
Abstract
Vertigo is a disorder that affects equilibrium. Symptoms include a loss of balance with nausea and vomiting. Employees diagnosed with vertigo can return to work safely; however, they may need workplace restrictions and accommodation as symptoms may persist for months. This article reviews the evaluation and treatment of vertigo with back-to-work recommendations.
Keywords
A 56-year-old female, HH, presented to the employee health clinic with progressive symptoms of “the room is spinning,” with accompanying nausea and vomiting. HH was an associate professor at a local state university and stated that when she woke up that morning, she had some mild difficulty walking due to “loss of balance” but was able to drive to work. As the morning progressed, her symptoms of disequilibrium became worse, and she decided to seek assistance at employee health. HH denied any loss of consciousness but was concerned that she had vertigo. HH stated that when she was in the Navy, she had seen sailors with “sea sicknesses” and had the same symptoms. The employee health nurse called HH’s primary care provider and made a same-day appointment. HH was unable to stand and requested that her husband drive her to the appointment because she felt unsafe driving.
Review of systems was negative for symptoms of ear pain or fullness, headaches, tinnitus, hearing loss, or a history of upper respiratory infections. HH denied any allergies and was currently taking an 81 mg baby aspirin for cardiovascular disease prophylaxis. She also denied any history of alcohol or nicotine use but drinks two cups of caffeinated coffee in the morning. HH did report a car accident about 6 months ago and was unsure if she had lost consciousness. She had a negative computed tomography (CT) scan at that time; she was diagnosed with a cervical strain, which resolved in 2 weeks.
Physical examination by her primary care provider revealed a normal ear examination. However, bilateral nystagmus was present as was an increased sway with Romberg. The Dix–Hallpike maneuver was positive. Weber and Rinne tests were normal. Orthostatic blood pressures were negative, which ruled out syncope. Heart examination did not reveal any murmurs or extra heart sounds, and carotid findings were normal. Due to her history of car accident, the primary care provider suspected vertigo.
A magnetic resonance imaging (MRI) with and without contrast was ordered to rule out primary causes of vertigo (e.g., acoustic neuroma or multiple sclerosis). Electronystagmography (ENG), a test for the etiology of nystagmus, was negative for a central cause but positive for a peripheral cause of vertigo.
HH was diagnosed with benign paroxysmal positional vertigo (BPPV). She was given sick leave for 1 month but had weekly appointments with her primary care provider and case management by the occupational health nurse. HH attended a physical therapy consult for gait and balance training with canalith repositioning. She was prescribed a scheduled dose of scopolamine transdermal patch for vertigo symptoms and Zofran as needed for nausea and vomiting.
After 1 month, HH returned to work with restrictions. She was not allowed to lift, push, or pull more than 25 pounds; bend; use awkward positions; or reach above her head. She was advised to change positions slowly and avoid fast-paced work assignments. It was recommended that HH not operate a motor vehicle or machinery.
Vertigo
Vertigo presents with illusory movement. It is a disorder of the inner ear, although vertigo may also be associated with diseases of the central nervous system. Employees may refer to vertigo as either motion sickness or sea sickness because it is characterized by a transient loss of balance with a spinning sensation. It may be accompanied by nausea and vomiting. Vertigo may become worse with sudden rolling or tilting of the head. Vertigo occurs when an imbalance of fluid or calcium particles (otoliths) occurs in the vestibular system, which includes the labyrinth and vestibular nerve.
The vestibular system consists of the semicircular canals and the otolith organs in the inner ear. Vertigo is categorized by two etiologies: peripheral and central. Peripheral vertigo is an inner ear disorder and central vertigo is a central nervous system disorder (Table 1). Diagnosticians must differentiate between vertigo, dizziness, and syncope.
Differential Diagnosis of Vertigo
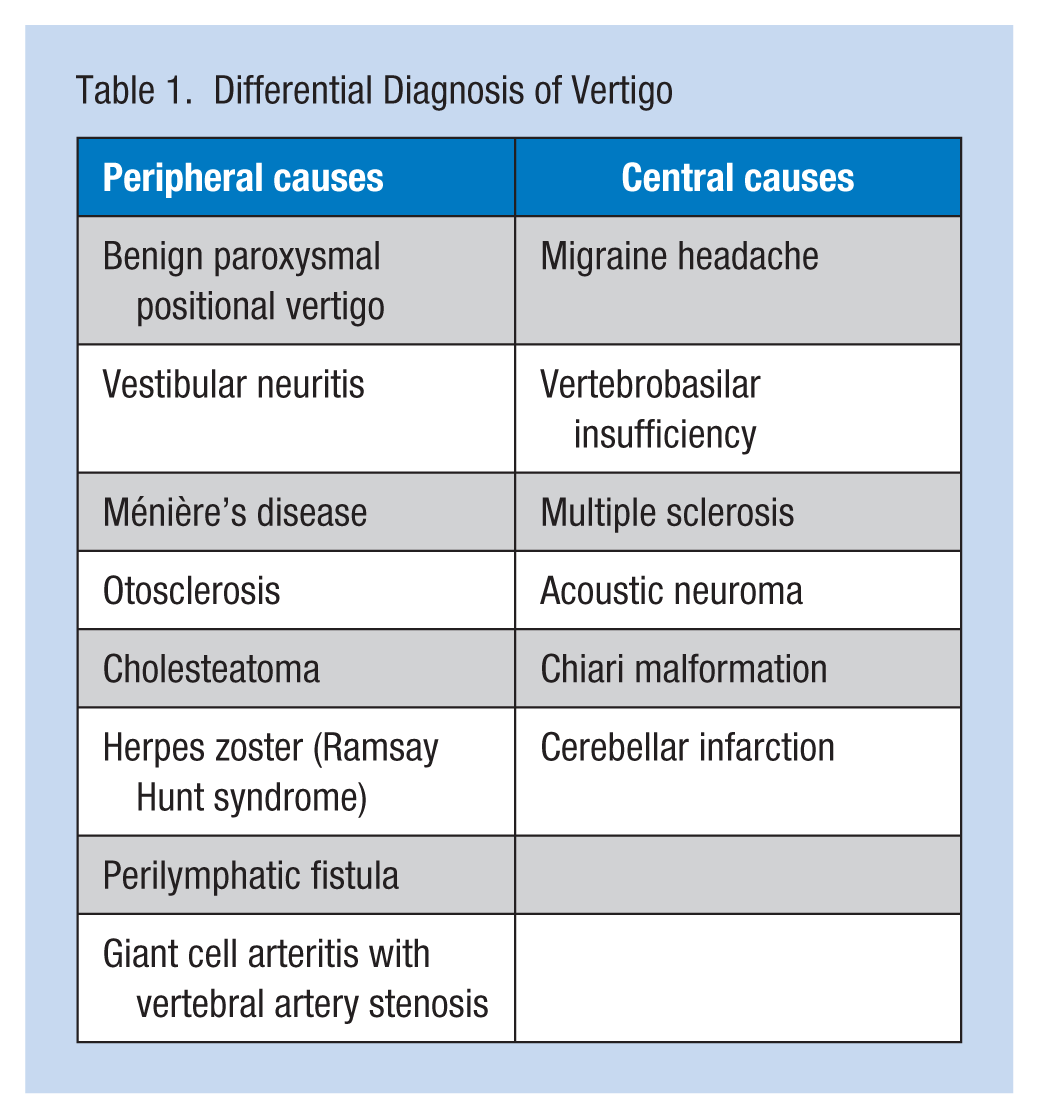
Loss of consciousness is not associated with vertigo. Hearing loss and tinnitus may be associated with inner ear disorders, and should be further evaluated for Ménière’s disease or acoustic neuroma. Vertigo with cranial nerve involvement and cerebellar findings are associated with central vertigo disorders. Vertigo with headache and ataxia requires prompt attention to rule out stroke or tumors. The symptoms of central vertigo are slow, persistent, and spontaneous without stimulus; symptoms of peripheral vestibular disorders are usually sudden and may be temporary lasting from 24 to 48 hours (National Clearinghouse Guidelines, 2014).
BPPV
Benign paroxysmal positional vertigo may be episodic, lasting seconds or minutes. These episodes may spontaneously disappear. Quick, positional changes of the body or head may precipitate this type of vertigo. The employee may also experience nausea and vomiting, with nausea persisting even when the symptoms of vertigo have been relieved. Workers may report balance disturbances that increase their risk for falls and other injuries. Benign paroxysmal positional vertigo affects mostly females, and the incidence increases after the age of 50. These employees may have a history of concussion or other head trauma.
The etiology of BPPV involves the labyrinth system, which is located in the inner ear and consists of the vestibule, semicircular canal, and cochlea. Otoliths (calcium particles) that are found in the labyrinth may be dislodged due to trauma and move into the semicircular canals causing the symptoms of vertigo. Endolymph, fluid located in the semicircular canals, becomes displaced and moves even when the head is motionless, contributing to the sensation of vertigo. Nausea and vomiting are the result of stimulation of the vestibular apparatus and other neurotransmitter receptors such as dopamine, serotonin, histamine, acetylcholine, and substance P.
Evaluation
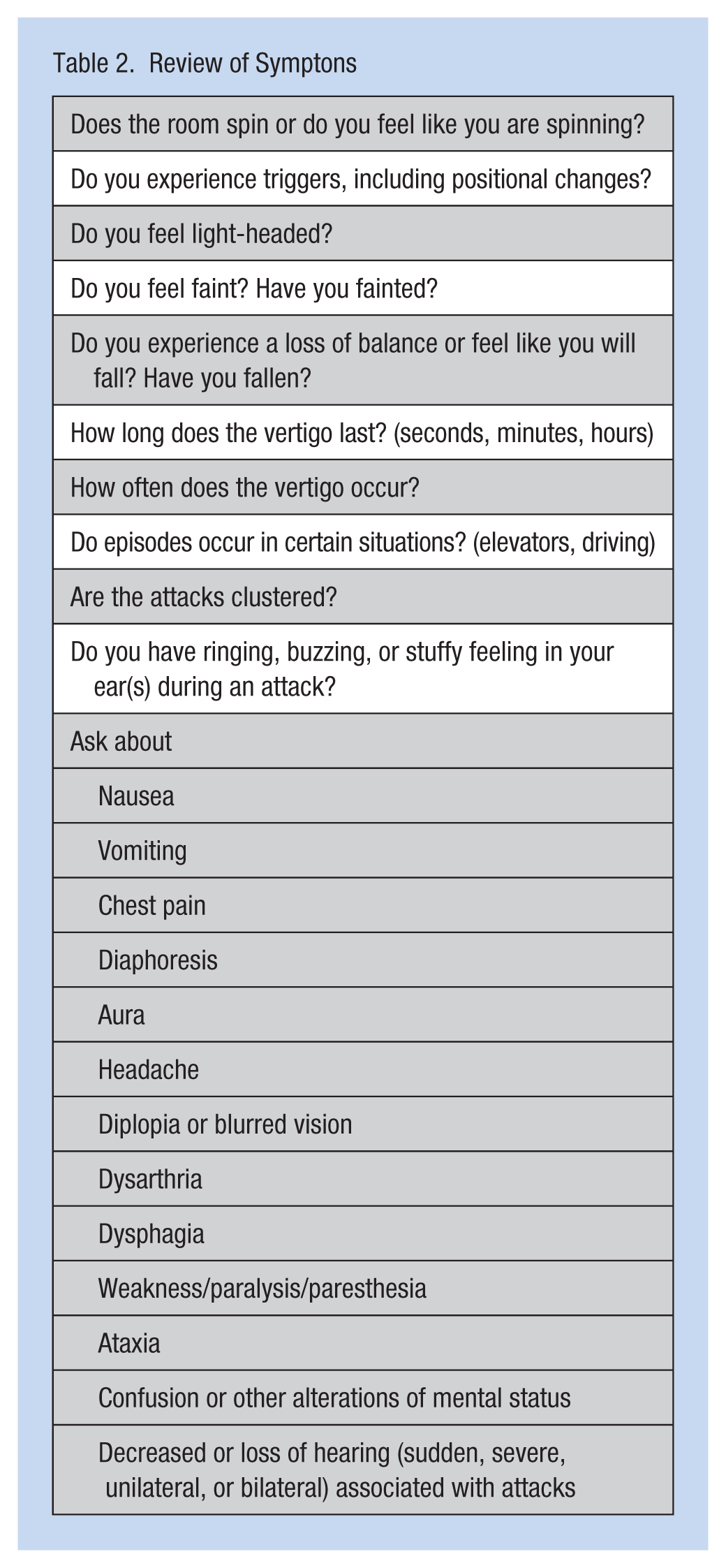
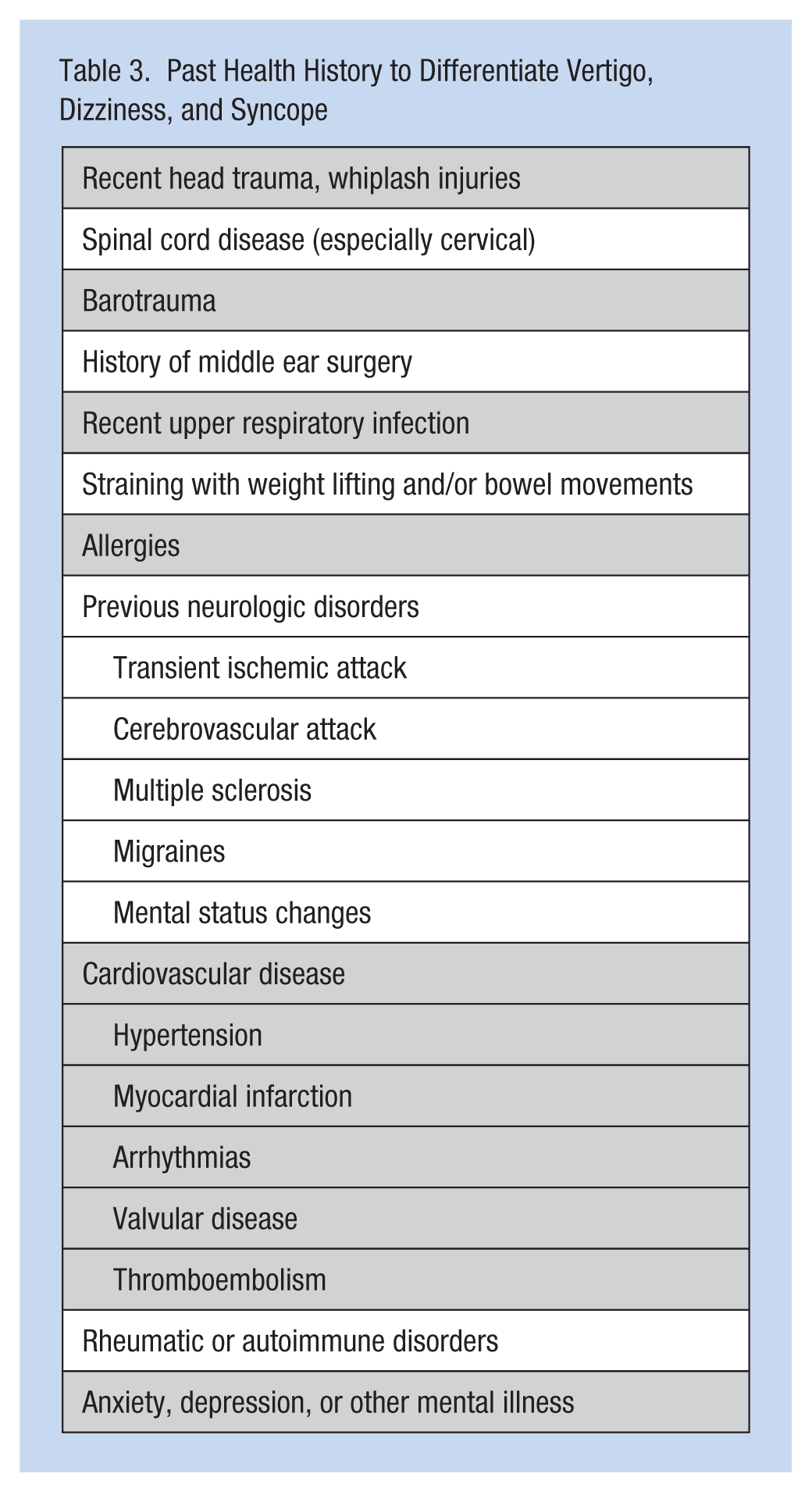
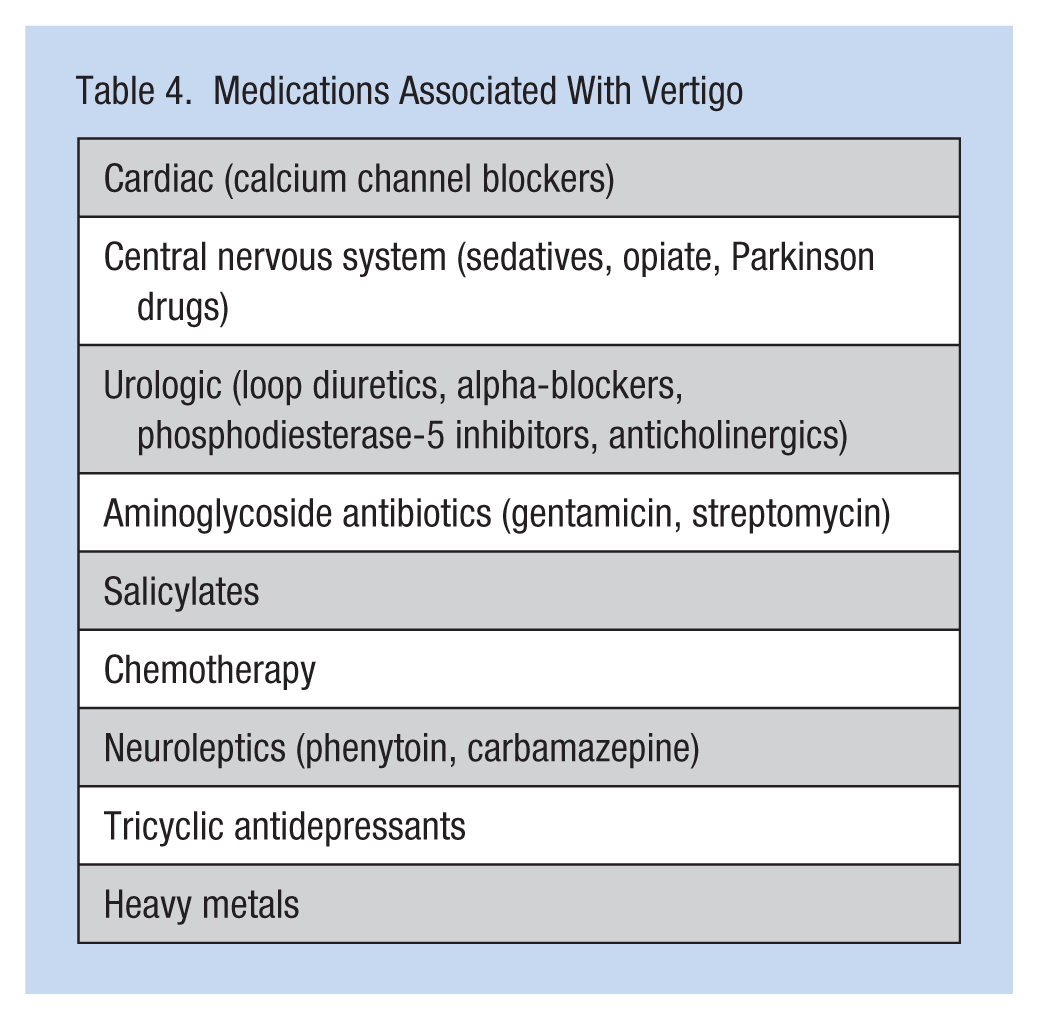
Workers’ symptoms and their health histories should be evaluated according to National Clearinghouse Guidelines (Tables 2 and 3). Their history of caffeine, tobacco, alcohol, and recreational drug use should also be documented. Occupational exposures (e.g., mercury and carbon monoxide) should be investigated. Medications (Table 4) may also be associated with vertigo (Chimirri et al., 2013).
Review of Symptons
Past Health History to Differentiate Vertigo, Dizziness, and Syncope
Medications Associated With Vertigo
A complete physical examination that particularly focuses on the ear, nose, and throat should be completed; a hearing test should be offered if hearing loss is reported. Neurological and cardiovascular examinations with assessment of orthostatic blood pressures should also be completed. A complete blood count should rule out anemia and infection. A comprehensive metabolic panel including thyroid tests (thyroid-stimulating hormone [TSH], T3, T4) can rule out metabolic etiologies. Testing for rheumatoid disorders (e.g., Lyme disease) and syphilis may also be considered.
The Dix–Hallpike maneuver requires individuals to sit on an examination table; the health care provider turns the worker’s head 45 degrees to one side and then rapidly places the individual in a supine position while the head is hanging at a 20 degree angle over the edge of the examination table. The health care provider observes the individual’s eye movements for 30 seconds. The Dix–Hallpike maneuver is repeated with the head turned in the opposite direction.
The Dix–Hallpike test for nystagmus is an objective assessment for vertigo (Evren, Demirbilek, Elbistanl, Köktürk, & Celik, 2016). If nystagmus is present, the provider must determine if the nystagmus has central or peripheral etiology. Vertical nystagmus and horizontal direction–changing nystagmus are signs of central nervous system involvement; unidirectional horizontal nystagmus can have either peripheral or central nervous system etiology. This maneuver can be performed by nurses, physicians, or physical therapists. Caution is advised for those workers with cervical spine disorders or carotid artery disease.
Diagnostic tests include an MRI of the head, with and without contrast, to determine central nervous system or peripheral or inner ear disorders (National Clearinghouse Guidelines, 2014). Electronystagmography can determine the central versus peripheral etiology of nystagmus (Gupta & Mundra, 2015). An ENG measures function of the oculomotor and vestibular systems via positional testing and stimulation of the vestibular system. Oculomotor includes saccades-quick, rapid eye movement and pursuit/gaze testing that requires workers’ eyes to focus and follow an object.
Interventions
Health care providers may consider consulting physician specialists. Neurologists may be considered when the etiology of vertigo is central. Otolaryngologists may be consulted for peripheral etiologies. Audiologists may conduct the hearing evaluation.
Physical therapists may be required for canalith repositioning and gait and balance training. Canalith repositioning, or Epley maneuver, is specifically offered for BPPV (Brasch, Ross, & Korownyk, 2015). It is speculated that workers with BPPV have calcium particles move from the semicircular canal into the inner ear. These calcium particles stimulate the vestibular system, thus provoking vertigo symptoms. Gait and balance training can adjust the response of the vestibular system to movements of the body.
Vestibular rehabilitation includes exercises that enable the worker to focus on a target without moving the head. The goal is to provide the central nervous system the spatial cues needed to judge the position of the head and body (Tjernstrom, Oz, & Klause, 2016), starting with slow exercises and progressing to fast-moving targets. These exercises are completed in various positions: standing or sitting. Physical therapy treatment may last for up to 6 to 8 weeks. Habituation exercises can be performed by the worker to become accustomed to specific sensations that may provoke vertigo. Balance training focuses on maintaining balance with diminished visual fields. Recommendations for an assistive device may also be evaluated.
Medications
The symptoms of vertigo are often managed by treating the underlying health problem (e.g., tumor resection for acoustic neuroma or antibiotic to treat an infection). Medications are used for the acute phase of vertigo.
One category of medications used to treat vertigo are H1 receptor antagonists. Meclizine and scopolamine are commonly prescribed medications in this category. These H1 receptor antagonists have antihistamine effects and anticholinergic properties that block muscarinic receptors. These medications depress labyrinth and vestibular stimulation and neurotransmitters associated with nausea. However, these medications have side effects (e.g., sedation and urinary retention). Long-term use may be associated with narrow-angle glaucoma.
If nausea and vomiting continue, medications (promethazine or odansetron) are prescribed. Promethazine, a H1 receptor antagonist, can be taken in addition to meclizine or scopolamine; however, caution with these medications is needed. Odansetron is a 5-HT3 receptor antagonist and may be a better alternative for treating nausea than promethazine because it does not affect muscarinic receptors. However, caution is again advised because of adverse effects (e.g., dizziness or prolonged QT interval). The medication blocks serotonin, decreasing stimulation of the vagus nerve; 5-HT3 receptor antagonists also block dopamine, histamine, and muscarinic receptors that may cause nausea.
Nursing Implications
Occupational health nurses ensure employees’ fitness for duty via comprehensive physical examinations prior to returning to work. Medication evaluation also should be noted. Intense case management should focus on safety precautions in the workplace.
Workplace Restrictions and Accommodations
Workplace accommodations should include job activities that do not require awkward head positions (e.g., head flexion and extension, reaching above head level that requires the head to flex in an extreme position). Ergonomic evaluations may be considered to reduce the need for quick awkward positioning. Medications may induce drowsiness and should be used with caution in the workplace. The use of these medications may increase employees’ risk for falls. Employees should avoid working with machinery. If permitted, an assistive device may be considered. Occupational health nurses should monitor noise levels; auditory stimulation may precipitate vertigo in susceptible employees (Pelegrin, Canuet, Rodriquez, & Morales, 2015). Some employees may find it difficult to concentrate, so they should be allowed rest periods as needed. It is recommended that employees fully recover from vertigo before driving because driving requires the abrupt turning of the head to check for blind spots.
Conclusion
Benign paroxysmal positional vertigo may be self-limiting or persist for months. The occupational health nurse must ensure that employees have safe work environments and monitor their health in collaboration with their primary care providers. Employees must have regular health and safety evaluations as they continue home exercise programs and medication regimes, reporting adverse side effects.
HH returned to work using a four-wheel walker with seat to travel to her classes. HH was allowed extra time to travel to classes and position her work station so that she could avoid moving her head up or down. She continued with physical therapy but discontinued her medications prior to returning to work, and reported to the occupational health nurse every 2 weeks with documentation of physical therapy progress and reports from her provider. HH reported resolution of her symptoms in 6 months.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann Regina Lurati is a nursing lecturer at California State University at Monterey Bay.