
Abstract
Influenza has a significant impact on the health of Americans and the U.S. economy. Annual influenza immunization can decrease the burden of influenza-related illnesses for both employees and employers. This project evaluated a nurse practitioner–led intervention to increase influenza immunization rates among retail employees from August through December of the 2015-2016 influenza season. The sample included employees from retail locations with on-site convenience care clinics staffed by nurse practitioners. This quality improvement project used a pre–post implementation evaluation design and compared influenza immunization rates of employees, before and after an intervention, at one worksite, and influenza immunization rates of employees, who did not receive the same intervention, at a comparison site. The intervention site employees were immunized at a higher rate than employees at the comparison site. Interventions, including health care professional–led education, program promotion, on-site access to and no-cost immunizations, choice of immunization delivery, and incentives, should be considered to increase immunization rates among employees.
The economic burden of influenza-related illnesses for employers totaled US $30.4 billion during the 2012-2013 influenza season (Walgreens 2013 Flu Impact Report, 2013). Employees infected with the influenza virus are less productive and more at risk for absenteeism. On average, American employees missed 3 days of work during the 2012-2013 flu season, and the estimated combined loss in wages for employees was approximately US $8.5 billion (Walgreens 2013 Flu Impact Report, 2013). During the 2008-2009 pandemic flu season, influenza-associated employer costs increased by 400% (Karve, Misurski, Meier, & Davis, 2013). Costs associated with influenza vary from season to season, but have been increasing overall for employers (Karve et al., 2013).
In addition to economic impact, influenza has an even greater impact on health care utilization, and U.S. morbidity and mortality due to vaccine-preventable diseases (Reed et al., 2015). During the 2010-2011 influenza season through the 2012-2013 flu seasons, influenza-associated hospitalizations increased from an estimated 115,000 to 630,000 and influenza-associated mortality increased from 5,000 to 27,000 deaths in the United States (Reed et al., 2015). The annual uptake of influenza immunizations by Americans is a valuable health promotion action and can potentially eradicate the serious impact and consequences of the virus. The Centers for Disease Control and Prevention (CDC; 2015a) conduct influenza immunization effectiveness studies each season and estimate that the effectiveness of the immunization ranges from 10% to 60%. Even with a decrease in the effectiveness of the influenza immunization during the 2014-2015 flu season, the immunization resulted in fewer visits to health care providers due to influenza-related illness by 23% for at-risk Americans of all ages (CDC, 2015a).
Evidence-Based Literature Review and Synthesis
The evidence suggests that a multicomponent approach to increase influenza immunization rates of employees is needed. The following components have been shown to be effective: education, program promotion, improved access, no cost, choice of immunization delivery, and an incentive (Stathopoulou & Skourti, 2010). Education alone, or in combination with program promotional materials, without other interventions (e.g., offering immunizations at no cost, on-site, and with incentive) resulted in minimal changes in influenza immunization rates (Lam, Chambers, Macdougall, & Mccarthy, 2010). These research findings also recommended that the educational component of these programs should focus on the benefits and effectiveness of immunization.
Among studies that included an educational component, influenza immunization rates were shown to increase when health care professionals delivered the education (Abramson, Avni, Levi, & Miskin, 2010; Nicholson, Hayes, & Bennett, 2009). For example, when a physician delivered an educational lecture on influenza immunization to employees in a primary care setting, the rate of influenza immunization increased to 52.8% in the intervention group compared with only 26.5% in the control group (Abramson et al., 2010). On hospital units where nurses delivered information about influenza immunization, influenza immunization rates were 20% higher compared with units that did not have nurses as educators (Nicholson et al., 2009). A survey of industrial employees from U.S. manufacturing facilities that focused on their knowledge and beliefs about influenza showed respondents wanted vaccine information and advice from a health care provider prior to receiving the immunization (Ofstead et al., 2013).
In addition to education, offering an incentive for immunization uptake has been shown to increase influenza immunization rates. The combination of education, an on-site vaccine day, and an incentive (e.g., $25 deposited into employees’ health savings accounts) increased influenza immunization rates among industrial employees at two U.S. manufacturing facilities to 51% and 63%, respectively (Ofstead et al., 2013). In addition, research has shown that offering a choice of immunization delivery is beneficial in increasing uptake. Health care workers’ responses to an influenza immunization questionnaire showed that these workers were less likely to consent to immunization if only an injectable option was available (Lin et al., 2010). An intervention that combined program promotion, immunization delivery choice, and incentive (e.g., $5 gift card) was effective in increasing vaccine coverage of workers from 53 U.S. companies with vaccine clinics from 39% to 46% (Norwalk et al., 2010).
The implementation of interventions to increase annual immunization uptake and decrease the financial burden of influenza for employers and health risk for retail employees are necessary. Retailers with on-site clinics offer an ideal setting for the implementation of these interventions. A retail location in Durham, North Carolina, with an on-site clinic staffed with nurse practitioners was chosen for a project aimed at increasing the rate of annual employee influenza immunization uptake. The retailer employed an average of 300 employees each year. During the 2014-2015 influenza season, 97 of these employees received their annual influenza immunization at the on-site clinic. Based on the average number of annual employees, the corresponding influenza immunization rate was approximately 32%. This rate is low compared to the national influenza immunization rate of 46% at the end of the 2014-2015 flu season (CDC, 2015b).
Purpose of the Project
The purpose of the project was to evaluate a nurse practitioner–led evidence-based intervention to increase annual influenza immunization rates among employees at a retail location with a clinic during the 2015-2016 influenza season, August through December. The aims of the proposed project were to (a) achieve an employee influenza immunization rate of at least 50%, (b) evaluate the relationship between employees’ exposure to a nurse practitioner–led influenza immunization education session and distribution of promotional materials and their decision to consent to immunization, and (c) compare influenza immunization rates among employees working in two similar settings, one with a nurse practitioner–led educational intervention and one that only advertised influenza immunizations, that offered influenza immunization on-site, and that offered immunizations at no cost to employees.
Method
This quality improvement project used a pre–post implementation evaluation design and compared influenza immunization rates of employees before and after an intervention at a designated site, and influenza immunization rates between a similar comparison site that did not receive the same intervention components.
Organizational Setting and Study Sample
Two retail locations in the same city with on-site clinics, approximately 6 miles from each other, were compared. Both clinics employed nurse practitioners and clinical support staff and were open 7 days a week from 9 a.m. to 8 p.m. on weekdays and 9 a.m. to 4 p.m. on weekends. The intervention site employed an average of 260 employees during the project implementation year and the year prior. The comparison site employed an average of 305 employees during this same period. This average census included seasonal workers employed during the months of October through December due to increased staffing needs during the holiday season. The convenience sample included all adults, aged 18 years and older, who were employed at the retail locations during the months of August 2015 through December 2015.
Description of the Intervention
Based on the literature, the intervention had multiple components: free immunization, on-site influenza immunization with a choice of immunization delivery (injectable or intranasal) and a gift card and gift bag as incentives for immunization uptake. Promotional materials (i.e., posters and flyers) indicating the availability of the immunization and encouraging immunization were created for display at the on-site clinic and retail location. Nurse practitioners provided education on the benefits of influenza immunization to the employees at one site. Stickers indicating receipt of immunization (see Appendix A) and an incentive were distributed to all employees who were immunized at the on-site clinic.
In addition, a six-item questionnaire was distributed to employees to evaluate the relationship between employees’ exposure to a nurse practitioner–led influenza immunization education session and distribution of promotional materials and their decision to be immunized.
Implementation Plan
Promotional posters advertised immunization availability and promoted uptake; these posters were funded by corporate management and displayed at both the intervention and comparison sites. As part of an employee benefit, injectable influenza immunizations were offered at no cost to all employees at both sites during the months of August 2015 through December 2015. Intranasal immunizations were offered and administered only during the month of August due to a supply shortage from manufacturers. Immunizations were administered on-site by nurse practitioners during clinic hours. Extended clinic hours at the intervention site were offered, once for a 3-hour period, in October for employees who worked shifts outside of the normal operating hours.
At the intervention site, nurse practitioners held education sessions with employees at pre- or postshift meetings and new employee orientations, reviewing a two-sided factsheet from the CDC on the benefits and effectiveness of influenza immunization. Clinic support staff at the intervention site distributed incentives, assembled and stored at the clinic, to all employees who were immunized. This incentive included a gift card for a free entrée from a restaurant franchise, a bottle of water and a granola bar, flavored water mix, mints, and lip balm and hand sanitizer labeled with the company’s logo. The incentive was funded by the clinic’s budget lines for health promotion and clinic advertising. The total cost of the incentive per employee was $5.66 (i.e., $2.43 per gift bag, $0.18 per bottle of water, and $3.05 per gift card). In addition, all employees immunized were encouraged to wear the sticker indicating receipt of the influenza immunization downloaded from the CDC website.
Questionnaires were distributed to employees and collected by the clinic support staff at the end of the project period. All employees who returned completed questionnaires received a gift card for a free entrée donated by a neighboring restaurant franchise. Employees, who initially received a gift card as incentive for immunization uptake, received an additional gift card for returning a completed questionnaire.
Assessment and Measures
The desired outcome of the project was an increase in the number of influenza immunizations administered to employees at the on-site clinic during the project period. The rate of influenza immunization was defined as the number of influenza immunizations administered to employees at the on-site clinic divided by the average total number of employees at the site during the project period. Employees who received an influenza immunization at a site other than the on-site clinic were not included in the influenza immunization rate for this project.
The six-item questionnaire was developed by the Project Investigator based on synthesis of the evidence, the project setting, population, and study aims to assess the fidelity of the intervention. Employees provided responses by checking corresponding boxes for each question. Responses were provided anonymously by employees and analyzed by adding the number of responses for each question and dividing it by the total number of returned questionnaires to determine percentages.
Data Collection Plan
Nurse practitioners ordered, administered, and documented influenza immunization administration in Athena, the electronic medical record (EMR) used by all providers at the on-site clinic. The EMR was queried at the end of the project period to determine how many immunizations were administered to employees at both clinic sites. The number of employee influenza immunizations was extracted based on billing code which was entered by clinic support staff and confirmed by providers. The regional director of human resources determined the average total number of employees at each location for the project period. Any identifiers were removed and only the number of employees was provided for analysis.
The questionnaires were randomly distributed to employees by clinic support staff at the intervention site. Employees were encouraged to complete the questionnaire and return it anonymously to the clinic by placing it in a designated envelope. Completed questionnaires without any identifying employee information were collected for analysis by the Project Investigator.
Results
The average number of employees at the intervention site during the project period was 246. Of these 246 employees, 91 received influenza immunizations at the on-site clinic, an influenza immunization rate of 45%. At the comparison site, the average number of employees during the project period was 290. Of these 290 employees, only 32% received influenza immunizations at the on-site clinic. As shown in Table 1, comparison of the two sites showed a difference in influenza immunization rates with the intervention site demonstrating a greater rate of immunization.
Comparison of Data From Clinic Sites
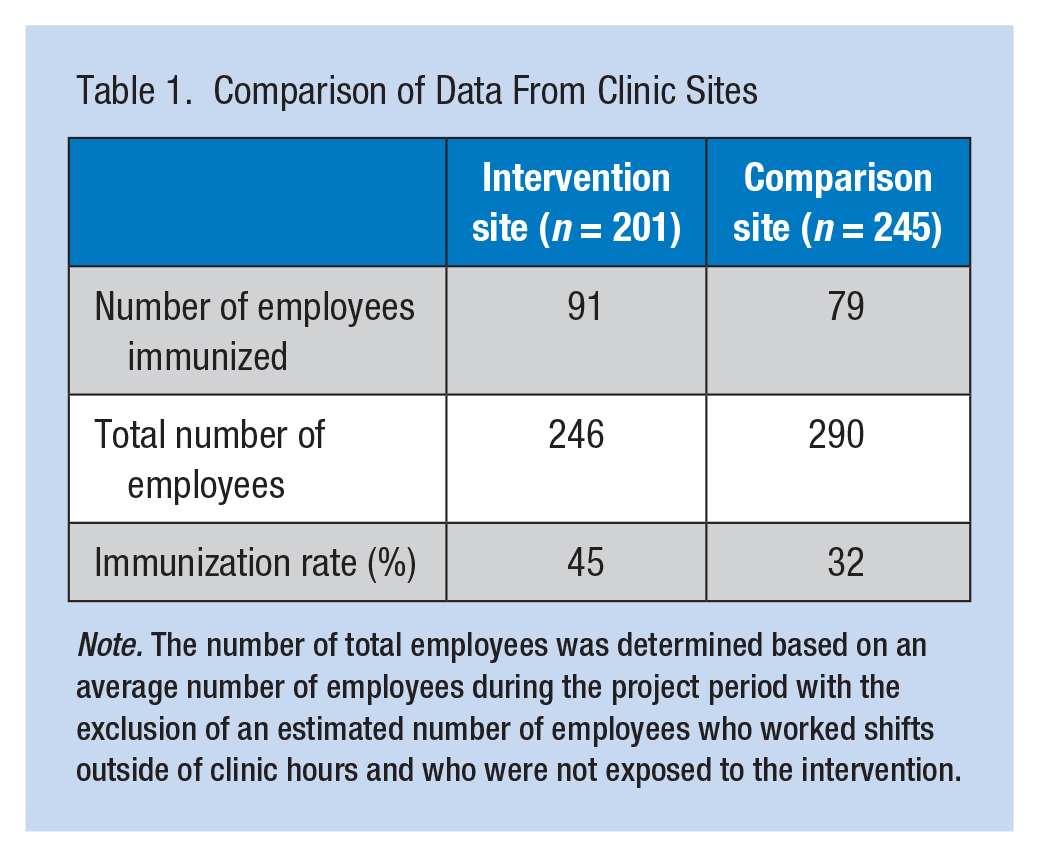
Note. The number of total employees was determined based on an average number of employees during the project period with the exclusion of an estimated number of employees who worked shifts outside of clinic hours and who were not exposed to the intervention.
Table 2 displays the results of the questionnaires distributed to employees at the intervention site. One hundred twenty-one questionnaires were returned, resulting in a response rate of 49%. The majority of respondents reported they had received education from a nurse practitioner (83%) and reviewed the handout (74%) on the benefits of influenza immunization.
Results From Employee Flu Vaccine Questionnaire (N = 121 Respondents)
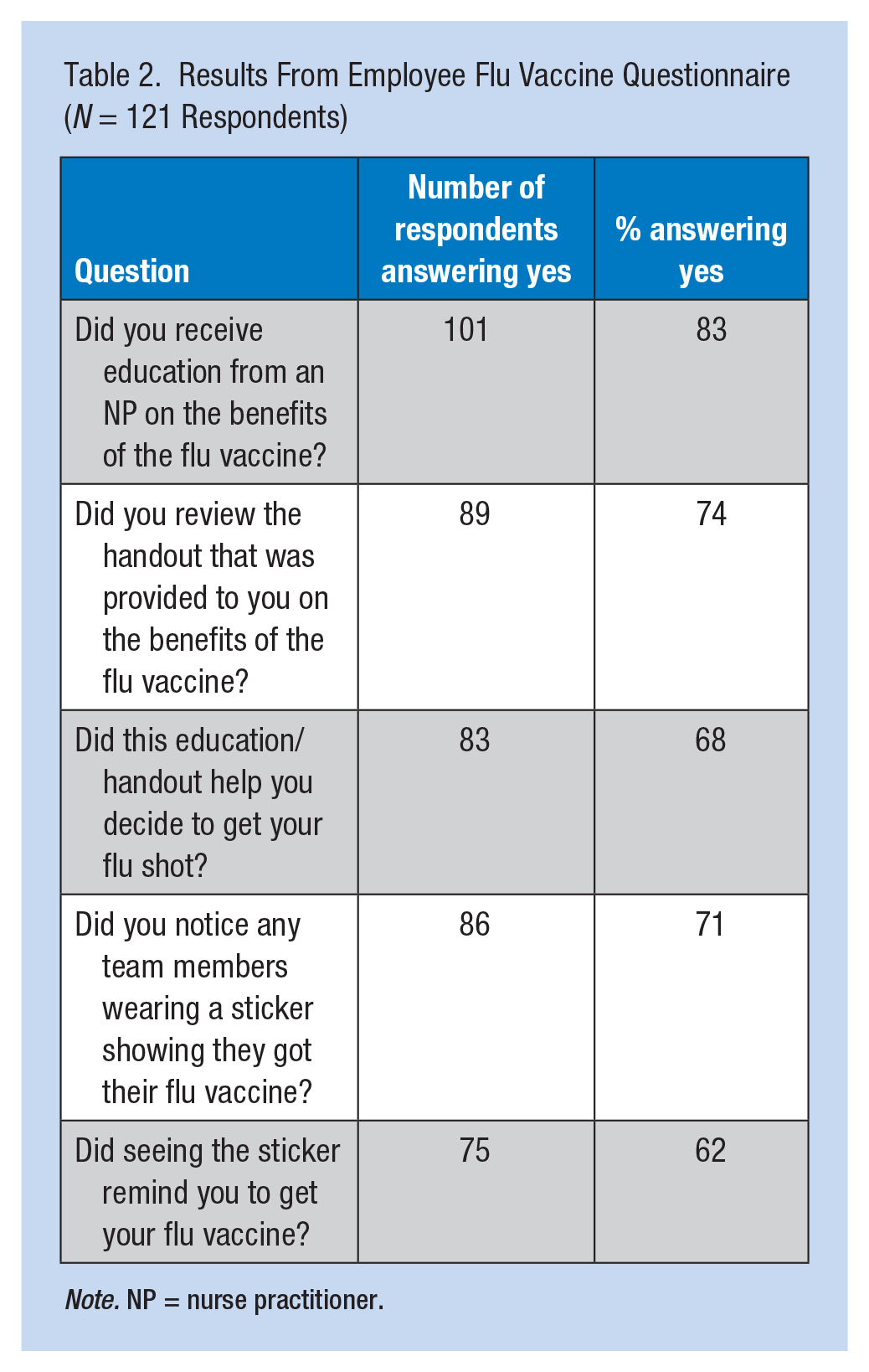
Note. NP = nurse practitioner.
In addition, 68% of respondents indicated that the education and handout influenced their decision to receive an influenza immunization. In regard to the distribution of promotional stickers, the majority of respondents (71%) reported noticing others wearing stickers that indicated receipt of immunizations. Seeing the sticker reminded 62% of respondents to seek influenza immunization.
As shown in Table 3, the most common setting in which respondents received influenza immunizations was the on-site clinic (65%). The remaining percentage of respondents either did not receive an immunization (23%) or received it at another location (12%) and were not included in the overall influenza immunization rate.
Location of Immunization Administration (n = 121 Respondents)
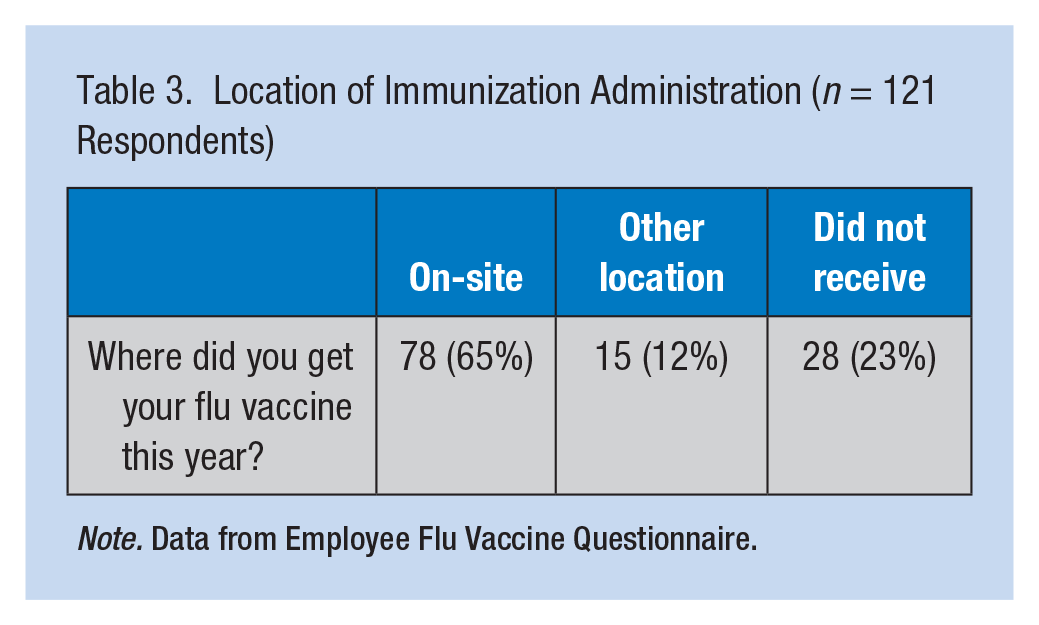
Note. Data from Employee Flu Vaccine Questionnaire.
Discussion
The intervention site had a 35% influenza immunization rate for the 2014-2015 season, which increased by 2% to 37% during the 2015-2016 season post intervention implementation. Despite an evidence-based multicomponent intervention, influenza immunization rates in this setting remained lower than the national average. However, the influenza immunization rate was higher at the intervention site than the comparison site.
In regard to the components of the intervention, a shortage of intranasal influenza vaccine affected employees’ administration options. According to a similar study, lack of delivery choice may have affected immunization uptake for employees who would have consented to needleless immunization if available during the project period (Lin et al., 2010).
Based on the analysis of responses from the completed questionnaires, nurse practitioners successfully distributed and discussed the CDC educational handout on the benefits of influenza immunization with employees at the intervention site, and clinic support staff distributed promotional stickers to employees who received immunizations. Questionnaire responses also indicated that employees reviewed the handout and reported it influenced their decisions to consent to immunization at the intervention site. Furthermore, responses indicated that seeing stickers had less effect on employees’ decisions to be immunized than nurse practitioner education and handout distribution.
Project findings are consistent with other studies that suggest active program promotion and education by health care professionals have a greater impact on increasing immunization uptake than passive program promotion (Abramson et al., 2010; Nicholson et al., 2009). Similar to other studies, the project found that education focused on the benefits of immunization is effective in influencing individuals to be immunized (Lam et al., 2010). The on-site clinic was the source of most immunizations, although some employees did seek immunizations at other locations.
Limitations
In general, other influences on employees’ decisions to receive influenza immunizations at both sites were not controlled in this study. Employees could have been exposed to education or program promotion from other sources (e.g., another health care provider, the media, pharmacist, friend, or colleague). During the study period, employees in the sample could have been lost due to changing employers or being absent from work. An insufficient supply of intranasal influenza immunizations affected immunization choice during the entire intervention period, which could have increased immunization uptake (Lin et al., 2010). This shortage may have affected the overall employee immunization rate as employees who preferred the intranasal method of vaccination may not have been immunized. Furthermore, employees who worked shifts that did not coincide with scheduled clinic hours were not exposed to the intervention and were not included in the rate calculation when comparing the two sites.
Despite offering an incentive for questionnaire completion, which has shown to increase completion rates (Ofstead et al., 2013), a sampling bias based on the questionnaire response rate of 49% resulted. In addition, responses could not be collected from employees who were not present during the 2-week time period of questionnaire distribution nor who worked shifts other than ones that corresponded with clinic hours. Some questionnaires were distributed to employees during their shifts which made completing it while engaging in other tasks difficult. These retail employees have limited or no access to company email, which made distribution of the questionnaire in an electronic format challenging.
In addition, the multicomponent intervention did not allow the researchers to determine the effects of specific components of the intervention on immunization rate. However, evidence indicates that multicomponent interventions increase influenza immunization rates and that implementing single component interventions is not as effective (Stathopoulou & Skourti, 2010). Therefore, health care professional–led education, program promotion, improved access to and no cost for the immunization, choice of immunization delivery method, and an incentive should all be included in an intervention program aimed at increasing influenza immunization rates.
Implications for Practice
Employers interested in maintaining employee health and productivity should consider multicomponent interventions to increase annual influenza immunization rates. A feasible component of an intervention to increase influenza immunization rates may include the discussion and delivery of a CDC-developed handout on the benefits of annual influenza immunization. Including the distribution of a promotional sticker to a program may remind other employees to seek immunizations. In addition, regularly offering extended clinic hours for employees who work shifts could increase uptake.
On-site health care professionals, such as occupational health nurses or occupational health nurse practitioners, offer a valuable resource to employers for delivering health education and promoting wellness to their employees. Using health care professionals in this role could improve employee influenza immunization rates. In addition, ensuring that interventions are implemented by health care professionals and including employees from all shifts appears beneficial.
Employees working in retail settings are at increased risk for influenza exposure due to their daily interactions with consumers and exchange of currency. However, the rates of annual influenza immunization in this population remain low. The American Academy of Pediatrics (AAP; 2015) issued a policy statement on mandatory employee immunization requirements, stating, “mandatory influenza immunization for all health care personnel is ethical, just, and necessary to improve patient safety” (p. 1). Many health care employers have elected to require annual influenza immunization to reduce influenza infection and protect patients (AAP, 2015). Retail employers may consider mandatory immunization policies to increase influenza immunization rates among employees if multicomponent approaches, which include the components implemented as part of this project, do not increase influenza immunization rates. This requirement in the health care setting has resulted in an influenza immunization rate of 75% nationwide (AAP, 2015).
Conclusion
Multicomponent interventions led by nurse practitioners in retail settings with clinics increase influenza immunization rates among employees and should be available to all retail workers regardless of shift and location. Determining barriers to immunization uptake among the retail employee population, particularly in regard to individual employees’ beliefs about immunizations, is needed. Evidence that increasing employee influenza immunization uptake will result in a more productive workforce and lower employer costs for employee illness is needed. In addition, identifying the effectiveness of each individual component of the multicomponent intervention would determine the need for each component. The use of a control clinic to establish a statistically significant comparison between two occupational clinic sites would also strengthen the findings.
In Summary
Retail employees are at increased risk for exposure to the influenza virus due to their daily interactions with consumers and exchange of currency.
Health care professionals, such as occupational health nurses or occupational health nurse practitioners, offer valuable resources for employers by delivering vaccine education and promoting uptake to their employees.
Retail employers interested in maintaining employee health and productivity should consider implementing multicomponent interventions to increase annual influenza immunization uptake among their employees.
Interventions should be directed at employees who work all shifts and include: health care professional–led education, program promotion, on-site access to and free immunizations, choice of immunization delivery method, and an incentive for uptake.
Mandatory immunization requirements may be needed to increase rates among employees.
Footnotes
Appendix
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Leigh Montejo is a doctor of nursing practice student at Duke University School of Nursing with an interest in health promotion and wellness. She is a certified family nurse practitioner providing patient care at a convenience care clinic.
Rachel Richesson is an associate professor of health informatics at the Duke University School of Nursing. She holds a graduate degree in population and community health and a doctorate in health informatics.
B. Iris Padilla is a professor at Duke University School of Nursing with an interest in diabetes self-care, adherence, co-morbid depression, insulin initiation and education.
Michael E. Zychowicz is a professor and director of the MSN Program at Duke University School of Nursing.
Crystal Hambley is a certified nurse practitioner providing patient care at a convenience care clinic and graduate of Duke University School of Nursing.