
Abstract
Metabolic syndrome is a continuing problem in the United States, and the Hispanic population is at increased risk of developing complications from this disease process. Many of the workers at a South Jersey yacht-building company are Hispanic, and a culturally sensitive education program was implemented to improve their overall health. Program assessments included the Latino Dietary Behavior Questionnaire (LDBQ), anthropomorphic measurements, and laboratory studies both pre and post intervention. The intervention included a Spanish-language lecture on metabolic syndrome and healthy nutrition, followed by an interactive culturally appropriate cooking demonstration for the participants and their significant others. Program participants showed reductions in body mass index, blood pressure, lipid levels, and hemoglobin A1c, and more knowledge of healthy nutrition as measured by the LDBQ. This finding supports culturally sensitive education programs to improve the health of Hispanic populations.
Keywords
The World Health Organization (WHO) defines metabolic syndrome as a constellation of disease processes that include insulin resistance, dyslipidemia, hypertension, and obesity; insulin resistance is the key component (Huang, 2009). The International Diabetes Foundation (IDF) definition focuses on obesity rather than insulin resistance. The concept of central obesity is also central to the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) definition (Huang, 2009). Current guidelines are appropriate for treating the Hispanic population; however, an interdisciplinary approach, sensitive to the financial and cultural needs of Hispanic individuals, is necessary for optimal outcomes (Haynes, Pruitt, Watt, Parker, & Price, 2010).
Metabolic syndrome is a continuing problem in the United States as it raises individuals’ risks for heart disease, stroke, and diabetes (Ford, 2005). Although all populations are affected, Hispanic individuals are at increased risk of developing this disorder. Considering that 75% of workers in the target population are Hispanic, the potential health risks are substantial. Individuals with metabolic syndrome often lack basic knowledge to improve their health. Educational efforts should be tailored to their level of understanding, and core concepts must be presented with cultural sensitivity to improve worker buy-in and achieve lasting behavior change. Research has shown that when Hispanic individuals with metabolic syndrome are offered culturally sensitive education and health care, they had a significant improvement in “systolic blood pressure, diastolic blood pressure, fasting blood sugar (FBS), HgbA1c, LDL cholesterol and cholesterol ratio” (Haynes et al., 2010, p. 89).
Significance of Metabolic Syndrome
Untreated metabolic syndrome can devastate human health. According to the American Heart Association (AHA; 2015), 48.3% of Hispanic American men have cardiovascular disease, 2.8% have suffered a stroke, and 43% have pre-diabetes. These statistics are a significant increase from 2013 when 33.4% of Hispanic men had cardiovascular disease and 38.2% had pre-diabetes (AHA, 2013). The incidence of stroke in this population has remained unchanged. Access to health care and education on lifestyle modification can minimize these statistics.
According to the Centers for Disease Control and Prevention (CDC), 53 million Hispanic/Latino individuals lived in the United States in 2011 (Lennie, 2006). Metabolic syndrome poses a significant health risk for this population as a whole and will continue to increase morbidity and resulting health care costs. Compounding this problem are many Hispanics who do not speak fluent English, have no reliable transportation, or have limited access to health care.
The yacht-building company employed approximately 650 Hispanic workers. The overall health care costs for individuals with metabolic syndrome are 62% higher than the health care costs for individuals without the disease (Boudreau et al., 2009); the ability to mitigate those costs could significantly decrease the health care budgets of small family-owned businesses. Education is needed to support individuals in making lifestyle changes to minimize the effects of metabolic syndrome. Providing culturally sensitive education is essential to improving and maintaining the overall health of this population (Rosal et al., 2011).
Review of the Literature
The Hispanic population is at increased risk of developing metabolic syndrome due to lack of knowledge and self-management skills. In addition, this population has limited access to health care, lacks reliable transportation, may not speak fluent English, and may experience cultural differences regarding body image, care of the sick, and dietary habits (Haynes et al., 2010). A strong body of evidence supports the need for a culturally sensitive nutritional education program that decreases the prevalence of metabolic syndrome in this population. Multiple studies have examined interventions that reduce central obesity, minimizing the risk of developing type 2 diabetes (American Diabetes Association [ADA], 2013), and mitigating cardiovascular risk by decreasing the intake of sodium, saturated fat, and trans fats (Grundy, Hansen, Smith, Cleeman, & Kahn, 2004) by the target population. Effective interventions must be culturally sensitive (Haynes et al., 2010) and take into account literacy, finances, and access to health care.
Haynes et al. (2010) conducted a study using Spanish-speaking providers and culturally sensitive educational materials to improve the health of a small Hispanic population in rural South Carolina. Targeted education sessions included information about hypertension, hyperlipidemia, obesity, and diabetes. Barriers to care were removed by providing care locally and being sensitive to language, literacy, and the costs of treatment. The study demonstrated significant improvements in “systolic blood pressure, diastolic blood pressure, FBS, Hgb A1c, LDL cholesterol and cholesterol ratio” (Haynes et al., 2010, p. 89).
Hispanic cultural norms differ from those in the United States. For example, Lindberg, Stevens, and Halperin (2013) explained that Hispanic women believe obese children are healthy and thin children are ill. The authors found that “eating is a culturally sanctioned form of stress reduction, and eating bread or sugar is, in fact, a common home remedy” (Lindberg et al., 2013, p. 2). Lindberg et al. (2013) also reported that many Hispanic cookbooks do not have exact measures and terms for specific measurement tools do not exist in Spanish. Understanding these cultural differences is essential when discussing weight loss and health education with Hispanic clients.
The Latinos en Control study offered multiple education sessions that included disease management as well as cooking classes with interactive participation. Literacy and cultural issues were addressed using picture-based food guides and interactive activities that focused on relevant aspects of Latino culture (Rosal et al., 2011). The Latinos en Control study showed that culturally sensitive interventions can significantly increase “diabetes knowledge at 12 months (p = 0.0001), blood glucose self-monitoring (p = 0.02), and diet, including dietary quality (p =0.01)” (Rosal et al., 2011, p. 838). Rosal developed the Latino Dietary Behaviors Questionnaire (LDBQ) for this study. The LDBQ was found to be valid, one of the few instruments developed for a Hispanic population (Rosal et al., 2011). For these reasons, it was chosen to measure the population’s progress in this project.
Cooking demonstrations along with nutrition education have also been found to reduce body weight and cardiovascular risk in a mixed ethnic population study conducted at multiple offices of the Government Employees Insurance Company (GEICO). Mean body mass index (BMI) dropped from 33.5 to 32 and mean low-density lipoprotein (LDL) dropped from 109 to 96 over the 18-week study. The control groups showed no significant change (Mishra et al., 2013). This particular study is significant because it was one of the few conducted in a workplace.
Purpose of Project
The goal of the intervention was to decrease the effects of metabolic syndrome on the target Hispanic population by providing an education session that explained the metabolic disease process, potential health risks, and methods to improve overall health. The intervention used a culturally sensitive approach to increase the population’s knowledge of metabolic syndrome and self-care techniques required to reduce or prevent negative outcomes.
Project Plan
The project began with a risk assessment that confirmed the need for the intervention. The stakeholders included the company owners, the chief financial officer, the vice president of human resources, and key department supervisors. The stakeholders identified threats and barriers to employee health. The intervention was designed to mitigate these issues.
Setting
A family-owned yacht-building company in New Jersey was the setting for this practice change. Data were collected at the onsite occupational health clinic, and the educational intervention was offered at locations convenient for the workers to encourage attendance. All administrative tasks for this practice change were completed at the manufacturing facility.
Target Population
The Hispanic workers at this company were the chosen population for the intervention. The company employs approximately 1,000 workers, and 65% of the workers were of Hispanic origin. The participants were not limited by age or gender. They ranged in age from young 20s to late 60s, and approximately 75% were male. The intervention targeted those Hispanic adults who were overweight with borderline hypertension, hyperlipidemia, or elevated blood glucose. Interested workers with any symptoms of metabolic syndrome were invited to participate in the study.
Implementation
Posters and handouts with project information were distributed to members of the target population. Those workers who had at least one indicator of metabolic syndrome and expressed interest in the intervention were recruited. The study consent form was reviewed and signed by participants, and they were instructed to complete the Latino Dietary Behaviors Questionnaire (LDBQ; Fernandez, Olendzki, & Rosal, 2011). The questionnaire was available in both English and Spanish. Rosal granted permission to use the LDBQ (M. Rosal, personal communication, March 20, 2014). The LDBQ was scored and the data entered for comparison.
Height, weight, waist circumference, pulse, and blood pressure were measured for each participant. BMI was calculated from the measurements. Blood for FBS, lipid panel, and hemoglobin A1c was drawn and sent to a hospital laboratory. The laboratory tests, anthropomorphic measurements, and LDBQ data were collected both pre and post intervention.
Once all pre-intervention steps were completed, the participants were invited to attend an educational session on metabolic syndrome and nutrition. The lecture was presented in English with live Spanish-language interpretation. An interactive cooking session followed the lecture, and traditional dishes were prepared adhering to dietary recommendations. Participants were encouraged to bring a friend or family member to these sessions, and the group dined together after the demonstration. Ample time was afforded for questions and answers. Participants were given a package of fresh vegetables, lean protein, whole grains, and a healthy Hispanic recipe guide. Post-intervention data collection occurred 5 to 6 weeks following the intervention and included anthropomorphic measurements, vital signs, the LDBQ, and laboratory work.
A modified lecture was presented at the worksite for those who could not attend the full program. Those attending the modified presentation received the food package, recipe book, and full presentation notes. For data collection purposes, those employees who attended either the full or the modified presentation were grouped together. Employees who did not participate in any educational intervention were grouped separately.
Data Evaluation
Pre- and post-intervention data were compared to determine the effectiveness of the intervention. Changes in weight, blood pressure, BMI, and laboratory values were compared to pre-intervention measures. The LDBQ data were compiled and evaluated question by question as well as aggregate scores. Group mean scores and the percentage of change were calculated for each question as well as the total LDBQ to identify trends. The percentage of change for these variables were calculated and benchmarked against the results of the Fernandez et al. (2011) study.
Outcomes
The Latino Dietary Behaviors Questionnaire (LDBQ) was administered both pre and post intervention. The LDBQ included questions on healthy dietary changes, the amount of artificial sweeteners in drinks, the number of meals eaten in a day, and the amount of fat consumed (Fernandez et al., 2011). Scores on the LDBQ improved when compared with the pre-intervention measurements for those participants who attended either of the intervention sessions.
The percent change in the mean total LDBQ score was 22.57% for the group attending the intervention. The intervention group’s mean pre-test score was 19.77 points of a possible 47 points. The group’s median score was 22 points. Scores ranged from a minimum of 11 to a maximum of 25. The intervention group’s mean post-test score was 24.23 (minimum = 19, maximum = 31, median = 24).
The group that did not attend an educational session had a percent change in the mean total LDBQ score of −7.14%. The non-intervention group’s mean pre-test score was 23.33 (minimum = 16, maximum = 28, median = 26), and the group’s mean post-test score was 21.67 (minimum = 15, maximum = 33, median = 17; Figure 1).
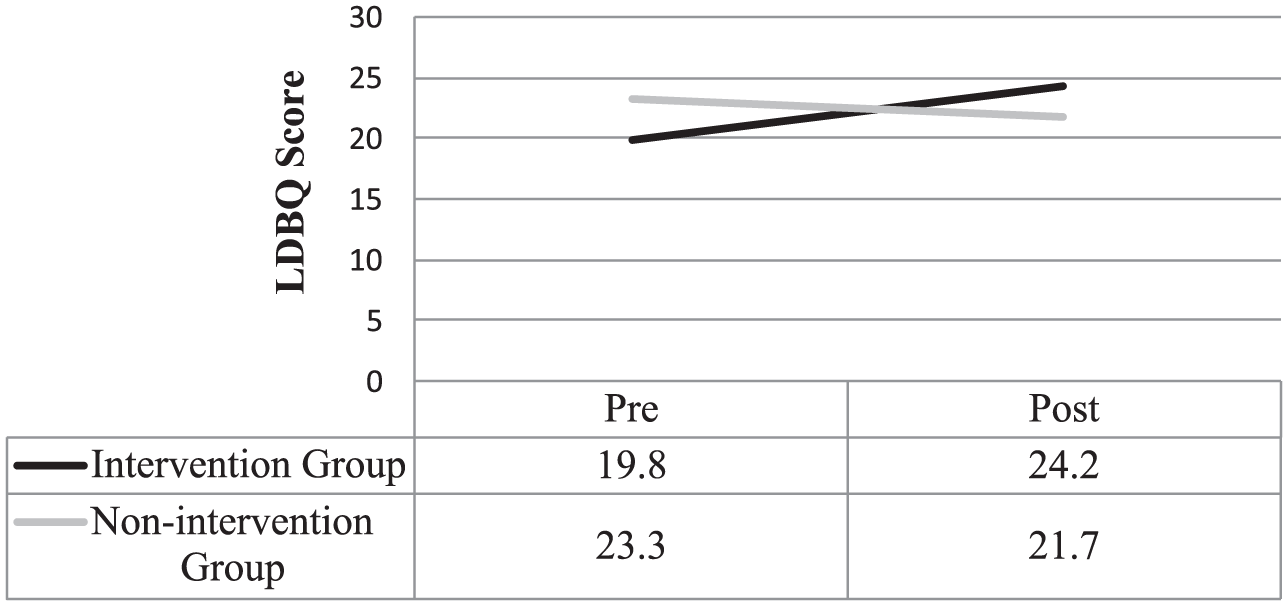
Mean total LDBQ score.
LDBQ questions that yielded the highest percentage of change were drinking skim milk (66.67%), portion control (61.54%), and healthier food choices (66.67%). The LDBQ questions that yielded the lowest percentage of change were drinking diet soda (1.75%) and the number of complete meals per day (−3.70%). Future educational programs should focus specifically on these issues. Fernandez et al. (2011) reported increased percent change for the mean total LDBQ score of 20.5%, and this percentage was the identified benchmark for the intervention. The intervention exceeded the benchmark with a mean percent change of 22.57%.
Both the intervention and the non-intervention groups had small improvements in weight, waist circumference, and BMI. Small changes were also noted in laboratory tests. Both groups showed decreases in FBS, hemoglobin A1c, cholesterol, and high-density lipoprotein (HDL). Interestingly, the intervention group showed a decrease of 2.53% in mean total LDL, but the non-intervention group showed increased mean LDL of 9.15%. In addition, the mean total triglyceride levels of the intervention group increased 30.3%, but the non-intervention group improved by −30.31%. The researchers could not identify definitive reasons for these values, but the post-intervention blood was drawn during the week following the Independence Day holiday, and dietary indiscretion may have affected the results (Tables 1 and 2).
Pre- and Post-Intervention Body Measurements and Blood Pressure
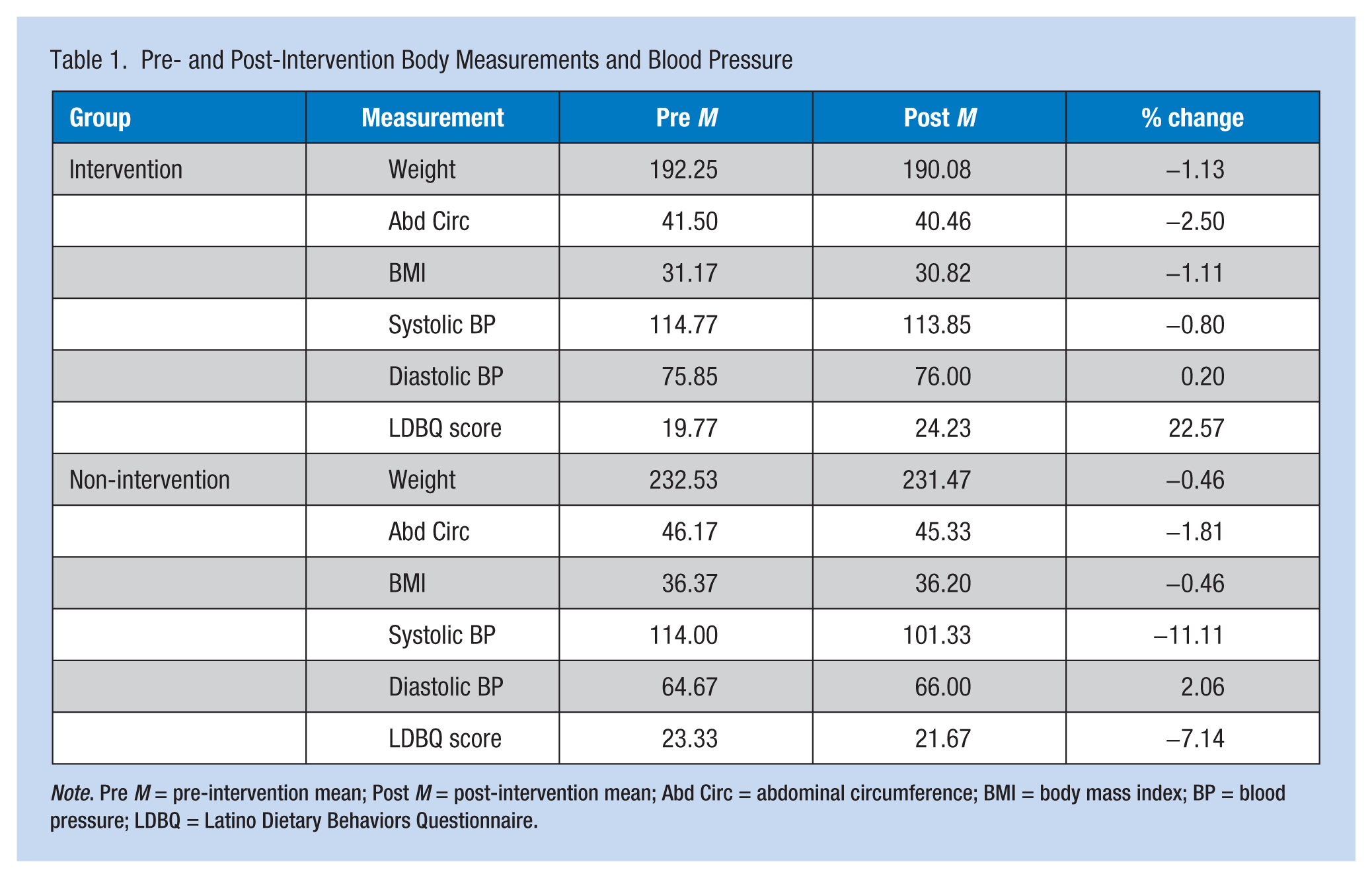
Note. Pre M = pre-intervention mean; Post M = post-intervention mean; Abd Circ = abdominal circumference; BMI = body mass index; BP = blood pressure; LDBQ = Latino Dietary Behaviors Questionnaire.
Pre- and Post-Intervention Laboratory Values
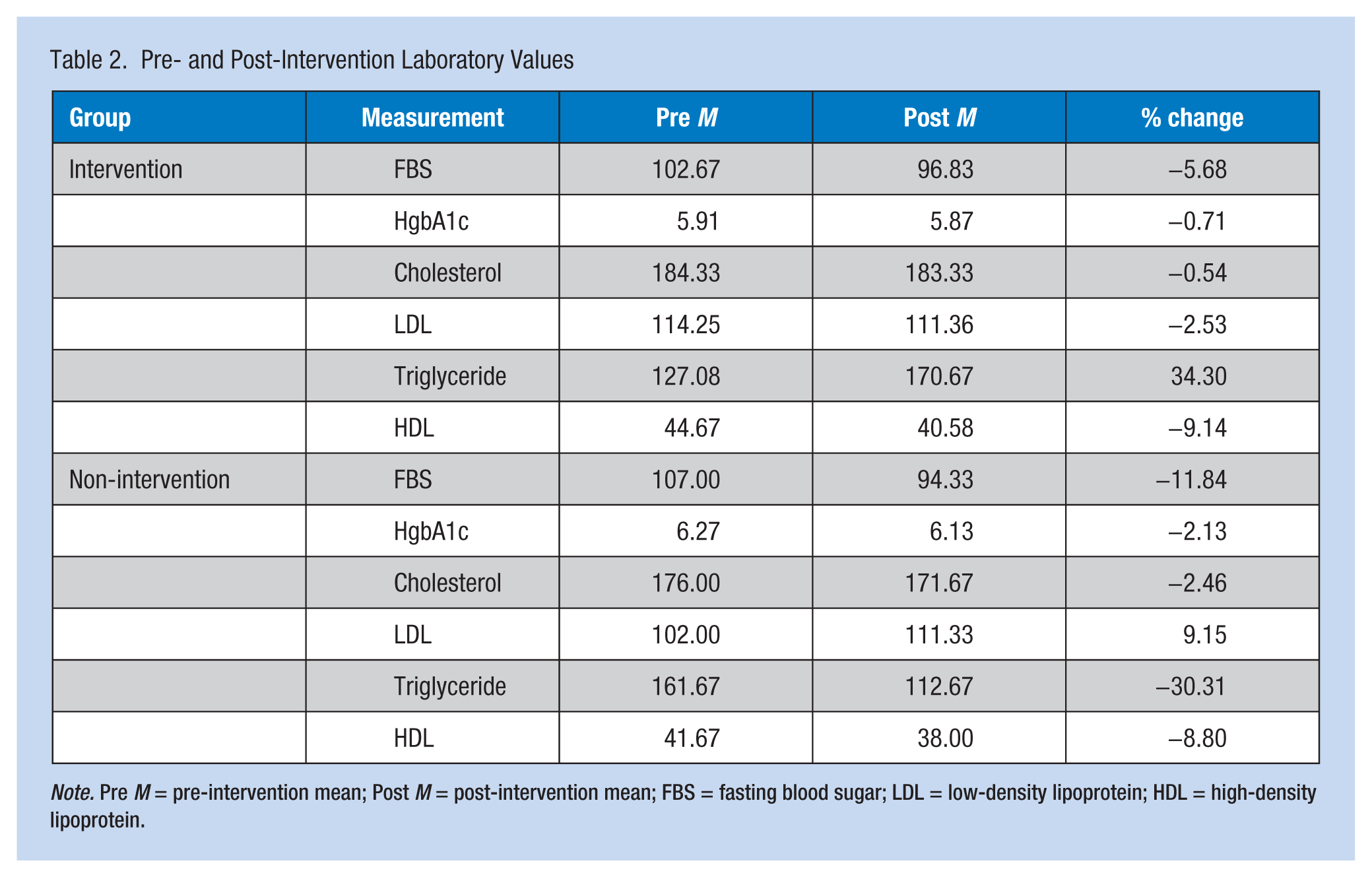
Note. Pre M = pre-intervention mean; Post M = post-intervention mean; FBS = fasting blood sugar; LDL = low-density lipoprotein; HDL = high-density lipoprotein.
Discussion
The intervention was successful compared with the benchmark. The percent change in the group mean score was 22.57% for those who attended the intervention, exceeding the benchmark of 20.5%. The score for the non-intervention group was −7.14%. According to the LDBQ scores, the intervention was most successful in improving skim milk intake, portion control, and healthier food choices. The intervention was the least successful in improving the number of complete meals per day and limiting the intake of diet soda.
Both groups showed small improvements in FBS, HgbA1c, cholesterol, LDL, and HDL, but these findings may have been limited by the short time frame between the intervention and the timing of the post-intervention measurements. The groups also had small improvements in weight, waist circumference, and BMI compared with pre-intervention measurements. Based on the study findings, this culturally sensitive education program was successful in meeting the educational needs of the Hispanic target population.
Limitations
The major limitation of this practice change project was the short period between the intervention and the final screening. Increasing the time between the education session and the post-intervention screening could result in significant improvements in all areas of measurement.
Clinical Implications
Culturally sensitive education is an effective means of improving the health of Hispanic populations. Minimizing the risk of metabolic syndrome could improve the health of these Hispanic participants, and the dietary behaviors may influence other family members as well. Educating individuals responsible for shopping and cooking meals could result in healthier meals for everyone in the household, thus extending the health benefits to everyone in the home. Those workers who live with extended families could benefit the most.
This evidence-based (EBP) change project has implications for patient education at all levels. The EBP change project included a culturally sensitive nutrition education program to address knowledge deficits regarding metabolic syndrome and self-management skills to improve health outcomes. To improve the potential for success, the project investigator met with key stakeholders to discuss the clinical problem, describe the intervention, and manage the threats and barriers to success. Effective open communication with stakeholders could provide future project leaders with the information necessary to overcome obstacles and manage successful projects.
The EBP change project was deemed successful because the intervention group exceeded the 20.5% benchmark score on the Latino Dietary Behavior Questionnaire (LDBQ). The actual mean total percent change for the intervention group’s LDBQ score was 22.57%. This finding adds to the body of nursing knowledge and supports the use of culturally sensitive education to improve health outcomes. It is imperative that nursing leaders understand the cultural nuances of their worker populations to design effective programs. In an era of scarce funding, occupational health nurses must use every resource available to address knowledge deficits that can lead to adverse health outcomes.
Occupational health nurses are in a unique position to address worker education issues on both local and regional levels. As a result of this EBP change project, the participant population may be at less risk for complications from metabolic syndrome which may improve the quality of their lives and their ability to earn sufficient incomes for their families, and minimize the money spent on health care. A healthy workforce may also improve the financial stability of the yacht-building company. Healthy workers are more productive and less of a financial drain on the company’s health insurance plan. Minimizing the company’s health care expenditures could enhance profits, which are generally reflected in stabilization of health insurance premiums and employment.
An EBP project like this one does not happen without significant interprofessional collaboration and information technology (IT) resources. The project leader met with multiple nutritionists via phone and email. Information gleaned from these meetings provided evaluations of similar programs, and needed program modifications. Local chefs planned the intervention menu and assisted with food preparation on the day of the intervention. This collaboration was essential because food safety, preparation, timing, and portion size were essential, and the project leader could then seamlessly move from food preparation to the cooking demonstration and then the meal itself. Future project leaders must look outside their professions to find community members with the diverse knowledge and experience to address aspects of the clinical problem.
The company’s IT professionals created secure network drives for data storage and assisted with the equipment needed to present a program in an off-site location. In addition, the IT professionals installed the software necessary for data collection and analysis on secure laptop computers. Using existing resources streamlined future projects as well as identified obstacles and minimized project costs.
Occupational health nurses must understand the cultural nuances of their worker populations. For example, in the United States, the term Hispanic is often misinterpreted as meaning Mexican. Nurses who do not understand this distinction may try to educate Central American or Caribbean Hispanic workers about tacos, burritos, and corn tortillas, none of which are part of their traditional diets. This misunderstanding could lead to ineffective education programs and adverse worker outcomes.
Knowing the cultural aspects of the participant population was essential in developing a program that addressed their needs. Many of the participants were surprised that they were at risk for metabolic syndrome. The nutritional component of the education session included the concept of eating whole grains, a foreign concept to many of the participants. It was interesting to note that many Hispanic cookbooks do not have ingredient measurements (e.g., the term cup could mean any size cup found in the pantry and not the eight-ounce measure that Americans use; the terms teaspoon and tablespoon are also not used culturally in this population). Understanding this, the occupational health nurse should provide a visual demonstration of measurement devices used in American kitchens.
It is easy for the occupational health nurse to tell workers with metabolic syndrome to reduce their carbohydrate and fat intake. The project leader often heard other professionals tell Hispanic workers to eliminate rice, beans, and tortillas from their diets. These professionals were frustrated by the poor progress these workers reported. This project used a different approach and remade traditional dishes using whole grains, portion control, and healthier cooking techniques. The presentation was delivered in Spanish and the slides were very visual. This approach was well received by the participants, many of whom were illiterate. This study demonstrates the importance of tailoring programs to the needs of the workers.
The concept of whole grains was foreign to the participant population, and they all agreed that brown rice was not used in their homes. Many traditional dishes were fried, so grilled alternatives were showcased. The population was appreciative that the foods offered were affordable on their incomes. Overall, the results were positive, and the participants remained engaged even after the intervention. Quite often, participants would come down to the office at the project’s site to discuss their laboratory results or ask questions about metabolic syndrome or nutrition.
The participant population came from regions that prepare drinks and desserts with significant added sugar. The researchers acknowledged participants’ “sweet tooth” but offered less sugar-laden alternatives. The presentation included slides depicting the amount of sugar in common foods using stacks of sugar cubes. This visual drew a response from the participants and generated a number of questions during the educational session. The appetizer and dessert courses included foods prepared with agave in place of sugar. The participants voiced their willingness to use these techniques, and if their changes in diet became permanent, their overall health should improve.
Concepts related to culturally sensitive education should be included in basic nursing curricula as well as workplace in-service programs. If these programs emphasized the value of culturally sensitive communication, every client interaction could be positively affected. Health education programs could be designed with cultural sensitivity to help audiences connect with the message being delivered, improving client knowledge, buy-in, and health outcomes. Better health outcomes may potentially minimize the strain on the U.S. health care system.
Future Projects
Education is needed in the workplace. Additional interventions for interested Hispanic employees and their families will be scheduled in the future. This program could be adapted for other cultural groups at the workplace and in the surrounding community. The use of newly available point of care testing could decrease the cost of future interventions. This concept could also be applied to a television or Internet-based production, thus providing cost-effective education to a larger audience.
Conclusion
Metabolic syndrome is a significant health problem in the United States, and the Hispanic population is at increased risk of complications. Language, transportation, and differences in culture are all barriers to educating the Hispanic population. Culturally sensitive interventions have been shown to be successful in educating the Hispanic population about metabolic syndrome and associated nutrition.
A culturally sensitive nutrition and metabolic syndrome education program was offered to a target population of Hispanic workers at a yacht-building company. The workers were screened using the LDBQ. Height, weight, waist circumference, fasting glucose, lipids, and HgbA1c were measured prior to the educational intervention. The intervention, held at a site convenient for the participants and their friends or family to facilitate attendance, consisted of a Spanish-language lecture on metabolic syndrome and nutrition, cooking demonstration, and a traditional meal prepared using whole grains and healthy cooking techniques. A family-style meal was served, and participants were given healthy Hispanic recipes and a package of lean protein, a whole grain, and a fresh vegetable. The LDBQ, anthropomorphic measurements, and laboratory tests were completed approximately 5 to 6 weeks post intervention. The data were compiled and showed improvement in LDBQ scores and decreases in blood glucose, HgbA1c, and lipids.
Culturally sensitive nutrition education is an effective way to minimize risk and improve healthy behaviors in the Hispanic population. This form of education eliminates barriers to care and creates an environment of mutual understanding. The intervention is cost effective and can be adapted to other audiences with some time and creativity.
In Summary
Hispanic workers are at risk for the development of metabolic syndrome. Barriers to health care include language, income, cultural differences. Programs that target their specific cultural needs are effective. Identifying barriers to care and planning to mitigate those barriers can improve outcomes. This model is effective in decreasing metabolic syndrome risk for Hispanic workers. Future programs could be developed using this model to address issues in various populations.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Steven Marks, DNP, RN, APN, COHN-S, FAAOHN, practices occupational health and primary care nursing at Viking Yachts, in New Gretna, NJ. He also has a private practice, and is an adjunct professor of nursing at Stockton University.