
Abstract
The health status of Jamaican workers was evaluated as a baseline for workplace health promotion interventions. Socio-demographic, health status, and lifestyle data were collected from 1,087 employees. Blood pressure, glucose and cholesterol levels, and body mass index were measured for study participants. The most common illness reported by the study participants was migraine headaches (16.0%), followed by hypertension (13.5%) and asthma (6.1%). Based on blood pressure measurements, 34.1% were pre-hypertensive (120-139/80-89 mmHg), 13.1% had Stage 1 hypertension (140-159/90-99 mmHg), and 2.3% Stage 2 hypertension (≥160/≥100 mmHg). Furthermore, 33% were overweight, 16.7% were obese, and 10% were extremely obese. Most (55.1%) of the study participants reported excessive fast-food consumption in the last 7 days. The high rates of obesity, hypertension, and fast-food consumption reported in this study emphasized the need for focused health promotion strategies. Universality across institutions presented an excellent opportunity for national workplace health intervention programs.
Jamaica, similar to other countries in the English-speaking Caribbean, is in epidemiological transition; the main causes of mortality and morbidity are no longer infectious diseases with the exception of HIV/AIDS but rather chronic non-communicable diseases (Ferguson, Tulloch-Reid, et al., 2011). This new epidemic has resulted in part from an increase in the prevalence of obesity associated with sedentary lifestyles, and a cultural tradition that favors obese women (Durazo-Arvizu et al., 2008; Ferguson, Tulloch-Reid, et al., 2011; Hospedales, Samuels, Cummings, Gollop, & Greene, 2011).
The burden of chronic non-communicable diseases in the English-speaking Caribbean is highest in the Americas and has resulted in regional governments’ commitment to reducing the epidemic (Hospedales et al., 2011; Samuels, Kirton, & Guerbert, 2014). One area that is likely to be affected by the change in morbidity and mortality etiology is the workplace, where unhealthy employees are reported to be less productive than their healthy counterparts although more randomized controlled clinical trials are needed (Dunet et al., 2008; Goetzel, Hawkins, Ozminkowski, & Wang, 2003; Pereira, Coombes, Comans, & Johnston, 2015). Furthermore, obesity has been associated with increased costs for employers due to absenteeism, occupational and non-occupational injuries, and chronic diseases (Goetzel et al., 2003; Neovius, Johansson, Kark, & Neovius, 2009; Xiang et al., 2005). Other lifestyle factors include smoking, unhealthy diet, and physical inactivity, which may be linked to coronary heart disease, stroke, and some cancers (Bauer, Briss, Goodman, & Bowman, 2014; Milton, Macniven, & Bauman, 2014)
Employers who promote healthy lifestyles among their employees benefit from lower health care costs and higher productivity. Furthermore, the workplace is an excellent site for health promotion activities because employees spend half of their waking hours at work and are a captive population (Dunet et al., 2008). These activities are part of a comprehensive public health strategy to improve adult health and quality of life through prevention of disease and promotion of healthy lifestyles.
Several population studies on the health of Jamaicans have estimated the point prevalence for chronic non-communicable disease risk factors (e.g., smoking and sexual practices; Durazo-Arvizu et al., 2008; Figueroa, Ward, Walters, Ashley, & Wilks, 2005). However, only a few studies have targeted the workplace and these have focused on the health sector (Jackson & Ashley, 2005; Lindo, McCaw-Binns, LaGrenade, Jackson, & Eldemire-Shearer, 2006).
Studies of the health of employed Jamaicans are needed to inform the design and implementation of workplace health promotion programs. Differences in the health profile of Jamaican employees may be based on their social and demographic characteristics and the type of company in which they are employed. Therefore, it may not be possible to introduce a single health promotion strategy in all Jamaican workplaces.
The aim of this study was to evaluate the health status of workers in Kingston, Jamaica. Specifically, the study was designed to determine the point prevalence of non-communicable diseases and associated risk behaviors reported by employees of public, private, and quasi-government employers.
Method
A descriptive cross-sectional study of 1,020 individuals employed by two government ministries, three private-sector companies, and a quasi-government agency was conducted in Kingston, Jamaica. The study was part of a larger investigation of commuting stress among office-based (i.e., managerial, administrative, support, and clerical) employees. Participants were divided into drivers and non-drivers because the mode of commuting was shown to have an effect on health and well-being (Künn-Nelen, 2015).
Data Collection
Data collection included two measurements of resting blood pressure, fasting blood glucose (FBG), and cholesterol. The height and weight of participants were also measured to calculate body mass index (BMI). Anthropometric and biomedical measurements were scheduled between 6:30 a.m. and 8:30 a.m. to avoid any disruption of the business day.
Sample
The total number of employed persons in the Kingston metropolitan area was estimated at 385,500 (Statistical Institute of Jamaica, 2007). To facilitate data collection from a sample of 1,087, large companies within a 10-km radius of downtown Kingston were stratified into government, quasi-government, and private-sector entities. Letters were sent to a random sample of 10% of them requesting permission to conduct the study in their respective institutions. These letters were followed by telephone calls and visits to the potential companies to determine which were willing to facilitate the study. Six companies agreed to participate in the study including the following:
Company 1P (private-sector firm with some government ownership interest),
Company 2P (local arm of a multinational utilities company),
Company 3Q (quasi-government institution),
Company 4G (government ministry),
Company 5G (government ministry), and
Company 6P (food manufacturing and distribution company).
Full-time employees at the above-mentioned companies were eligible to participate in the study. All employees were invited to participate in the study and those not eligible were excluded from the database. This method allowed a more amicable relationship with the study team and enhanced compliance in comparison with random selection of some study company workers. Persons employed in sales and/or other traveling jobs, part-time employees, those on vacation, and pregnant women were excluded from the study.
Instruments
Cholesterol and blood glucose were measured using Accutrend® Plus cholesterol meters and glucometers, which were calibrated to laboratory standards using samples from the Department of Pathology, University of the West Indies. Height and weight were measured using Seca 214 stadiometers (North Bend, WA, USA) and Tanita HD 351 scales (Arlington Heights, IL, USA), respectively. A structured pre-tested questionnaire was used to collect data on socio-demographics, health status, and lifestyle practices as well as stress levels experienced in the home and work environments. The Cronbach’s alpha internal consistency reliability coefficient for the instrument was .868. Data were analyzed using SPSS version 18 for Windows.
The study was approved by the Ethics Committee of the University of the West Indies/University Hospital of the West Indies and written informed consent was required prior to data collection.
Results
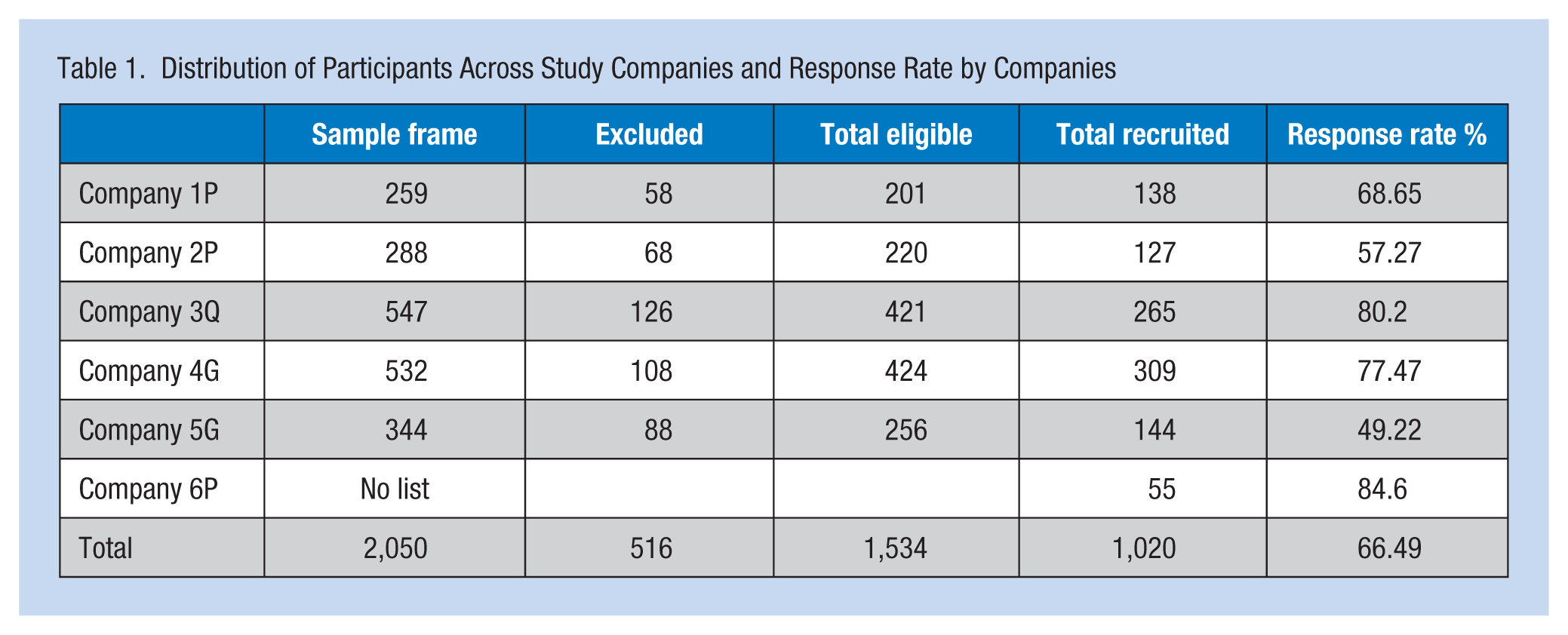
The total number of employees in each company and the number who participated in the study ranged from 547 in Company 3Q to 259 in Company 1P (Table 1). One company did not provide a complete list of employees although they allowed workers to participate in the study. The overall response rate was 62.9%, varying from 56% to 72.9% among the data collection sites (Table 1). The highest response rate was 80.4% (Company 6P) and the lowest was 49.22% (Company 5G). The mean age of the study participants was 35.4 ± 10.14 years with ages ranging from 17 to 63 years. The study population was comprised of 729 (74.7%) females and 247 (25.3%) males for a ratio of 2.95:1.
Distribution of Participants Across Study Companies and Response Rate by Companies
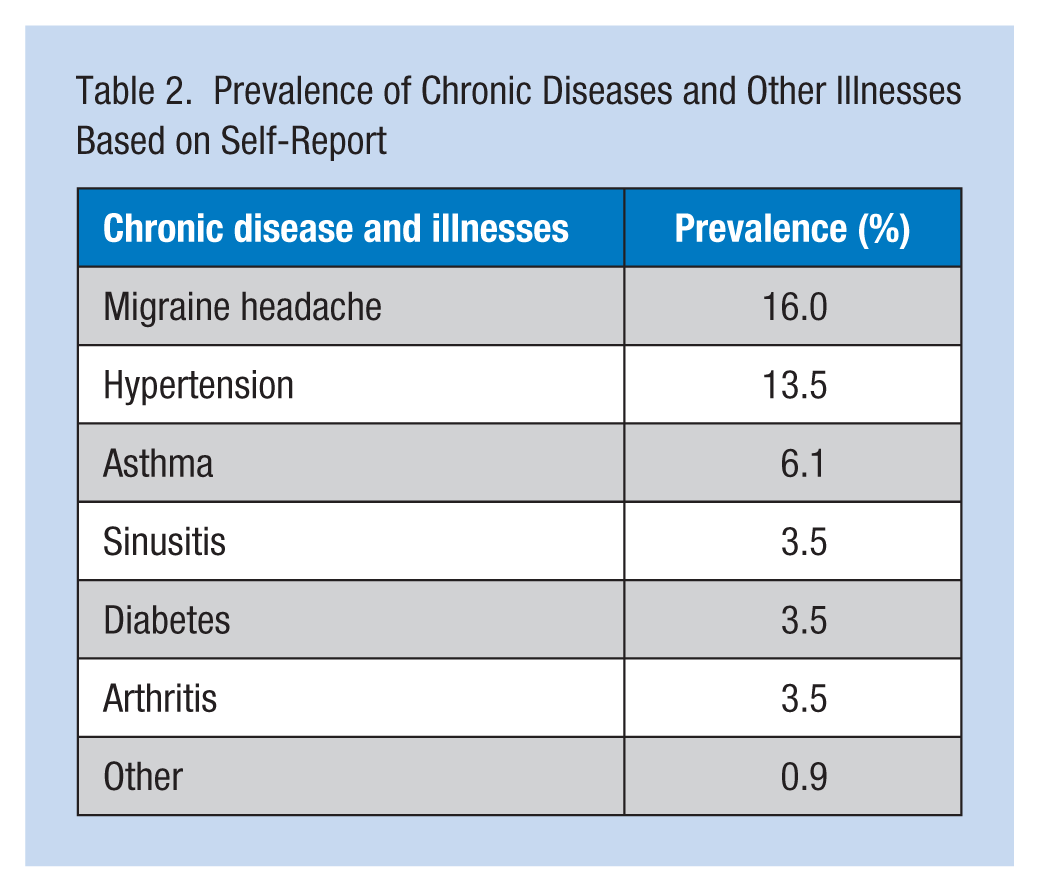
The prevalence of chronic diseases and other illnesses based on participant self-report is shown in Table 2. The most common illnesses reported by study participants were migraine headaches (16.0%), hypertension (13.5%), and asthma (6.1%). Sinusitis, diabetes, and arthritis were reported at a similar frequency (3.5%).
Prevalence of Chronic Diseases and Other Illnesses Based on Self-Report
Based on actual blood pressure measurements, 50.3% of the participants had normal blood pressures (<120/<80 mmHg), 34.1% were pre-hypertensive (120-139/80-89 mmHg), 10.5% had Stage 1 hypertension (140-159/90-99 mmHg), and 5.0% Stage 2 hypertension (≥160/≥100 mmHg; Table 3). These categories were based on the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure classification. Among the study participants, blood pressures were not uniform across age, sex, and marital status. Conversely, no differences in blood pressure measurements were found by salary, type of institution, or education (Table 3). Fourteen percent of the study participants reported a history of hypertension (14.1% of female participants and 11.9% of male participants). However, when the data were analyzed based on current anti-hypertensive medication use and blood pressure measurements greater than 140/85, 20.1% of the study population were actually identified as hypertensive. Furthermore, similar percentages of females and males (i.e., 20.7% and 21.9%, respectively) were hypertensive.
Factors Associated With Hypertension
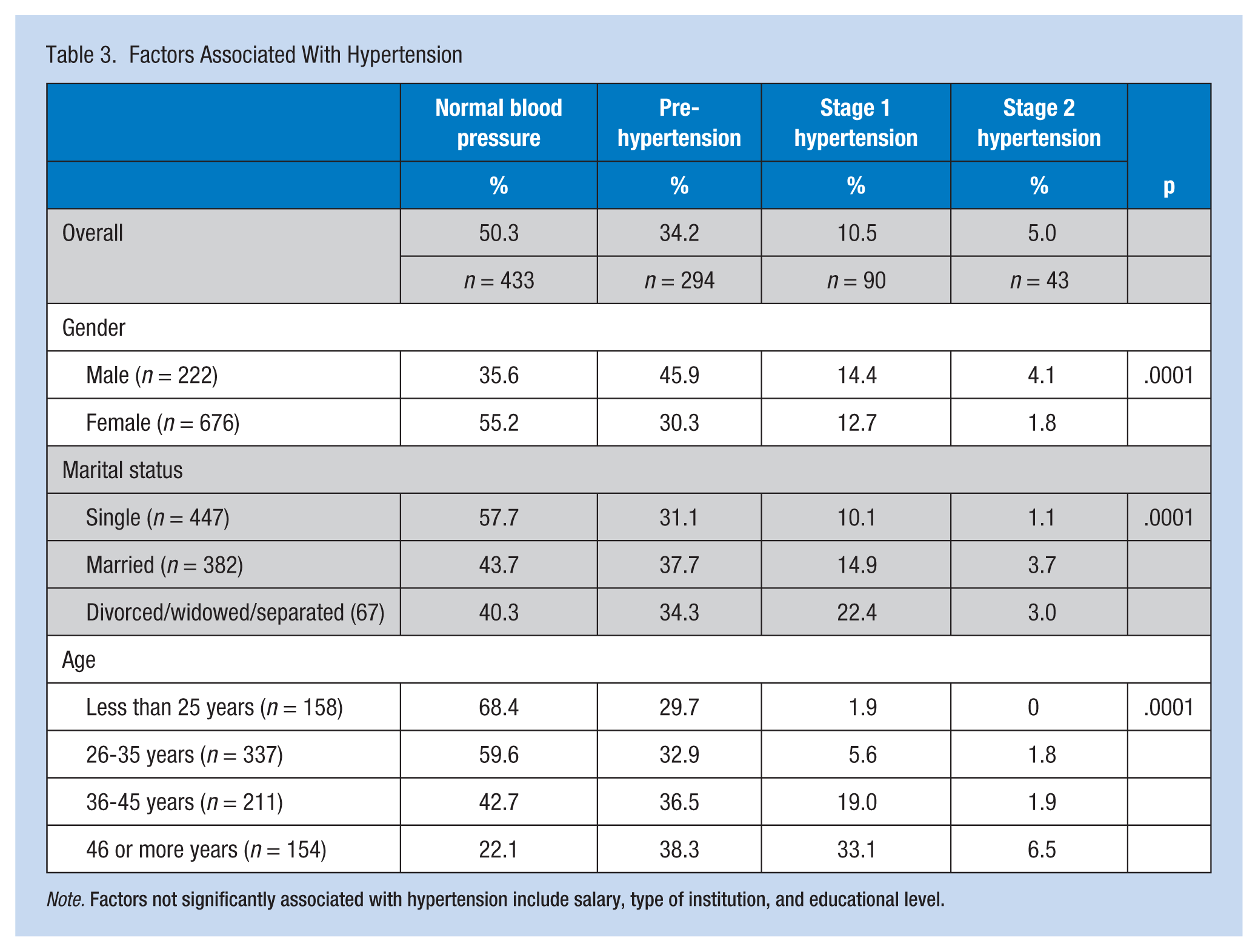
Note. Factors not significantly associated with hypertension include salary, type of institution, and educational level.
Table 4 shows the majority (84.7%) of study participants had normal cholesterol levels (<91.9 mg/dL), 12.7% had cholesterol readings between 91.9 and 109.9 mg/dL, and 2.6% had cholesterol levels greater than 109.9 mg/dL. The mean cholesterol level for this sample was 72.8 ± 12.1 mg/dL. The cholesterol levels of the study participants did not differ when compared by type of institution, gender, salary, or education. Differences in cholesterol levels by marital status were noted; however, the relationship was spurious as it lost significance when the data were analyzed by age. When respondents were divided into age groups, the proportion of participants with normal cholesterol levels decreased with increasing age. Ninety-two percent of participants less than 25 years of age had desirable cholesterol levels (<91.9 mg/dL); this percentage decreased to 89.6% among participants in the age group, 26 to 35 years. Among participants aged 36 to 45 years and 46 years and older, 80.1% and 72.2%, respectively, had normal cholesterol (χ2 = 38.35, p = .0001; Table 4).
Factors Associated With Cholesterol Levels
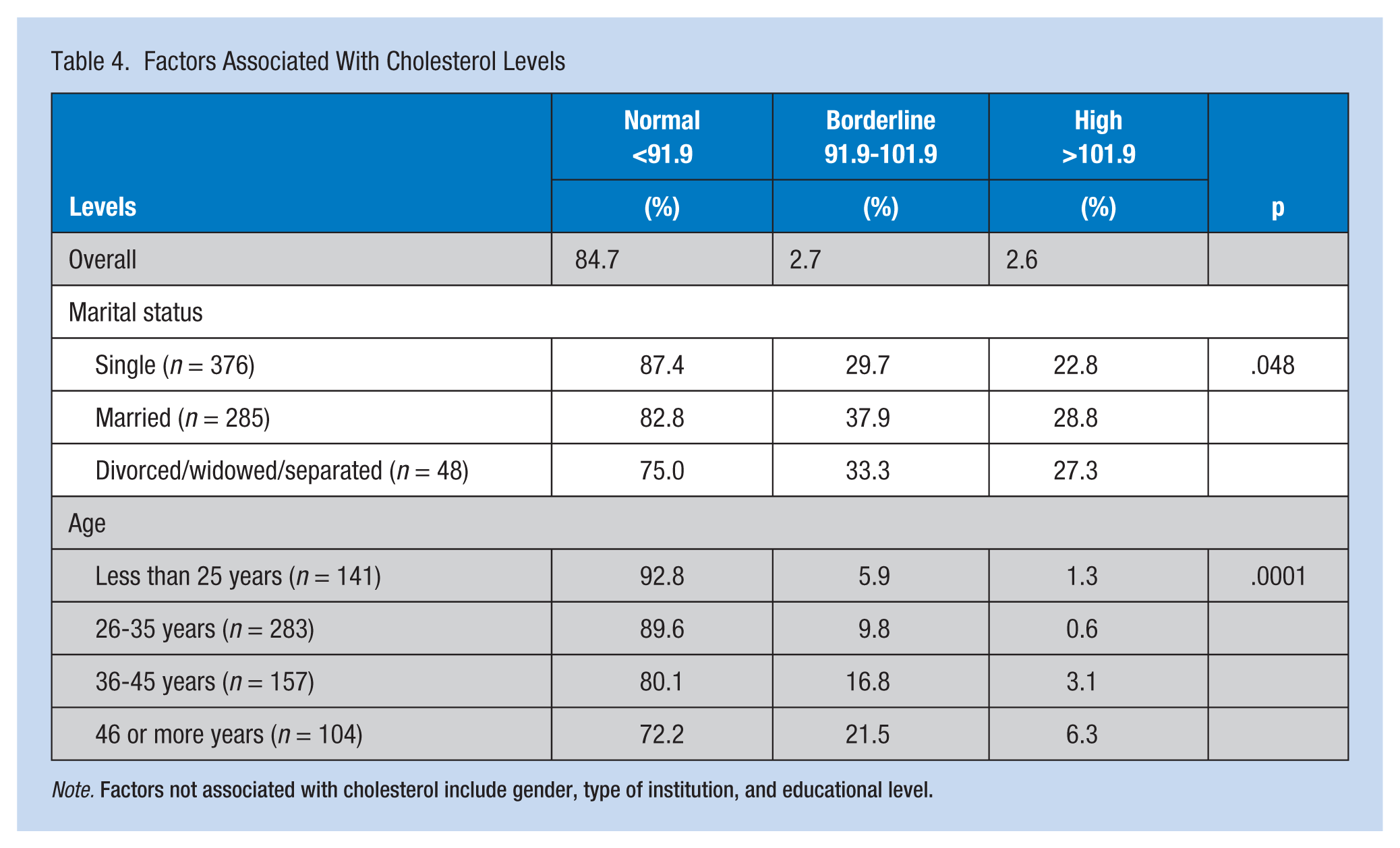
Note. Factors not associated with cholesterol include gender, type of institution, and educational level.
Only 40% of the study participants had normal BMIs; one third were overweight, 16.7% were obese, and 10% were extremely obese. Older participants were more likely to be obese than younger participants; females were more likely to be obese than males. Differences in BMI were also related to marital status and salary (Table 5). Conversely, participant BMI was not related to having children living at home, education, type of institution, exercise, or reported fast-food consumption.
Factors Associated With BMI
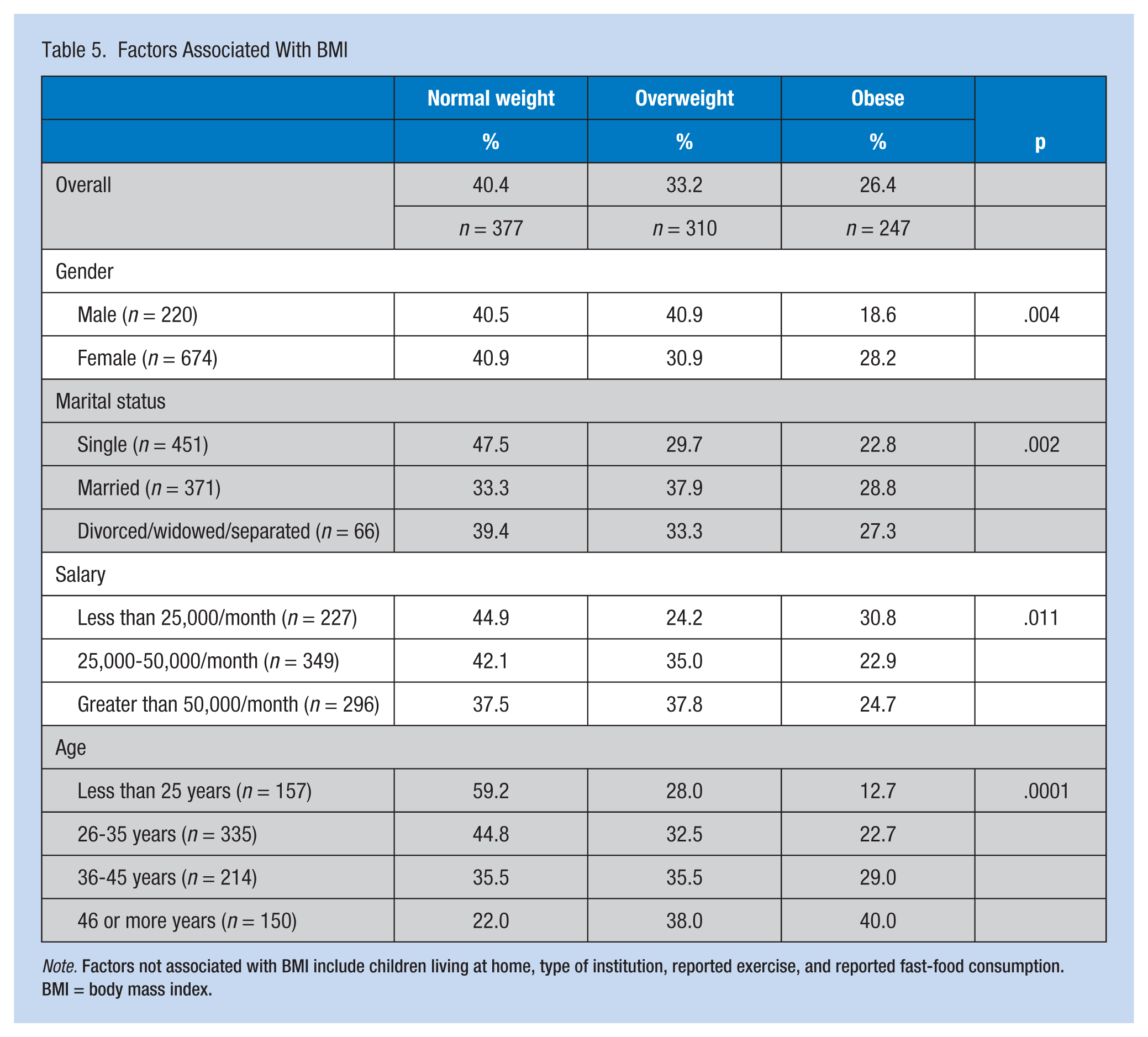
Note. Factors not associated with BMI include children living at home, type of institution, reported exercise, and reported fast-food consumption. BMI = body mass index.
Most of the employees (82.4%) had normal FBG levels (less than or equal to 106.3 mg/dL), 14% had glucose levels between 108.1 and 124.3 mg/dL, and less than 5% had measurements greater than or equal to 126.1 mg/dL. However, as participants aged, they were more likely to have elevated fasting glucose levels (χ2 = 57.11, p = .0001). Fewer males (71.8%) had normal FBG levels than their female counterparts (85.7%; χ2 = 21.74, p = .004). Single participants (88%) were most likely to have normal FBG measurements, followed by divorced, widowed, or separated participants (83.6%); common law union or married participants (75.3%) were the least likely to have normal blood glucose levels (χ2 = 23.4, p = .0001). In the same manner, 85.6% of participants who reported a college education had normal blood glucose followed by 79.3% of participants with high school education or less and only 75.7% of workers who had attended graduate school (Table 6).
Factors Associated With FBG Levels
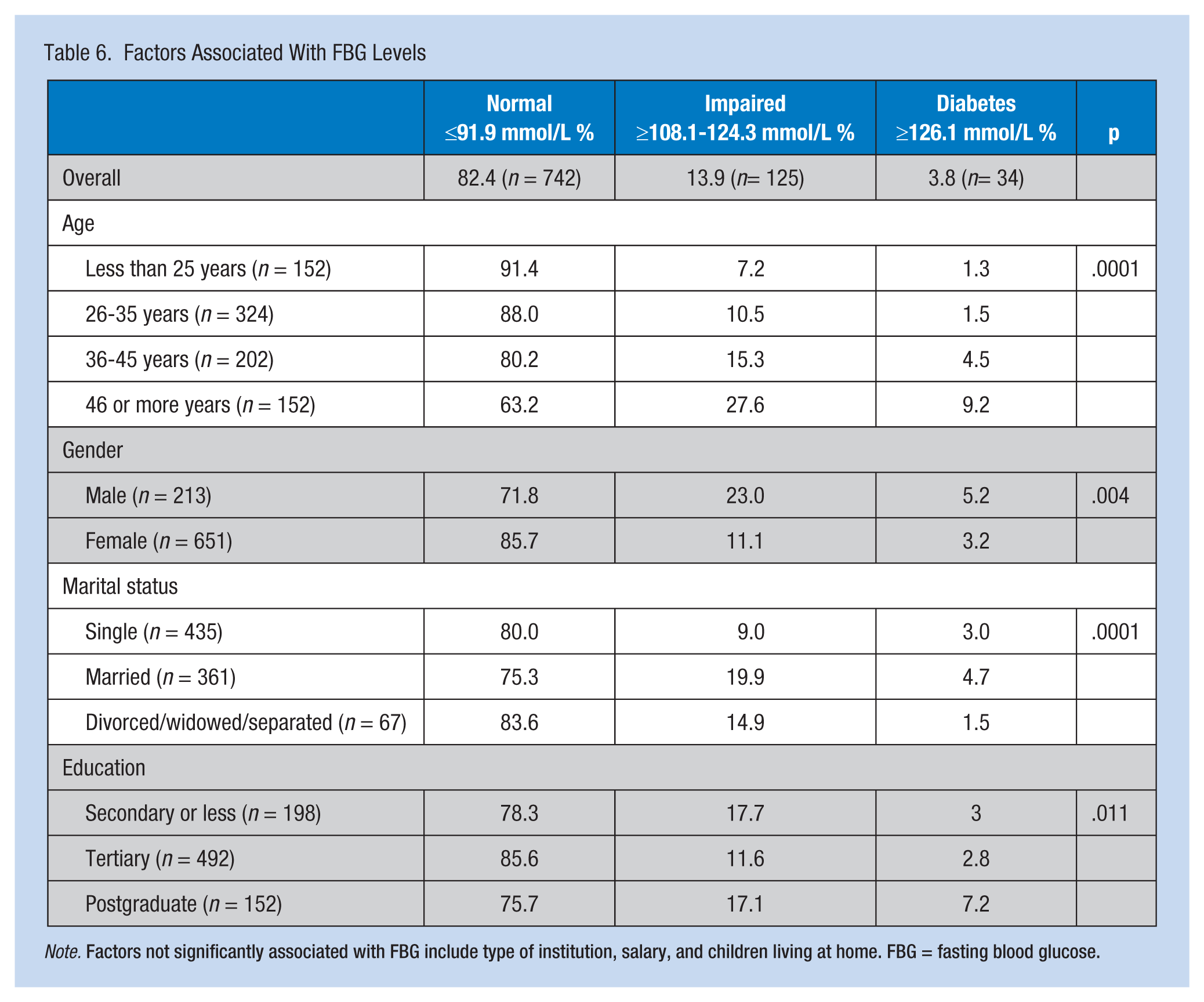
Note. Factors not significantly associated with FBG include type of institution, salary, and children living at home. FBG = fasting blood glucose.
No differences in FBG levels were found across types of institutions, salary levels, or having children at home. In addition, no relationship was found between exercise or reported weekly fast-food consumption and FBG levels. Across institutions, no differences in the prevalence of diabetes, hypertension, obesity, or hypercholesterolemia were measured by the research team.
To further explore the health status of the study population and their health-seeking behaviors, participants were asked how many times they had visited a physician in the past 6 months. Just over a quarter (26.8%) of participants had not visited a physician in the past 6 months, another quarter (27.0%) had made one visit, a similar percentage (21%) had visited 2 or 3 times, and 10% had visited a physician more than 4 times during the period. More than 46% of participants had visited a physician between 4 and 20 times in the previous 6 months.
The participants did not generally experience high stress (8.7%) at home with 44.1% reporting mild stress, 32.8% moderate stress, and 14.1% no stress at all. In addition, participants were asked to rate the level of stress experienced at work on a scale of 1 to 10. The mean level of stress reported was 6.72; however, reported stress varied from 5.79 to 6.84 across companies (f = 3.18, p = .008).
Few participants exercised. Most participants did not engage in any form of routine exercise (55.2%); 23.7% exercised for 30 minutes at least twice per week and 11% exercised for 30 minutes 3 times per week. An additional 10% of participants exercised between 4 and 7 times per week. No difference was found in the rates of exercise among employees of various types of companies. Neither were differences found by marital status, education, or whether participants reported having children residing with them. A smaller proportion of women (39.8%) reported participating in exercise than men (60.0%; χ2 = 28.90, p = .0001). Similarly, participants who were drivers (48.6%) were more likely to participate in exercise than non-drivers (41.3%; χ2 = 6.36, p = .041). Very few participants in the study were smokers (27/977 or 2.8%). However, alcohol consumption was reported by 75.4% of the study participants. Despite this high rate, most participants (47.6%) reported drinking alcohol rarely or only on special occasions (26.5%), with less than 10% reporting consuming between one and five drinks per week. Very few participants (6.3%) reported drinking alcohol to relieve stress.
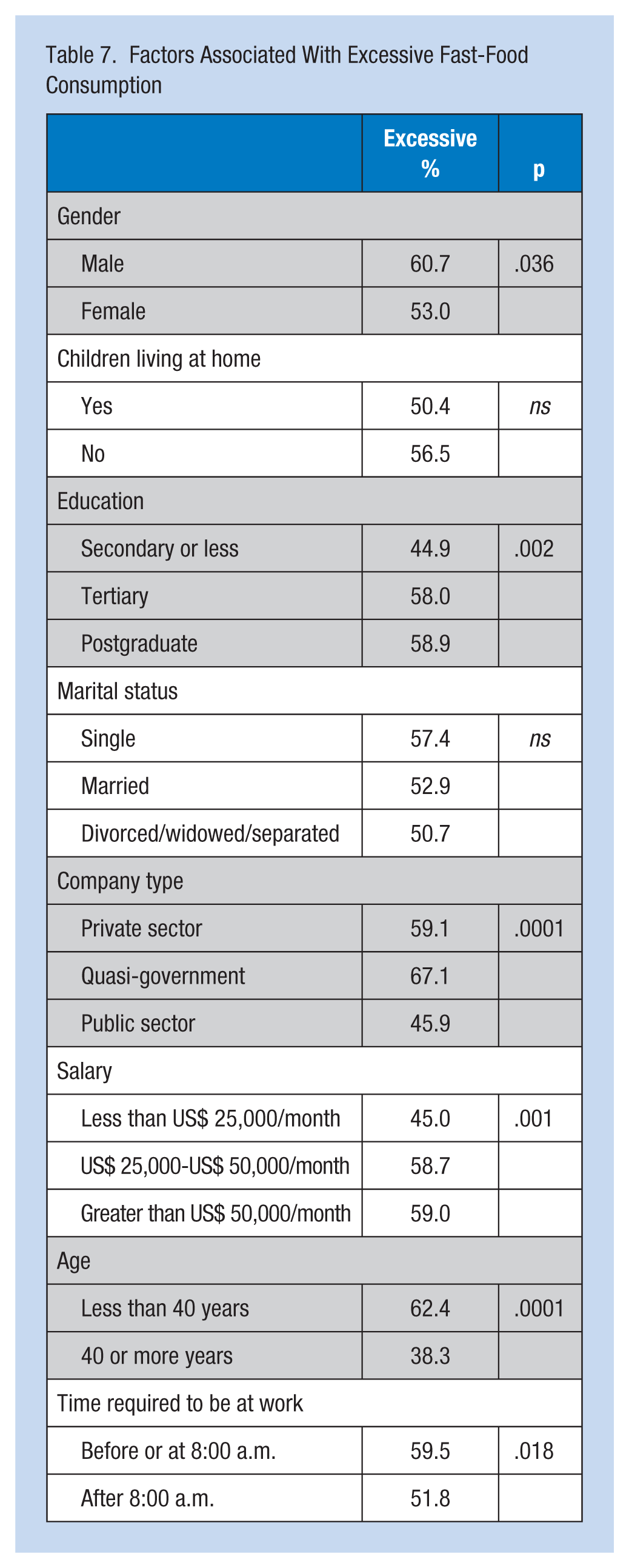
Based on the classification of Wilks, Younger, McFarlane, Francis, and Van Den Broeck (2007), fast-food consumption was classified as seldom (less than once per week) and excessive (one or more fast-food meals per week). Most (55.1%) of the study participants reported excessive fast-food consumption in the past 7 days; the remainder (44.9%) had not eaten fast food in the previous week. Among the group with excessive fast-food consumption, 15.3% reported consuming three or more fast-food meals each week with a maximum of 20 fast-food meals over the study period. The following factors were associated with reporting excessive fast-food consumption: being male, higher levels of education, being employed in quasi-private and private-sector companies, younger age, and being required to arrive at work before or at 8:00 a.m. (Table 7).
Factors Associated With Excessive Fast-Food Consumption
Discussion
The purpose of this study was to determine the health status and health practices of office-based workers in Kingston, Jamaica, as a baseline for workplace health promotion interventions. Some general trends were observed with respect to obesity, hypertension, and diabetes. First, obesity was higher among employed individuals than in the general population although the trend of women being more obese than men was observed in both studies (Wilks et al., 2007). Whereas obesity was estimated at 23.9% and 7.6% in women and men in the general population, the estimates in this study population were 28.2% and 18.6% for women and men, respectively (Ichinohe et al., 2005; Mendez, Cooper, Wilks, Luke, & Forrester, 2003). Rates of exercise in this study population, which is one way to control obesity, were very low with more than 50% of participants reporting that they did not participate in any form of exercise. Only 21% of participants engaged in exercise for 30 minutes or more 3 times or more each week and was more common among drivers than non-drivers. Motor vehicle ownership (drivers) may be a proxy for higher socio-economic status and the higher likelihood of participating in exercise activities. Furthermore, men reported more frequent exercise than women, consistent with exercise rates in the general population (Wilks et al., 2007). Obesity increased with age and was more likely if participants were cohabitating; higher salaries were associated with lower prevalence of obesity.
Hypertension in the study population (14.1%) was much lower than that seen in the general population (25.2%; Ferguson, Francis, et al., 2011). This finding may be reflective of the target population of office workers, which may in turn reflect higher levels of education and health awareness than the general population. The prevalence of hypertension increased with age and was greater among males than females. Like obesity, cohabitation was not protective for hypertension with the lowest rates occurring among unmarried workers (11.2%) followed by married workers (18.6%) and then divorced/widowed workers (25.4%). The findings of this study suggest that more males than females were unaware of their blood pressure status, which may present an opportunity to target health promotion interventions to male workers (Welsh, Duff, Campbell-Taffe, & Lindo, 2015).
The prevalence of diabetes among employed males (5.2%) was lower than the general population estimate of 7.9% (Ferguson, Francis, et al., 2011). Similarly, the estimate among employed females (3.2%) was significantly less than that among females in the general population (15.7%; Ferguson, 2011).
Cholesterol for most study participants was normal. However, more than half of the study population reported excessive fast-food consumption (Wilks et al., 2007). Within this population, 15.3% consumed three or more fast-food meals per week. This high rate of fast-food consumption may contribute to higher rates of obesity among the study participants compared with the general population. The results strongly suggest that socio-economic status is a predictor of fast-food consumption, which increased with higher education and monthly income, and was lowest among public-sector workers who are the poorest paid of all subgroups in the study. Other factors associated with fast-food consumption were being male and required to arrive at work early.
Cigarette smoking was very low with less than 3% of employed participants reporting tobacco use. This finding is in sharp contrast to the general population for which 22.1% of males and 7.2% of females reported smoking cigarettes (Ferguson, Francis, et al., 2011). Similarly, in the current study, 75.4% of participants reported alcohol use, although only infrequently. The study did not ask about recent alcohol use (in the past week or month); these data would have been a more appropriate measure of use. In a study of the general population, 79.8% of men and 51.9% of women reported using alcohol within the last month. Low alcohol and tobacco use in this study population present an opportunity for examining chronic disease outcomes in the absence of these two predictors.
The study population visited physicians often; almost half of the participants visited their physicians at least 3 times in the previous 6 months. Private-sector workers are likely to have private health insurance from their employers and can access private or public providers. Furthermore, since 2008 when Jamaica introduced a system of no user fees at its 330 health centers and 23 public hospitals, financial constraint may no longer be a deterrent to accessing health care.
This study has significant implications for occupational health nurses in Jamaica. By providing a health profile of office workers independent of company type, interventions to improve this health profile can be offered to all office workers.
The researchers acknowledge study limitations related to the study’s cross-sectional design and use of unadjusted descriptive statistics. The study findings revealed a high prevalence of obesity among Jamaican office workers, and the researchers suggest that excessive consumption of fast food and lack of physical activity (especially among women) may be significant contributors to chronic illnesses. Hyperlipidemia and alcohol and tobacco use were relatively low among the study participants. Targeted workplace health promotion activities and accompanying monitoring are indicated for this group.
Applying Research to Practice
A sedentary lifestyle is a major contributor to epidemics of obesity and associated co-morbidities including hypertension and diabetes. Office-based work is often associated with a sedentary lifestyle during commuting and at the workplace. The health practices and profiles of office-based workers in Jamaica are unknown. The workplace is an excellent place for health promotion because persons spend a significant portion of their day at work. However, workplace health interventions are reliant upon accurate data of health profiles and practices.
High rates of obesity, hypertension, and fast-food consumption among office-based workers were of major concern. There were no differences in health profile between employees in the public or private sector and this provided an opportunity for national workplace health intervention policies and programs.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by the National Heath Fund (NHF) and the Culture, Health, Arts, Sports and Education Fund (CHASE).
Author Biographies
Jascinth L. M. Lindo is associate professor in the College of Nursing & Health Sciences at Barry University and lecturer in the University of the West Indies, School of Nursing, Jamaica. This work was completed in partial fulfillment of her doctoral studies. She has published 24 peer-reviewed articles in her areas of workplace health, maternal and child mortality, and nursing.
Janet LaGrenade is a former senior lecturer in the Department of Community Health and Psychiatry, at the University of the West Indies. She is a psychiatrist by training and has an interest in workplace health with a focus on the health sector. She has also conducted research on primary mental health care. She has supervised many students at the master’s and PhD levels.
Denise Eldemire-Shearer is professor of public health and aging at the University of the West Indies. She is director of the WHO Collaborating Centre at the University of the West Indies and former head of the Department of Community Health and Psychiatry. Her research focus is the role of primary care on the health and wellness of the aging population. She is currently director of postgraduate studies at the University and has supervised many students at the PhD level.