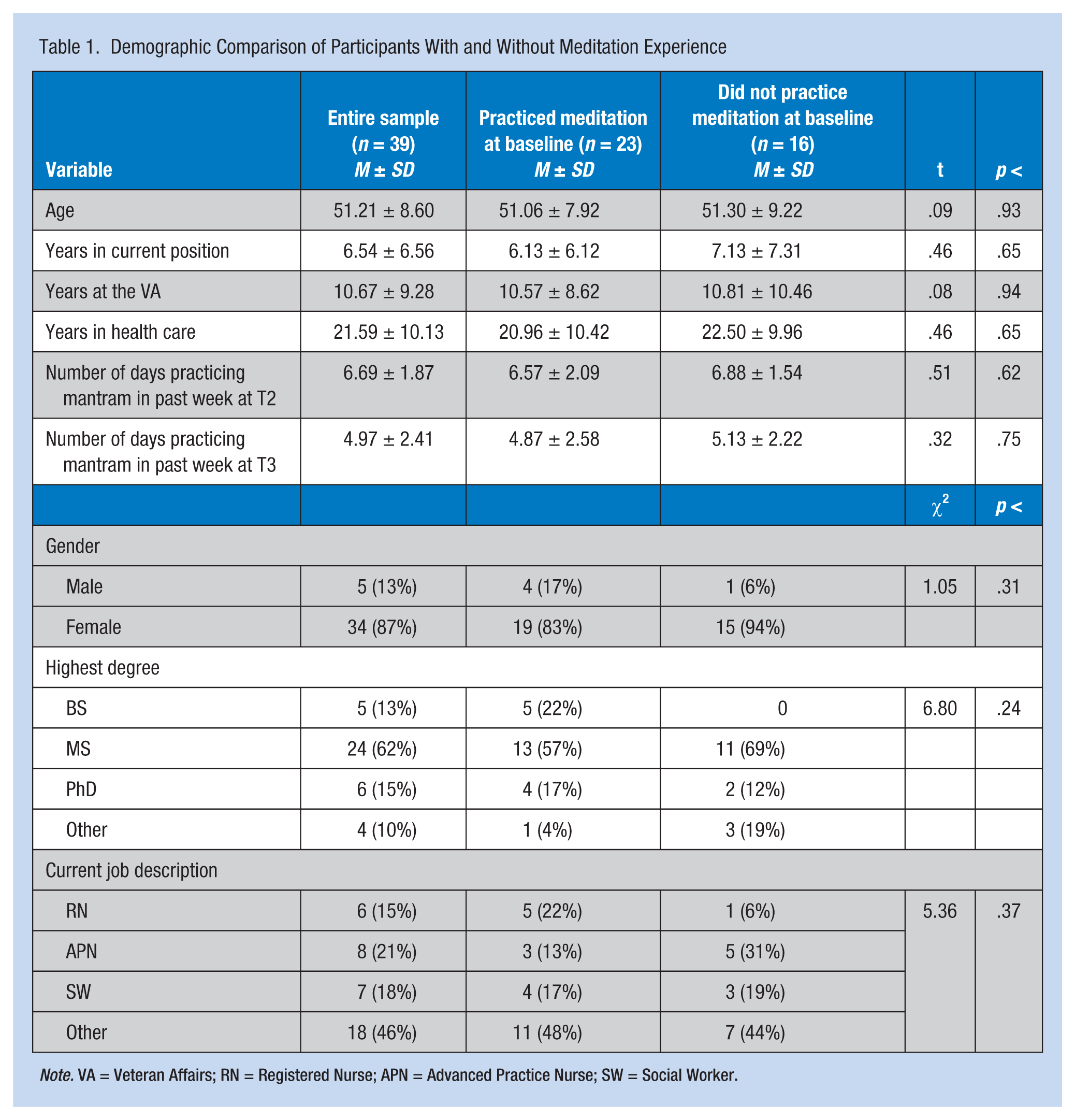
Note. VA = Veteran Affairs; RN = Registered Nurse; APN = Advanced Practice Nurse; SW = Social Worker.
Comparisons of participants who did and did not practice meditation at baseline indicated these groups reported similar demographic characteristics. The most frequently reported types of meditation or mindfulness practiced at baseline (T1) were mindfulness based (35%), yoga (18%), breathing exercises (8%), and prayer (18%). Of the 23 participants who reported practicing meditation at T1, 18 (78%) reported practicing two or more types of meditation.
Results from t tests and chi-square associations presented in Table 1 indicated both groups engaged in a similar number of mantram sessions during the week prior to T2 and during the week prior to T3. Study hypotheses results are presented in Table 2 and indicated respondents exhibited a significant decline in feelings of exhaustion (EX) between T1 and T3. Although this significant decline was realized by the group that did not practice meditation at baseline, the group that did practice meditation at baseline did not report changes in EX over the course of the study. Participants did not report changes in professional efficacy (PE) over the course of the study. The group that practiced meditation at baseline also did not change their PE during the study. However, the group that did not practice meditation at baseline reported a significant increase in PE between T1 and T2; no significant difference in this variable between T1 and T3 was identified. Table 2 data indicate that the entire sample and the meditation/no meditation groups did not change their cynicism (CY) over the course of the trial. The perceived frequency of stressful events (FS) for the entire sample declined from T1 to T2 but was not found to significantly differ between T1 and T3. The group that did not practice meditation at baseline reported lower FS at T2 and T3 compared with T1; the group that did practice meditation at baseline did not change their FS over the three data collection points. The entire sample decreased their perceived troubled conscience about stressful events (TC) between T1 and T3. This significant decline in TC between T1 and T3 was realized by the group that did not practice meditation at baseline, but the group that did practice meditation at baseline did not change their TC during the study.
Burnout, Frequency of Stressful Events, and Troubled Conscience About Those Events Over the Duration of the Study
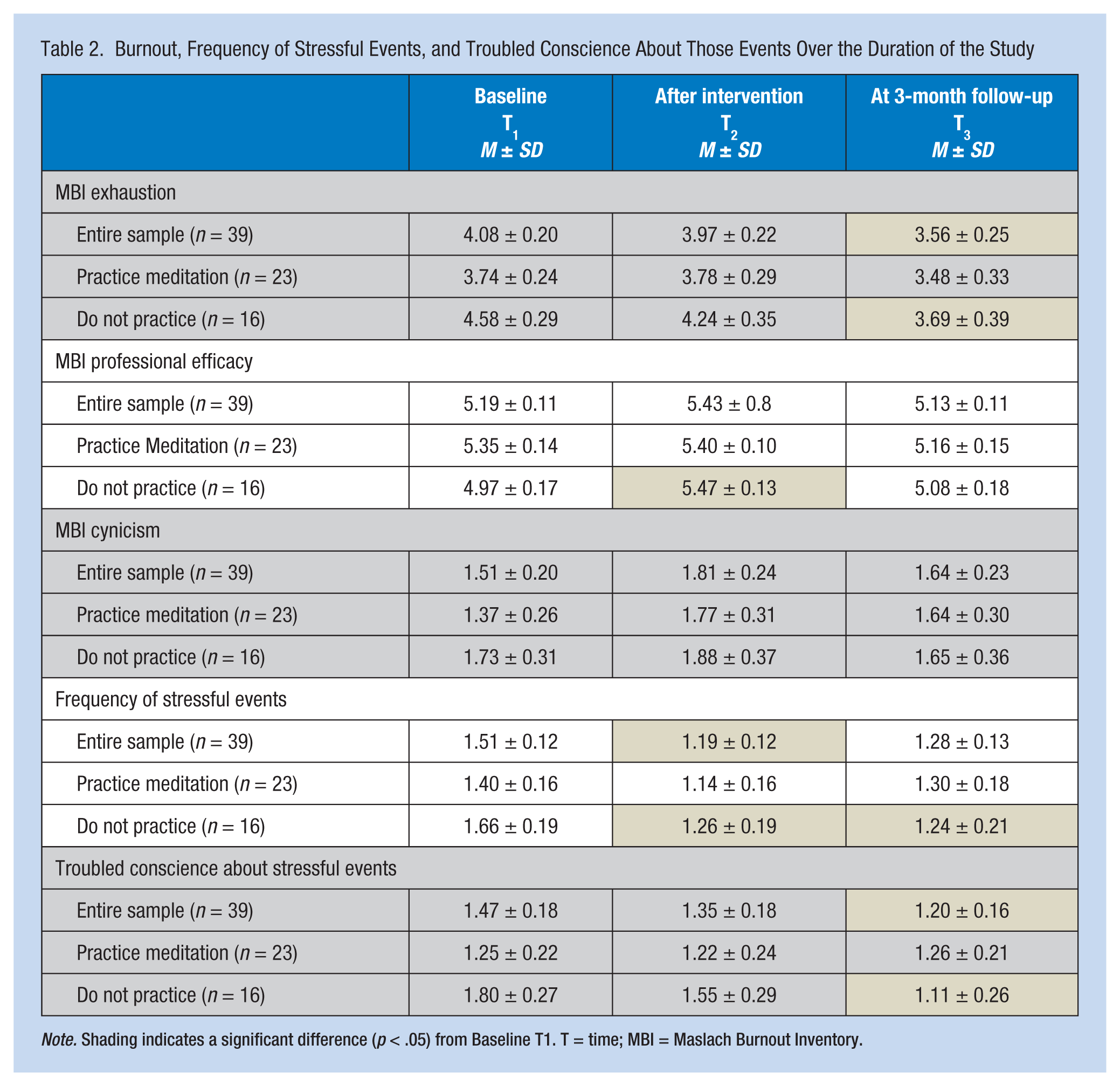
Note. Shading indicates a significant difference (p < .05) from Baseline T1. T = time; MBI = Maslach Burnout Inventory.
Discussion
The findings provide partial support for the study’s research hypotheses. The findings showed that the MRP reduced burnout characteristic of EX and the degree of troubled conscience characteristic of TC for the entire sample between T1 and T3. The entire sample did not report any significant changes in PE, CY, or FS from T1 to T3, although FS of the entire sample was lower at T2 compared with T1. These findings appear to indicate that the MRP can have a long-term effect on exhaustion and troubled conscience about stressful events up to 3 months following the supervised MRP intervention. These findings are consistent with previous investigators who have reported the beneficial effects of health care providers practicing mantram (Bormann, Becker, et al., 2006; Bormann, Oman, et al., 2006; Yong et al., 2011). Another study of employees who completed the MRP reported significant reductions in the exhaustion component of burnout (Leary, Bormann, Georges, Smith, & Andrews, 2014). Also, a review of the effects of mantram (Bormann et al., 2014) has indicated this intervention can reduce psychological distress as well as improve mindfulness and spiritual well-being, in a variety of patient and nonpatient groups.
In addition to the consistency of findings with prior studies that support the efficacy of the MRP intervention for stress reduction and improved quality of life (Bormann, Becker, et al., 2006; Yong et al., 2011), the findings were also supported by Lazarus and Folkman’s transactional model of stress and coping (Lazarus & Folkman, 1984). This model asserts that individuals’ reactions to occupational stress are dependent on their perceptions of stressful events and their ability to cope with these events. Individuals can learn to manage stress and cope with stressful events by practicing problem-focused or emotion-focused coping strategies. The current study hypothesized that burnout and SOC are types of maladaptive coping and that practicing MRP provides individual workers with a type of emotion-focused adaptive coping. Thus, Lazarus and Folkman’s model supports the findings of the current study. Individuals who employ emotion-focused adaptive coping via MRP practices can experience less burnout and stress of conscious.
The beneficial effect of MRP appears to be specific to individuals who had not practiced meditation prior to the study. As Table 2 indicates, participants who did not practice meditation prior to the study reported significant declines in EX, FS, and TC between T1 and T3 and less PE and declining FS between T1 and T2. These findings are in contrast to the group that practiced meditation prior to the study; no changes in any of the outcome variables were observed in this subgroup between any of the data collection points. One explanation for MRP not affecting the individuals practicing meditation before the study is that both MRP and meditation have a similar effect, reducing burnout and stress of conscious. This explanation is supported by the observation that the group that practiced meditation prior to the beginning of the study exhibited consistently, although not statistically significantly, more favorable measures of burnout and stress of conscious at T1. This finding suggests that future researchers may choose to study the beneficial effects of MRP only with groups naïve to practicing mantram or any other form of mindfulness. Including individuals who practice some form of mindfulness in an intervention study examining the impact of MRP may dilute the effect size of the intervention and limit the true impact of the intervention.
The findings of this study must be interpreted cautiously. Although the findings are consistent with previous studies and theoretical constructs, the proposed benefits of mantram identified in this study may have been affected by a number of threats to internal and external validity. First, the study did not include a “no intervention” control group. Including a control group in the design would have minimized the possible effects of environmental or individual factors changing over the course of the study that may have affected the outcomes. Second, the project team did not monitor whether participants engaged in other forms of meditation during the study. The decision to eliminate a control group and refrain from monitoring other forms of meditation among the sample was an attempt to recruit and retain a diverse sample. Recruitment efforts may have resulted in a smaller homogeneous sample with limited external validity if participants were informed a priori they could be assigned to a control condition or if they had to discontinue their current meditation practices. The design employed in this study attempted to balance the need for rigorous internal validity with recruiting a more diverse population. The final validity threat was the potentially low statistical power of the analysis resulting from the small sample size for the two groups (i.e., those who did and those who did not engage in meditation prior to beginning the study). This low statistical power was evidenced by the PE and CY variables favorably trending over the duration of the study, although not achieving statistical significance, particularly in the group that did not meditate before enrolling in the study. Future studies may wish to employ the effect sizes reported in this study to justify the sample sizes of future studies examining the impact of mantram on burnout and stress of conscious.
Implications for Occupational Health Nursing Practice
The study findings have a number of implications for occupational health nurses within health care systems. The ultimate goal of these nurses is to improve worker outcomes while containing costs (Kutney-Lee et al., 2009; McHugh, Kutney-Lee, Cimiotti, Sloane, & Aiken, 2011). Occupational health workers may reduce burnout and SOC by encouraging HCWs to practice with the MRP tools. These tools are practical and portable because they can be implemented anytime and anywhere. Prior studies of HCWs, including nurses, who have participated in MRP have reported less perceived stress and anxiety and improved spiritual well-being and quality of life (Bormann, Becker, et al., 2006; Bormann, Oman, et al., 2006). Such improvements in psychological distress are likely to contribute to more employee satisfaction and less staff turnover. These benefits of MRP may contribute to a more productive workplace and improved patient care and safety (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002). Furthermore, MRP or other mindfulness-based interventions should be included in the curriculum of prelicensure nursing programs to minimize maladaptive coping strategies and encourage adaptive coping among recently graduated nurses entering the acute care work environment.
Applying Research to Practice
The study findings have a number of implications for nursing practice within healthcare systems that are tasked with improving patient outcomes and satisfaction while containing costs (Kutney-Lee et al., 2009; McHugh, Kutney-Lee, Cimiotti, Sloane, & Aiken, 2011). Reducing burnout and stress of conscience through health care workers using mantram may translate to improved teamwork and employee satisfaction, and reduced staff turnover, overtime, patient event reports, and hospital acquired infections. These benefits of mantram may contribute to healthy work environments and improved patient care and safety (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002). Further, the Mantram Repetition Program or other mindful interventions could be included in the curriculum of prelicensure nursing programs to minimize maladaptive coping strategies and encourage adaptive coping among health care workers.
Study Hypotheses
H1: A structured Internet-delivered MRP will reduce burnout among health care workers within the VA.
H2: A structured Internet-delivered MRP will reduce stress of conscience among health care workers within the VA.
H3: Health care workers within the VA who practiced meditation will have a different response to the MRP in regard to burnout than the health care workers within the VA who had not practiced meditation.
H4: Health care workers within the VA who practiced meditation will have a different response to the MRP in regard to stress of conscious than the health care workers within the VA who had not practiced meditation.
Program Topics
Class 1 Introduction to Mantram Repetition
Class 2 How to Choose, Use, and Track Mantram Practice
Class 3 The Stress Response and Mantram Repetition
Class 4 Slowing Down
Class 5 One-Pointed Attention
Class 6 Putting It All Together
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Sheryl Leary is a nurse researcher at the Veterans Administration San Diego Healthcare System.
Kimberly Weingart is a clinical psychologist and works as a Health Science Specialist in research at the Veterans Administration San Diego Healthcare System and is a Health Sciences Assistant Clinical Professor at the University California San Diego.
Robert Topp is the Patricia A. Chin Nursing Research Endowed Professor at the Hahn School of Nursing and Health Science and Beyster Institute for Nursing Research, University of San Diego.
Jill Bormann is Associate Nurse Executive/Research at the Veterans Administration San Diego Healthcare System, VA Center of Excellence for Stress and Mental Health and Adjunct Clinical Professor at the Hahn School of Nursing and Health Science and Beyster Institute for Nursing Research, University of San Diego.