
Abstract
Nursing is a physically active profession; however, nurses and nursing support staff may limit their physical activity (PA) on non-workdays. The purpose of this pilot study was to examine the effects of a 12-week pedometer-based PA intervention on daily steps of hospital nursing and support staff from two departments, emergency (ED) and oncology (ONC). The 12-week minimal-contact, self-managed intervention was designed to increase total and non-workday PA. Twenty participants with an average age of 47.6 ± 7.1 years completed the intervention. Significant differences were found between total daily steps at baseline (8,446) and at 12 weeks (10,655; p = .014), and between workday steps at baseline (10,398) and at 12 weeks (13,056; p = 0.005). Oncology unit participants significantly increased their non-workday steps from baseline (5,850) to 12 weeks (9,829; p = .003). As part of a comprehensive intervention, pedometers can promote total and non-workday PA of nursing and support staff.
Nursing is a physically active profession, particularly in hospital settings with 12-hour work shifts. Welton, Decker, Adam, and Zone-Smith (2006) found that hospital nurses walked 4 miles to 5 miles during a 12-hour shift. Yet, overweight and obesity rates, physical activity (PA) levels, and other health habits are about the same for nurses as the general population (Tucker, Harris, Pipe, & Stevens, 2010). It could be that nurses compensate for PA during shiftwork by limiting leisure-time PA, or perceive they engage in adequate PA while at work so do not need additional PA on non-work days, which limits total PA and negatively affects overall health.
In a study of Australian and New Zealand nurses, workplace PA did not positively affect health and well-being, but leisure-time PA was associated with better health and well-being (Henwood, Tuckett, & Turner, 2012). Given the potential for positively affecting the health and well-being of nurses, it would seem that increasing leisure-time PA could be important.
Many strategies have been used to increase the PA of workplace populations. One recommended strategy has been the use of pedometers as a motivational tool; pedometers are easy to use, cost-effective, and give instant feedback on daily steps. Pedometers have been successfully used in interventions to increase the daily steps of wearers, especially when used in conjunction with goal-setting, PA counseling, and self-monitoring (Bravata et al., 2007). Limited research on the use of pedometers with nurses was identified. Most pedometer-based interventions have focused on hospital or clinic employees in general, with some participation by nurses and nursing support staff (Chyou, Scheuer, & Linneman, 2006; Hess, Borg, & Rissel, 2011; Shaw, Alfonso, Howat, & Corben, 2007). Lavoie-Tremblay et al. (2014) examined the impact of an 8-week pedometer-based intervention on nurses’ PA and various health outcomes. Although pedometer-determined PA was only collected post intervention, PA scores collected via International Physical Activity Questionnaire (IPAQ) collected pre and post intervention indicated no change in vigorous PA, moderate PA, or walking. In a 10-week pedometer-based intervention for hospital nurses who are also working mothers, Tucker et al. (2011) found increases of about 1,400 daily steps in both the intervention and control groups; however, no statistically significant difference between intervention and control groups was found. The goal of the aforementioned interventions was to increase total PA, including PA at work and at home.
No research could be identified that examined the effects of a PA intervention or a pedometer-based intervention on the non-workday PA of nurses or nursing support staff working in a hospital setting. Given long work shifts, it would seem that the most likely opportunity for leisure-time PA would be on non-workdays. Thus, the purpose of this study was to examine the effects of a 12-week pedometer-based PA intervention on daily steps of hospital nursing and nursing support staff to increase non-workday PA.
Method
This pilot study used a quasi-experimental, pre/post-test design to examine the effects of a 12-week pedometer-based program on total daily steps, total workday steps, total non-workday steps, body mass index (BMI), and waist circumference. Data collection and counseling sessions were scheduled at the workplace.
Sample
The participants in this pilot study were 20 nursing and nursing support staff from two departments, emergency (ED) and oncology (ONC), at a Portland area hospital. Participants were recruited via presentations at department staff meetings. Before participating in the study, all participants read and signed an informed consent form approved by the hospital’s institutional review board and completed a Physical Activity Readiness Questionnaire to determine whether participants needed to consult their physicians prior to initiating the PA program.
Measures
Demographic (i.e., age, gender, ethnicity, education) and occupational (i.e., unit, position, shift, hours per shift) data were collected at baseline. Health data (i.e., height and weight to determine BMI, waist circumference.) were collected at baseline and at 12 weeks post intervention.
To determine daily steps, participants wore an Accusplit AE120x electronic pedometer (an imported version of the Digi-Walker SW-200) for 7 days at baseline. Reliability and validity of various Digi-Walker models in accurately assessing daily step counts have been established with adult populations in free-living conditions (Le Masurier, Lee, & Tudor-Locke, 2004). Participants also wore a second pedometer while at work during the baseline period to determine workday steps. The pedometer was worn on the waist, clipped to a belt or clothing, and centered over the dominant foot, with exact placement determined by a 20-step walking test. Participants were instructed to wear the pedometers during all waking hours except when bathing or swimming. For the baseline pedometer measure, pedometers were examined after 7 days and step counts recorded. The average step counts of the final week of the 12-week intervention, as recorded in the participants’ logs, were also recorded.
Intervention
The PA intervention used in this study was a modification of the program called “Maine in Motion,” a program developed by the Maine Governor’s Council on Physical Activity. The program, based on social cognitive theory, uses a participant manual and consists of counseling, pedometers, and self-monitoring. Upon completion of pre-intervention testing, all group participants met with a researcher to set daily step goals, review pedometer use, discuss procedures for keeping a step calendar, review tips for increasing daily PA, and identify strategies for overcoming barriers. Goals for non-workdays were individualized, whereby participants had the option to increase or maintain their current daily steps; the majority of participants opted for an increase of 10% over baseline daily steps for their initial goal and were instructed on how to set new weekly or bi-weekly goals during the intervention. Participants wore the pedometer as instructed and learned to reset pedometers to zero at the beginning of each day. At the end of each day, participants learned to remove the pedometer and record the following on their step calendar: date, workday or non-workday, and total number of steps displayed on the pedometer.
Analysis
Both descriptive and inferential statistics were used to analyze the data. Independent-samples t tests were used to determine significant differences among the groups at baseline. Paired t tests were used to determine significant differences between baseline and post-program physical scores.
Mixed factorial ANOVA procedures with one independent group factor (group [A or B]) and two repeated measures factors (time and treatment [group by time interaction]) were used to examine changes over time and differences between the groups on the change scores. Statistical significance was set at p < .05. Data were analyzed using SPSS Version 19.0 (Chicago, Illinois).
Results
Demographic data can be found in Table 1. Twenty participants (19 females, one male), with an average age of 47.6 (SD = 7.1) years (range = 33-63 years), completed the intervention. A majority of the participants were Caucasian, held a college degree, held registered nurse (RN) or licensed practical nurse (LPN) positions, worked first shift, and worked 12-hour shifts. Seven participants worked in ONC, and 13 worked in ED. No significant differences were found among the groups from baseline to 12 weeks on any measures. At baseline, a significant difference was found between daily steps during workdays and non-workdays for the total sample.
Demographic Data
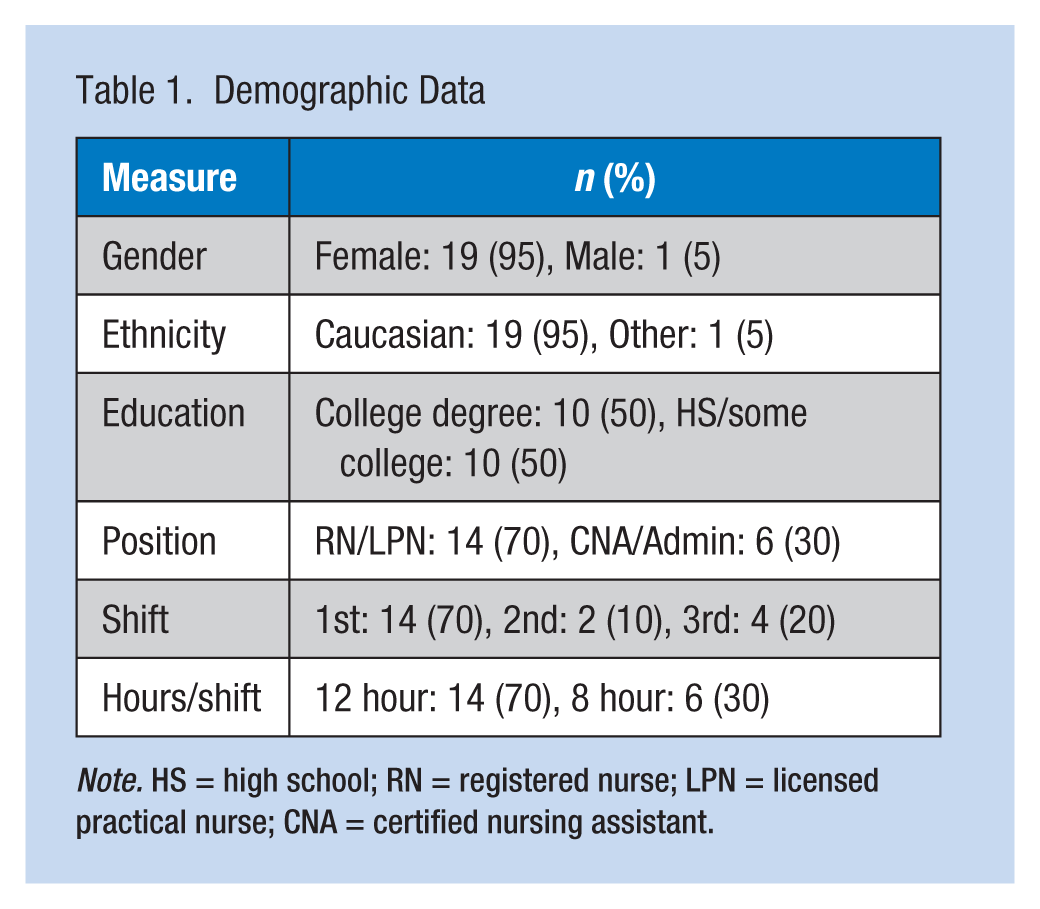
Note. HS = high school; RN = registered nurse; LPN = licensed practical nurse; CNA = certified nursing assistant.
Baseline and post-intervention measures can be found in Table 2. For total daily steps, a significant main effect was found for time, F(1, 17) = 7.512, p = .014. No main effect was found for the group, F(1, 17) = 1.599, p = .223, nor time by group interaction, F(1, 17) = 0.162, p = .692. A significant increase was found in total daily steps from baseline to post intervention, 8,446 (SD = 2,266) to 10,655 (SD = 2,023; p = .003).
Baseline and 12-Week Measures (M ± SD)
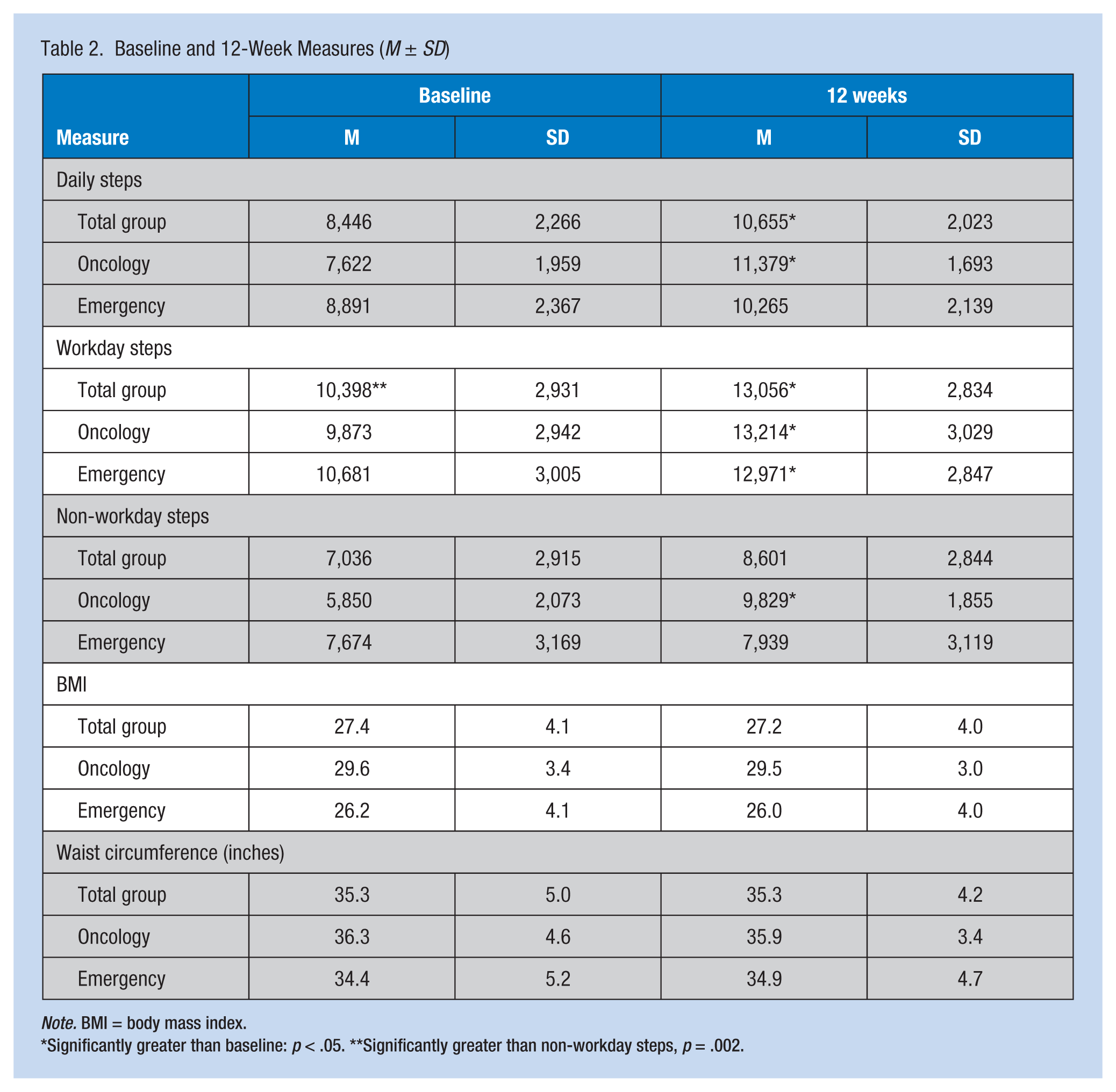
Note. BMI = body mass index.
Significantly greater than baseline: p < .05. **Significantly greater than non-workday steps, p = .002.
For workday steps, a significant main effect was found for time, F(1, 17) = 10.110, p = .005, and no main effects was found for the group, F(1, 17) = 0.206, p = .655, nor time by group interaction, F(1, 17) = 0.188, p = .670. A significant increase in workday steps was found at baseline to post intervention, from 10,398 (SD = 2,931) to 13,056 (SD = 2,834; p = .000).
For non-workday steps, significant main effects were found for time, F(1, 17) = 6.636, p = .005, and for group, F(1, 18) = 5.082, p = .019; however, no time by group interaction was found, F(1, 18) = 0.001, p = .975. The total group had a non-significant increase in non-workday steps from baseline to post intervention, from 7,036 (SD = 2,915) to 8,601 (SD = 2,844), with no significant differences between the groups (p = .087); participants from oncology significantly increased their non-workday steps from baseline to post intervention, from 5,850 (SD = 2,073) to 9,829 (SD = 1,855; p = .003).
For BMI and waist circumference, no significant main effects for time, group, or time by group interaction were found. No significant differences in BMI were found at baseline (27.4, SD = 4.1) and post intervention (27.2, SD = 4.0; p = .172), or waist circumference at baseline (35.3, SD = 5.0) and post intervention (35.3, SD = 4.2; p = .969).
Discussion
The objective of the intervention in this study was to increase daily steps, specifically the non-workday steps of nursing and nursing support staff. The total sample increased their total daily steps; the oncology group also increased their non-workday steps. However, no significant changes were found in participants’ BMI or waist circumferences.
At baseline, nursing and support staff in the present study averaged 8,400 total daily steps. When compared to 5,100 daily steps measured in the general population (Bassett, Wyatt, Thompson, Peters, & Hill, 2010), there is some support to the belief that nursing and nursing support staff are more physically active in general. Compared with other nurses, total daily steps were considerably lower than the 12,500 daily steps found in a previous study (Tucker et al., 2011); however, the sample in the Tucker study was considerably younger than in the present study (35 years vs. 48 years).
Participants in the present study did not achieve the post-intervention daily steps found in two prior studies of nurses. Total daily steps in the present study were 10,655. In a study with similarly aged nurses, 12,913 steps were reported post intervention; however, baseline steps were not reported (Lavoie-Tremblay et al., 2014). In another study of medical center staff with an average age of 40 years, which included nursing staff, post-intervention scores were higher than the present sample; however, baseline steps were also higher (10,265 vs. 8,446; Shaw et al., 2007).
The increase in total daily steps found in this study can be partially accounted for by an increase in workday steps of participants, which was not a primary objective of the study. Although a change in work conditions is an unlikely explanation for this increase in steps, perhaps participants increased their leisure-time steps on workdays as well as non-workdays.
Increasing non-workday steps was the primary objective of the study, and the oncology group did significantly increase their non-workday steps. They had lower non-workday steps at baseline, thus greater room for improvement. Hess et al. (2011) also found greater increases in PA among initially inactive hospital participants. The less active are precisely the population that benefit most from increases in PA and are thus a prime target for workplace interventions.
As expected, nursing and nursing support staff achieved greater daily steps on workdays (10,398) versus non-workdays (7,036). This finding is consistent with prior studies on subjectively determined PA levels of workers in active professions and a study on postal workers in Scotland, which reported that delivery staff achieved more steps on workdays than non-workdays (Tigbe, Lean, & Granat, 2011). These findings lend support for an increased emphasis on non-workday PA for individuals in generally active professions.
No changes were found in BMI or waist circumference as might be expected after a PA intervention of short duration. A recent pedometer-based intervention study of similar duration with nurses of comparable age also found no changes in BMI and waist circumference (Lavoie-Tremblay et al., 2014); another study of longer duration but similar aged participants, which also included clinic physicians and staff, had positive reductions in BMI (Chyou et al., 2006). Perhaps a longer intervention duration (20 weeks or more) is more likely needed for positive changes in waist circumference and BMI.
The findings of this study are preliminary. The sample in this study was small, fairly homogeneous, and self-selected, which could have resulted in selection bias, thus limiting the generalizability of the findings. It is recommended that future studies include a control group and recruit a larger sample. Given the propensity for PA to revert to baseline levels after the intervention, long-term monitoring for 6 months to 12 months is recommended. Finally, step equivalents for non-ambulatory PAs are also recommended because pedometers can under-record (cycling) or not record (swimming) for certain activities.
Conclusion
In summary, participants enrolled in the 12-week pedometer intervention increased their daily steps and workday steps. The group that was less active at baseline increased their non-workday steps, the main focus of the intervention. As part of a comprehensive intervention, pedometers, used in conjunction with brief counseling, self-monitoring, and ongoing contact, can promote PA (e.g., total and non-workday steps) among nursing and support staff.
Results from this study have implications for occupational health nurses who develop and implement PA interventions at worksites, particularly interventions for nurses and nursing support staff. Although interventions could be designed for the workday at worksites, it is likely not feasible to increase leisure-time PA on workdays for those individuals who work long shifts in active professions. Thus, for those individuals in active professions who may compensate by limiting activity on non-workdays, the focus of interventions should be on increasing leisure-time PA on non-workdays.
Applying Research to Practice
Hospital nurses and nursing support staff may be physically active at work, especially during long shifts. However, these staff members may be less active on non-workdays. The health of nurses and nursing support staff could benefit if employers offered interventions designed to increase non-workday PA. The use of pedometers or other wearable activity monitors, in conjunction with goal-setting and self-monitoring, could motivate participants to increase PA on non-workdays, at least in the short term.
Footnotes
Acknowledgements
The author wishes to thank the following individuals for their contributions to development of the study and data collection: Laurie Mitchell, assistant vice president of global wellbeing and health; Nicole Cooley, corporate program director for medically oriented gym; Elizabeth Winship, staff physical therapist at Maine Medical Center; and Leah Hebert and Vijiayurani Suresh, former graduate students in the MS in Nurse Practitioner program at the University of Southern Maine.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an in-kind grant from MaineHealth.
Author Biography
Dr. Karen Croteau is a professor in the Department of Sport and Exercise Science at Saint Joseph’s College. A fellow in the American College of Sports Medicine, she has conducted numerous research projects in the area of pedometer-based physical activity interventions for a variety of populations.