
Abstract
This exploratory study determined the impact of organizational structure, particularly participation in decision making, instrumental communication, formalization, integration, and promotional opportunity, on burnout among Pakistani pediatric nurses. Data were collected from pediatric nurses working for Punjab’s largest state-run hospital. The findings revealed that participation in decision making, instrumental communication, and promotional opportunity prevented burnout. Formalization contributed to burnout but integration was not related to burnout. Quite interestingly, except for supervisory status, most control variables for this study were not significantly related to emotional burnout. Hence, the hypothesis that organizational structure is a determinant of job burnout was accepted.
Keywords
Contemporary nursing requires constant assertiveness, friendliness, warmth, technical skill, physical strength, and emotional and intellectual effort (Estryn-Béhar et al., 2007; Gandoy-Crego, Clemente, Mayán-Santos, & Espinosa, 2009; Jourdain & Chênevert, 2010; McVicar, 2003; Whittington, 2002). However, the overload of psychological processing, concentration, and activity often results in tension, fatigue, and tiredness, both during and after the workday (Ben-Zur & Michael, 2007; Hasselhorn, 2007; McGrath, Reid, & Boore, 2003; Watson, Deary, Thompson, & Li, 2008). Furthermore, nurses frequently experience a discrepancy between the professional prestige of nursing and its demands and expectations. In Pakistan, though the demand for nurses is high, their economic security and social status are low, resulting in significant migration. These circumstances may result in feelings of despair, fear, or disappointment, leaving nurses emotionally susceptible to burnout syndrome.
Burnout reduces nurses’ quality of life at both home and work. Unless its victims can recover, they constantly struggle to muster energy to function at an expected level (Cocco, Gatti, de Mendonça Lima, & Camus, 2003). Burnout is also associated with psychosomatic health hazards and substance abuse (Burke & Greenglass, 2001; Cocco et al., 2003; Maslach & Leiter, 2008; Watson et al., 2008); burnout can affect nurses’ self-image, resulting in less concern for themselves (Breninkmeijer et al., 2001). Burnout, over time, can increase problems at home, leading to detachment from friends and family (Burke & Greenglass, 2001; Jackson & Maslach, 1982; Kilfedder, Power, & Wells, 2001).
The quality of services that nurses provide is also affected by burnout, creating an unpleasant environment for colleagues and patients (Gandoy-Crego et al., 2009). Nurses experiencing burnout are unenthusiastic and dread going to work (Cherniss, 1980). They withdraw from both peers and patients, and may treat them coldly, as impersonal objects (Diers, 1982; Maslach & Leiter, 2008). These nurses become less effective at and withdraw from work; their patients and coworkers are forced to handle this situation. When nurses experience burnout, health care institutions suffer as well. Hospitals depend on nursing staff to perform critical functions and cannot operate without nurses. Burnout can affect performance and increase work withdrawal, turnover intent and turnover, and absenteeism (Burke & Greenglass, 2001; Cocco et al., 2003; Hillhouse & Adler, 1997; Jourdain & Chênevert, 2010; Kilfedder et al., 2001; McGrath et al., 2003; Watson et al., 2008). Simply said, burnout, in the health care industry is costly and harmful to employees, their patients, colleagues, family, hospital workplaces, and society (Cocco et al., 2003; McVicar, 2003). In the era of shrinking budgets, rising costs, and personnel shortages, it is especially crucial to protect nursing staff from burnout.
The public may blame individual employees for burnout rather than the work environment (Maslach, 2011). Some individuals argue that incompetent employees burn out; other individuals believe that workers who burn out are working too much or too hard. However, research does not support these arguments and suggests that situational and contextual factors contribute to burnout (Maslach, 2011; Schaufeli & Enzmann, 1998).
Despite being a serious issue in the health care industry, burnout has still not received needed empirical attention (Cocco et al., 2003). To respond to this critical issue, exploration of the work environment could contribute to an understanding of the possible sources of burnout. Although the body of nursing research has expanded considerably, many organizational sources of burnout remain unexplored. This descriptive study was therefore conducted to determine the relationship between organizational structure (i.e., particularly, its dimensions of participation in decision making, instrumental communication, formalization, integration, and promotional opportunity) and a dimension of burnout (i.e., emotional exhaustion) among pediatric nurses at a government-regulated hospital.
Literature Review
Despite being globally widespread, burnout has no all-embracing and specific definition in the literature. Freudenberger (1974) coined the term job burnout and defined the term as feelings that occur when individuals become exhausted and worn out by excessive work demands. Kafry and Pines (1980) proposed that burnout is a condition of work tedium, which distresses and disconnects employees from their jobs, so they feel depleted physically and emotionally. Kahn (1978) posited that burnout stems from an individual’s pessimistic outlook toward self and others, which gradually leads to psychosomatic exhaustion. Pines and Maslach (1978) stated that “burnout is a syndrome of physical and emotional exhaustion involving the development of a negative self-concept, negative job attitudes, and a loss of concern and feeling for clients” (p. 56). Freudenberger (1980) later redefined burnout as a state of frustration or fatigue for an employee. The pioneers in the field of burnout, Maslach and Jackson (1981), viewed burnout “as an increased feeling of emotional exhaustion, depersonalization, and reduced personal accomplishment, which becomes apparent at the endpoint of continuous, unsuccessful coping” (p. 99).
Consistent with Maslach and Jackson (1981), burnout consists of three dimensions: ineffectiveness, emotional exhaustion, and depersonalization. Ineffectiveness is defined as being less productive when working with clients and peers. It is a feeling that work has not made a meaningful difference to others and the organization. Emotional exhaustion implies being emotionally worn-out and consumed by the job. Burned-out workers show little or no emotional enthusiasm, desire, or energy to go to work every day. Depersonalization means being insensitive and impersonal toward others in the workplace. When employees experience burnout, they develop a cynical attitude and distance themselves from others, which results in detachment from work (Maslach, 1982, 2011).
Maslach (1982) originally hypothesized that first emotional exhaustion occurs, then, as a counteraction, depersonalization follows, which ultimately causes ineffectiveness. Maslach and Jackson (1984) later noted that the three dimensions were equally represented during burnout but were independent of each other. They posited that the nature of the work environment determines the occurrence and effects of each dimension (Cordes & Dougherty, 1993; Maslach, 2011). Cherniss (1980) proposed three stages of job burnout. Job demand and resource imbalance occur in the first stage, which leads to emotional stress for employees during the second stage. Workers become cynical in the third stage, feel a lack of accomplishment and view others in an impersonal, detached manner which leads workers to disengage from others and from their jobs, which finally results in ineffectiveness at work. Golembiewski (1989) agreed on the same burnout dimensions, but proposed that first depersonalization occurs, which leads to ineffectiveness at work, causing strain, frustration, and ultimately emotional exhaustion for employees. Finally, Schwab and Iwanicki (1982) theorized that these dimensions do not necessarily follow a causal process; they are individual concepts that are mutually exclusive of each other.
Several different perspectives on job burnout have been posited, all of which consider emotional exhaustion the core of burnout (Cordes & Dougherty, 1993; Maslach, 1982). Compared with other burnout dimensions, emotional exhaustion has been studied widely. Emotional exhaustion, as mentioned earlier, is viewed as the first stage of burnout. Workers usually refer to feelings of emotional exhaustion, the most commonly experienced form of burnout, when they discuss their or others’ experiences of burnout (Burke & Greenglass, 2001; Cocco et al., 2003; Kilfedder et al., 2001; Maslach, 2011; Maslach & Leiter, 2008; McGrath et al., 2003; McVicar, 2003; Watson et al., 2008). Emotional exhaustion has been the focus of several prior studies on nursing staff burnout (Armstrong-Stassen, al-Ma’Aitah, Cameron, & Horsburgh, 1994; Ben-Zur & Michael, 2007; Estryn-Béhar et al., 2007; Gandoy-Crego et al., 2009; F. J. Lee, Stewart, & Brown, 2008). Hence, burnout’s emotional exhaustion dimension is the main focus of this article.
Research on Pediatric Burnout
The work of health care professionals, particularly pediatric neurologists, oncologists, and nephrologists, is emotionally and physically more challenging than other work, and thus can lead to burnout (Garcia et al., 2014). In pediatric health care, the work environment is stressful, tasks are taxing, and required commitment is greater (Kotzer, Koepping, & LeDuc, 2006; Maytum, Heiman, & Garwick, 2004). Pediatricians regularly interact with infants, children, and adolescents diagnosed with incurable chronic illnesses. They also deal with emotional, stressed, and fatigued parents or caretakers who often ask unanswerable questions (Al-Youbi & Jan, 2013; McPhillips, Stanton, Zuckerman, & Stapleton, 2007). Burnout sharply affects pediatricians’ ability to practice effectively, hinders the development of healthy caregiver–patient relationships, and seriously compromises the quality of care delivered (Meyer, Li, Klaristenfeld, & Gold, 2015). Pediatric novice nurses’ compassion fatigue has been investigated as a mediator between stress exposure and compassion satisfaction, burnout, and job satisfaction (Adwan, 2014; Meyer et al., 2015). Burnout syndrome has significant implications for pediatricians and health care institutions. However, studies on this issue are scarce, especially in the Middle East.
Studies conducted in other contexts show that a major source of pediatricians’ burnout is a challenging work environment (Kotzer et al., 2006). Authoritarian leadership, excessive rules and policies, limited autonomy over work, and restricted interaction and tension among colleagues generally lower worker morale, increase stress, and lead to pediatricians’ burnout (Spinetta et al., 2000). Role ambiguity (i.e., uncertainty or lack of understanding regarding job responsibilities, expectations, and goals) is a significant contributor to stress, which causes burnout long term (Bruce, Conaglen, & Conaglen, 2005; Burnard, 1991; Hazinski, 2013). Job dissatisfaction is another element that acts as both a contributor to and consequence of pediatric burnout (Chopra, Sotile, & Sotile, 2004).
Two main observations can be drawn from the literature review. First, work environment contributes significantly to burnout among pediatric staff and second, research is needed to identify possible antecedents of burnout. Many workplace and organizational factors can affect burnout but have not been studied adequately. Addressing such factors is valuable to limit worker burnout.
Relationship Between Organizational Structure and Burnout
Burnout is a condition of exhaustion caused by employees’ continued exposure to challenging work and resulting stress. The person–environment fit theory proposes that organizational factors which cause stress for employees over time play a critical role in the incidence of occupational burnout (Estryn-Béhar et al., 2007; Maslach & Jackson, 1985). A possible factor that can trigger burnout for pediatric nurses and result in poor person–environment fit is organizational structure. Organizational structure depicts how a firm operates, organizes, and arranges itself, and it generally pervades the company (Oldham & Hackman, 1981). Researchers have delineated some dimensions of organizational structure: integration, instrumental communication, centralization, formalization, and promotional opportunity (Lincoln & Kalleberg, 1990). These dimensions highlight resource availability for workers; resource availability protects employees from burnout but resource deficiency contributes to employee strain and burnout (Leiter & Maslach, 1988).
Centralization refers to the distribution of power in an organization (C. Lee, Pillutla, & Law, 2000). A flat structure encourages workers to voice their concerns but a top-down hierarchical arrangement neither encourages employees to participate in decision making nor allows employees to affect company outcomes (Lincoln & Kalleberg, 1990). Instead of centralization, this research uses the phrase “participation in decision-making.” When workers are allowed to participate in decision making, they believe they are valued by the organization and have authority over occupational matters. In contrast, lack of participation contributes to workers feeling they are part of impersonal organizations (Cordes & Dougherty, 1993). Having little or no authority over their work lives, workers may feel powerless, threatening their emotional well-being. Hence, it is hypothesized:
Information received by workers regarding organizational issues, processes, and their work is called instrumental communication (Mueller, Boyer, Price, & Iverson, 1994), which offers both general and specific salient information to workers, facilitating effective job performance (Shadur, Kienzle, & Rodwell, 1999). Instrumental communication clarifies the organization’s challenges and needs, and contributes to employees feeling valued by the organization. The absence of instrumental communication restrains employees, signaling they need not concern themselves with organizational affairs (Lincoln & Kalleberg, 1990; Mueller et al., 1994). When employees are uninformed about workplace challenges and needs, the risk of worker burnout increases. Hillhouse and Adler (1997) found that an antecedent of worker stress is lack of communication. Hence, it is hypothesized:
The degree of structure related to organizational rules and policies is called formalization (Bluedorn, 1982). House and Rizzo (1972) defined formalization as “the extent to which standard practices, policies, and position responsibilities are formalized explicitly” (p. 391) and as “clarity of structure, authority, and expectations” (p. 473). Formalization reduces uncertainty in the workplace and provides guidelines to employees regarding the handling of change, problems, or tasks (Lincoln & Kalleberg, 1990). Formalization supports workers by providing guidance and direction to their efforts, and eliminates ambiguous expectations. Absence of formalization can lead to confusion and frustration, both of which are directly related to burnout. Hence, it is hypothesized:
Integration denotes group cohesiveness and belonging among workers (Lincoln & Kalleberg, 1990). According to Bearman (1991), integration is
the extent of social relations binding a person or a group to others such that they are exposed to the moral demands of the group. Integration may vary from complete embeddedness in a group to the pure isolate without social relations. (p. 503)
Integration alleviates loneliness, contributes to a sense of interdependence, and can lead to enjoyable, friendly work experiences. Furthermore, integration may create an organizational support system for workers (Cherniss, 1980). Support from coworkers reduces the impact of stress, preventing exhaustion and burnout (Maslach, 1982). The absence of integration can contribute to a dysfunctional workplace. Workers viewed as impersonal objects can also contribute to burnout. Hence, it is hypothesized:
Promotional opportunities demonstrate that the organization rewards workers for their skills and motivation (Curry, Wakefield, Price, & Mueller, 1986). Workers generally aspire to grow and be promoted. They want to build a career rather than simply work at a job (Cotton & Tuttle, 1986). However, employees perceive promotional opportunities differently. In the absence of promotional opportunities, employees see little or no chance of bettering themselves in the organization; their careers come to a standstill which can increase employee strain and frustration, leading to burnout. Hence, it is hypothesized:
Research is needed to determine how the characteristics of a hospital are associated with pediatric nurse burnout. The present study determined whether relationships between the concepts of organizational structure and pediatric nurse burnout exist in Pakistan. Such an analysis of this relationship addresses burnout in a developing nation, and may further expand and enrich the limited body of research on the linkage between these two concepts.
Method
Before conducting this study, the university’s Institutional Review Board (IRB) gave approval. The study surveyed pediatric nurses working in Punjab’s largest state hospital. The hospital treats approximately 1 million patients each year, employing about 200 pediatric nurses. However, at the time of the study, some nurses were on leave for various reasons. All 185 available nurses were personally provided a cover letter, questionnaire, and information about a drawing. The nature of the research, the purpose of the survey, and significance of participation were explained in the cover letter. It was emphasized that all responses were confidential; hospital administration did not have access to completed questionnaires. To increase participation in the survey, nurses who return completed questionnaires were entered into a drawing for US$25.00. Pediatric nurses who agreed to participate in the study signed informed consent documents that signified their participation in the study was voluntary; 113 completed questionnaires were returned, a 61% response rate.
Instruments
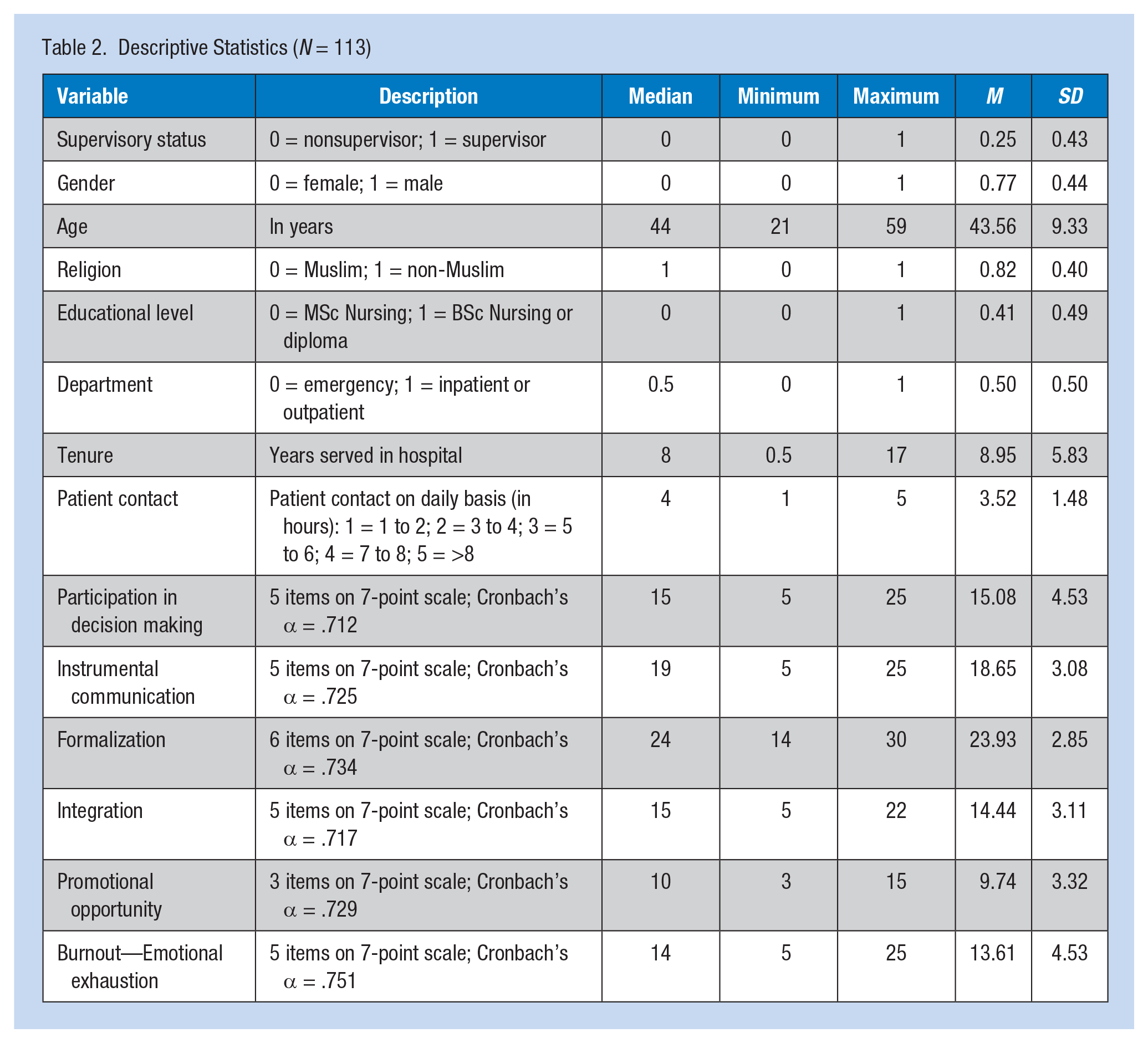
The sociodemographic attributes of supervisory status, gender, age, religion, education, department, and tenure acted as control variables in the study. Age and tenure were assessed on a continuous scale; the other variables were measured on a nominal scale. Approximately 22% of participants held a supervisory position and were supervising other nursing staff at the hospital (coded 0); the remaining 78% held no such position (coded 1). Nearly 72% of the participants were females (coded 0), and only 28% were males (coded 1). Most participants were between 21 years and 59 years of age with a mean of 43.56 years. With respect to religion, about 76% of the participants were Muslim (coded 0), 19% were Christian, and 5% were Hindu (coded 1). With respect to education, only 12% of participants had earned a master’s in nursing (coded 0), 66% had earned a bachelor’s in nursing, and 22% had earned a diploma (coded 1). About 57% of participants worked in the Emergency Department (coded 0), and 25% worked in the outpatient department and 18% worked in inpatient departments (coded 1). The tenure of participants ranged from 6 months to 17 years, with a mean of 8.95 years.
As discussed, burnout is often the outcome of intense interpersonal contact with patients (Maslach, 1982). To measure this antecedent, participants indicated the number of hours they interacted directly with patients each day using a 5-point Likert-type scale. To measure job burnout, the criterion variable, five items from the Camp (1994) scale were adopted using a 7-point Likert-type scale ranging from “never” (coded 0) to “every day” (coded 6). Participants indicated how frequently they felt emotional fatigue and consumed by work in the past 6 months. To confirm that the items loaded on the correct factor, principal-axis factor analysis with a varimax rotation was applied. The factor loading of all five items ranged from 0.5 to 0.9.
The dimensions of organizational structure, participation in decision making, formalization, instrumental communication, integration, and promotional opportunity, were predictor variables for this study and were quantified using a 7-point Likert-type scale ranging from “completely dissatisfied” (coded 0) to “completely satisfied” (coded 6). The participants indicated their level of satisfaction with each statement. From the scale proposed by Curry et al. (1986), three items measured instrumental communication, five items assessed promotional opportunities, and five items determined participation in decision making. Similarly, to measure integration, five items from the Miller and Droge (1986) scale were adopted. To create a scale for formalization, four items from the Oldham and Hackman (1981) scale and two items from the Finlay, Martin, Roman, and Blum (1995) scale were adopted. Finally, to measure the emotional aspect of burnout, five items from the Hong (2010) scale were adapted. Again, principal-axis factor analysis with a varimax rotation was applied. The factor loading of all items was above 0.30, the cutoff point.
Prior to testing hypotheses, it was essential to determine the internal consistency and validity of the measurement scales. First, the scales’ alpha coefficients and composite reliability were determined. For the six scales used in this study, the alpha coefficients ranged from .71 to .75, and their corresponding composite reliability indices were between .73 and .82. Because both reliability measures exceeded the threshold, scale reliability was ascertained. Second, the researchers calculated the average variance extracted (AVE) for the six scales to establish convergent validity. The AVE statistics were in the .51 to .66 range, confirming convergent validity (see Table 1).
Scale Validity and Reliability
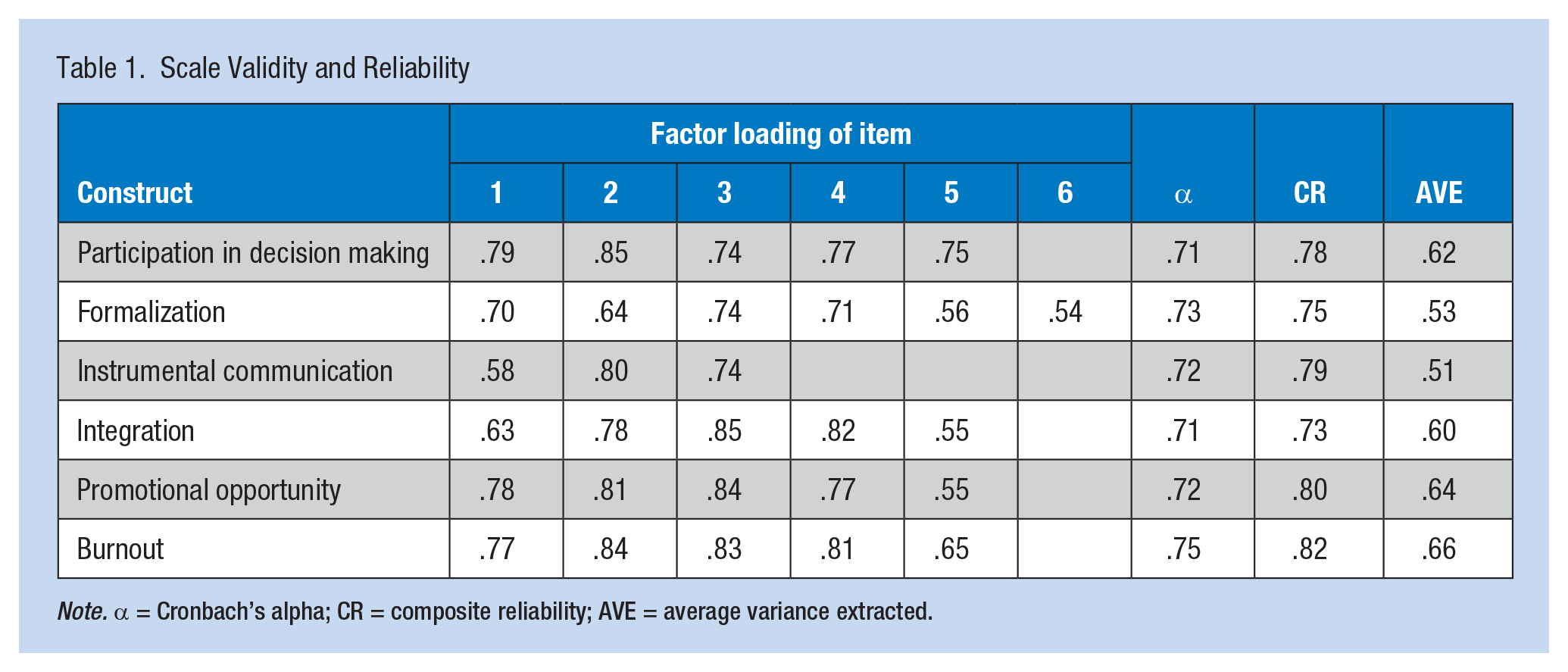
Note. α = Cronbach’s alpha; CR = composite reliability; AVE = average variance extracted.
Because the responses for both organizational structure and perceived burnout were provided solely by pediatric nurses, the occurrence of common-method bias is possible. To determine the occurrence and magnitude of this bias, Harman’s one-factor test was applied to all six scales. As expected, the results precisely yielded six factors instead of one common factor. The extracted factors had eigenvalues greater than 1.0, and the largest factor explained 21% of the variance; the explained cumulative variance of all six scales was 75%. Hence, it was concluded that this data set was not affected by common-method bias.
Results
Table 2 shows that study variables were normally distributed with similar mean and median values, and had no kurtosis and skewness. Table 3 displays Pearson’s correlation coefficients for each of the variables. Participation in decision making (r = −.38, p < .01), integration (r = −.28, p < .01), instrumental communication (r = −.33, p < .01), and promotional opportunity (r = −.35, p < .01) were negatively correlated with emotional burnout. Patient contact was positively correlated with emotional burnout (r = .16, p < .05). Quite interestingly, formalization (r = −.12, p > .05) and control variables, that is, gender (r = .04, p > .05), religion (r = −.01, p > .05), age (r = .06, p > .05), educational level (r = −.05, p > .05), tenure (r = .07, p > .05), and supervisory position (r = .11, p > .05), were not related to emotional burnout among pediatric nursing staff.
Descriptive Statistics (N = 113)
Pearson’s Correlation Matrix (N = 113)
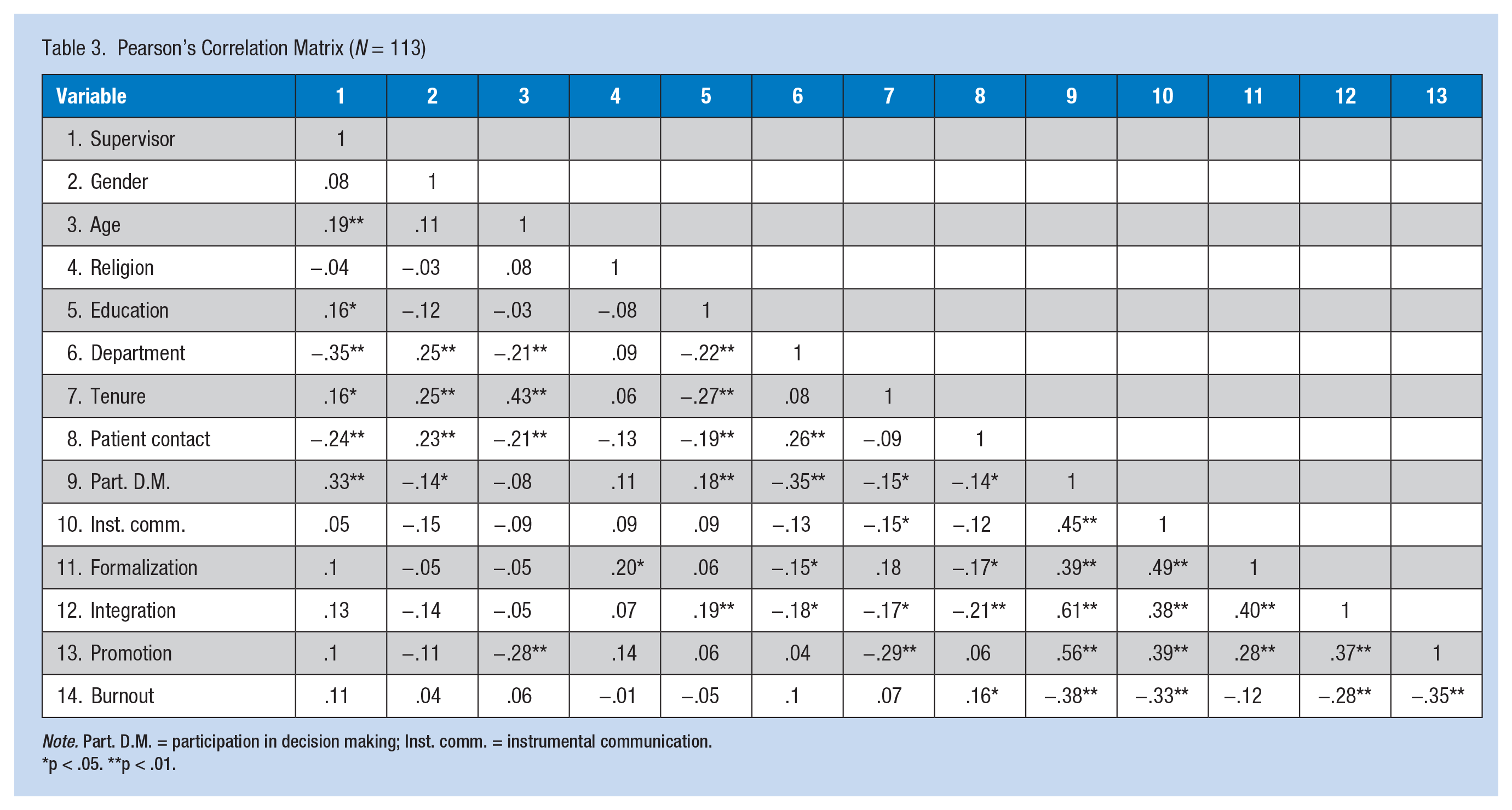
Note. Part. D.M. = participation in decision making; Inst. comm. = instrumental communication.
p < .05. **p < .01.
To determine the degree of variation in burnout explained by the organizational structural dimensions while controlling for other variables, ordinary least squares (OLS) regression was used (Table 4). Variance inflation factor (VIF) and tolerance were within acceptable limits, indicating no multicollinearity. Twenty-six percent of the variance in emotional burnout was attributed to independent study variables. Burnout experienced by supervisors was more likely than burnout among nonsupervisors. Patient contact positively affected the prevalence of burnout. The longer pediatric nurses were with patients, the more burnout they experienced. As hypothesized, participation in decision making, instrumental communication, and promotional opportunities were inversely associated with burnout; hence, H1, H2, and H5 were confidently accepted. Contrary to the hypotheses, formalization contributed to burnout, and integration was not related to burnout. Thus, H3 and H4 were rejected. In addition, standardized regression coefficients demonstrated that formalization had the least impact on burnout, and participation in decision making had the most impact on burnout.
Results of OLS Regression (N = 113)
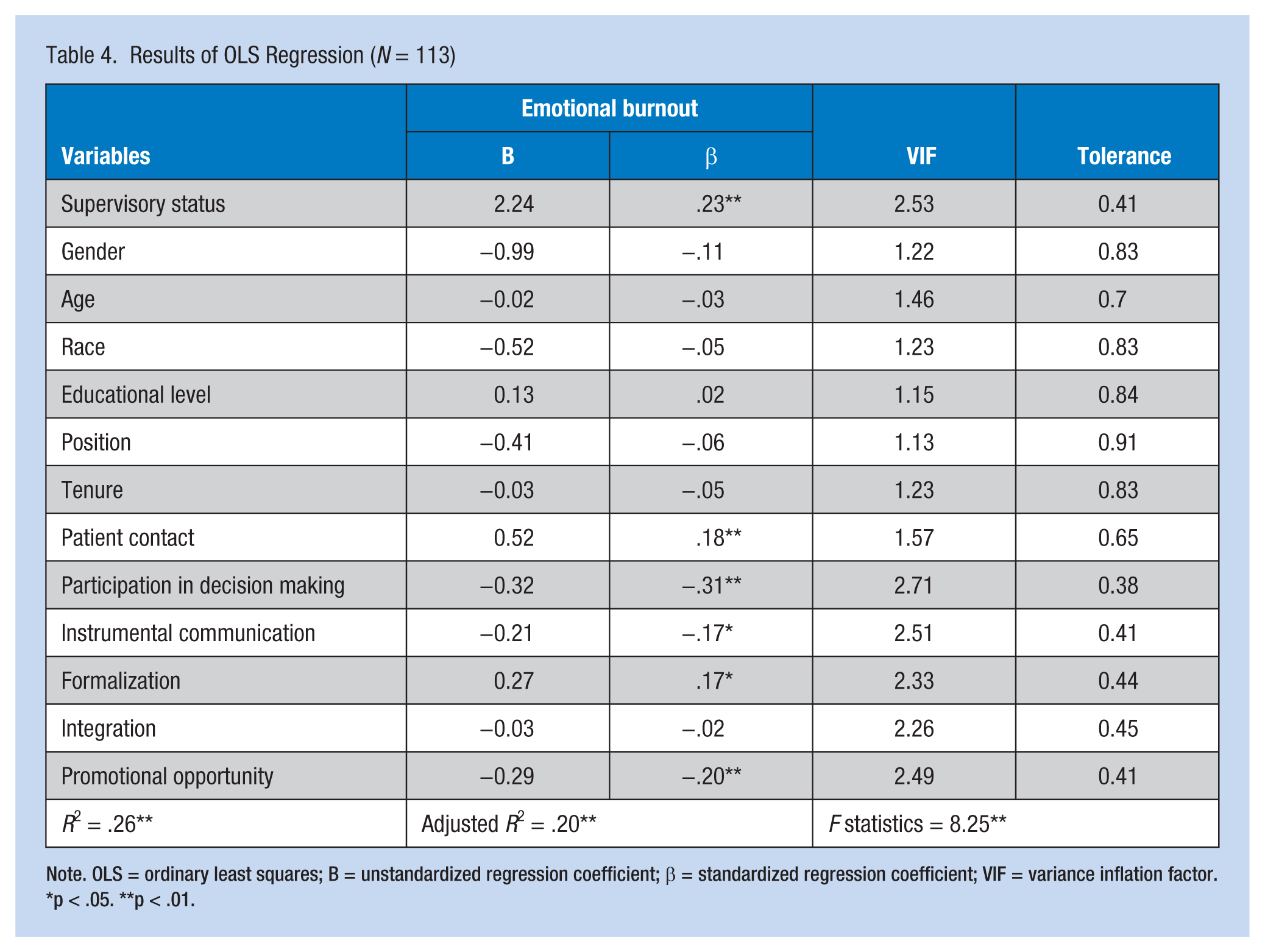
Note. OLS = ordinary least squares; B = unstandardized regression coefficient; β = standardized regression coefficient; VIF = variance inflation factor.
p < .05. **p < .01.
Discussion
The findings confirmed some hypotheses, while rejecting others. As hypothesized, emotional burnout was inversely related to participation in decision making, promotional opportunities, and instrumental communication. Participating in decision making signals nurses that hospitals respect and trust them. Allowing nurses to voice their opinions about hospital operations communicates that they are valued members of the health care team whose knowledge and skills matter to hospitals. Likewise, instrumental communication provides clarity to nurses and facilitates the performance of their jobs more effectively. In addition, effective, timely communication reduces the strain of being “in the dark” and creates rapport between the nurses and the hospital. Participation in decision making together with instrumental communication can reduce nurses’ feelings of helplessness, powerlessness, and frustration, three stressors which if experienced continually over time can result in burnout. Moreover, participation in decision making and instrumental communication provide nurses with future directions, which supports nurses in building their own future. Promotional opportunities give nurses pathways to building their careers. Without promotional prospects, nurses experience stress and resulting burnout.
Although the relationship between formalization and emotional burnout among pediatric nurses was statistically significant, the relationship was opposite to what was predicted. As discussed earlier, except for participation in decision making, a dearth of studies examined the impact of organizational structure on burnout. Therefore, it could be that either formalization actually had a positive influence on burnout, or the observed results are due to chance. Formalization refers to a multilayered organizational structure with rigid rules and regulations. High levels of formalization in the organization often shift the focus from ends to means, and may lead to bureaucratic “red tape,” a strict adherence to unreasonable rules and routines that benefit the organization, but show no concern for employees (Bozeman, Reed, & Scott, 1992). It is possible that formalization actually measured participants’ views on bureaucratic “red tape.” If this is the case, then it seems sensible that excessive and unnecessary regulations would frustrate nurses, which would gradually lead to job burnout. For instance, if through interacting with management, it was perceived that nurses were subject to various rules, policies, and training, the aim of which was not to support nurses in their work but to hold them responsible for their actions and save the hospital from lawsuits, formalization could contribute to burnout. Lacking real, meaningful guidance regarding work-related activities can lead to frustration and ultimately burnout. Hence, further research should be conducted to examine the difference in the effects of bureaucratic red tape and formalization on burnout among pediatric nurses.
Integration, contrary to the hypothesis, was not significantly linked to emotional burnout. Social support is generally believed to be a critical protector against stressors. It is possible that although hospitals promote integration and group cohesion, coworkers may not support each other. Social support demands a certain level of intimacy and trust among employees, more than that required by integration. Furthermore, prior research suggests that to avoid burnout, support from coworkers may not be as important as support from supervisors (Cherniss, 1980; Maslach, 2011). The association between integration and burnout is an underresearched area. Hence, study results may be due to chance, and integration and burnout may actually be related.
The study found a positive linkage between contact with patients and emotional burnout among pediatric nurses. This result may be due to participants surveyed. Prior studies on nursing staff found no association between these two variables (Firth, McIntee, McKeown, & Britton,1986; Whittington, 2002). Nurses differ in their perceptions of stress depending on the type and frequency of contact with patients (Firth et al., 1986), as some contacts are more stressful than others. This finding calls for additional investigation about the nature of contact with patients and the effect on burnout.
Quite interestingly, most control variables in this study, gender, religion, age, education, tenure, and position, had no significant association with emotional burnout. These findings are consistent with the “person-environment fit theory” (Estryn-Béhar et al., 2007) and provide support for the argument that organizational factors affect burnout more than personal factors (Cherniss, 1980; Maslach & Jackson, 1985). Conversely, only the control variable, supervisory status, was found to share a statistically significant relationship with emotional burnout. Compared with nonsupervisors, supervisors experienced more burnout. Supervisors have significant responsibilities and may be the first to blame when things go wrong. They deal with pressures, frustration, and disappointment more than staff nurses, and therefore their risk of burnout is greater.
This study was limited by its exploratory design. Additional research will ascertain the replicability of results in other hospitals and determine whether findings differ by type of hospital and nursing staff surveyed. Although burnout is a multidimensional construct (Maslach & Jackson, 1985), this study measured burnout from the perspective of emotional exhaustion only and did not consider its other dimensions. Future research should investigate the impact of organizational structure on burnout’s other dimensions of ineffectiveness and depersonalization as well as emotional exhaustion.
Conclusion
The work environment of health care institutions is complex. Many significant antecedents of burnout among nursing staff have not yet been explored. As discussed, the independent variables included in the study explained only a quarter of the variance in burnout. More research is therefore needed to identify other variables that affect the incidence of burnout. For instance, underutilization and boredom have been theorized to be stressors for workers, which may, over time, lead to burnout (Cherniss, 1980; Cocco et al., 2003). The contribution of such factors to burnout among pediatric nurses should be examined in further research. In addition, research is needed on the consequences of burnout among nurses (e.g., influence on organizational citizenship behavior, deviant workplace behavior, job and life satisfaction).
This study supported the “person–environment fit theory” which stresses that burnout is significantly affected by work environment factors. The results demonstrated that participation in decision making, formalization, instrumental communication, and promotional opportunity are significantly related to burnout. With time and effort, making required changes in these areas should reduce burnout among nurses. However, burnout may not be eliminated completely as other forces affect the phenomenon as well. Firth et al. (1986) emphasized the need to acknowledge possible forces that promote burnout and develop strategies to prevent burnout. The problem of burnout cannot be ignored as it has various detrimental consequences for all involved. This study also demonstrates the need for more inquiry into pediatric nursing staff burnout.
Applying Research to Practice
Burnout among nurses leads to decreased performance. Though the body of research on nursing has expanded considerably, many of the organizational sources of burnout remain under explored. Hospital administration can develop a deeper understanding of the significance of organizational structure for reducing employee burnout. The direct effect of organization structure may help administration identify how burnout can be controlled by making small changes in organizational structure. Administration is better able to examine their hospital structure, and design and implement structural changes that address burnout and performance issues among their nursing staff.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Atif Bilal is a PhD scholar at Bahria University, Islamabad, and lecturer of Management Sciences at SZABIST, Islamabad campus. His research and publication interests include organizational psychology, employee creativity, workplace violence, and organizational bureaucracy.
Hafiz Mushtaq Ahmed is a professor of management sciences at Bahria University, Islamabad. He holds a PhD in management sciences. His research work focuses on organizational behavior, strategic management, and workplace violence.