
Abstract
Rotating shiftwork is common for air traffic controllers and usually causes sleep deprivation, biological adaptations, and life changes for these workers. This study assessed quality of life, the sleep, and the health of 30 air traffic controllers employed at an international airport in Brazil. The objective was to identify health and quality of life concerns of these professionals. The results identified physical inactivity, overweight, excess body fat, low scores for physical and social relationships, and sleep deprivation for workers in all four workshifts. In conclusion, these workers are at risk for chronic non-transmittable diseases and compromised work performance, suggesting the need for more rest time before working nightshifts and work environments that stimulate physical activity and healthy diets.
Air traffic control results from complex regulations, conventions, and operational procedures determined by national and international legislation. Among the workers in the air navigation system are air traffic controllers (ATC).
In Brazil, this job is performed by military and civilian workers who rotate shifts, a common practice for ATC in the United States, Canada, Australia, New Zealand, and Brazil (Signal & Gander, 2007). This workshift model is a way to minimize the effects of chronic desynchronization of the circadian clock (Comperatore & Krueger, 1990; Dahlgren, 1981; Luna, 1997) and avoid social and physiological changes caused by permanent and consecutive workshifts without affecting ATC phraseology (e.g., standardized global communication between ATC and pilots by radio) proficiency (Hopkin, 1988; Luna, 1997; Melton & Bartanowicz, 1986).
Technology used in air traffic services improves operations, providing greater efficiency by adequately attending to increasing demands. However, this system is dependent on human factors that require knowledgeable and healthy professionals to accomplish their assigned duties, ensuring system security.
Workers, in general, adapt to shiftwork, but adaptations depend on endogenous factors such as age, gender, and personality as well as exogenous factors such as task type and social and environmental conditions to ensure that changes do not damage worker health (Vincenzo, Martoni, & Cicogna, 2003).
Sleep deprivation contributes to workers’ fatigue and has been associated with work-related accidents and the development of chronic diseases (Tucker & Folkard, 2012). Thus, studies on sleep, working environments, and health conditions of ATC are fundamental, as these factors are related to workers’ adaptations to shiftwork and work performance.
This study investigated quality of life, sleep, and health of ATC working at an international airport in the state of São Paulo, Brazil, to assess the impact of shiftwork on these variables.
Method
Of 52 ATCs at an international airport in the state of São Paulo, Brazil, 30 ATC voluntarily agreed to participate and signed a Term of Free Consent. All ATC resided in the state of São Paulo in Brazil. These ATC work rotating shifts, 6-hour shifts with 12-hours off between shifts for 4 days followed by 2 days off work.
Questionnaire
The auto-answered structured questionnaire was used to gather data including identification variables (name, gender, date of birth, marital status) and socioeconomic status (social class and education). The researchers also used the Economic Classification Criterion Questionnaire of Brazil (Brazilian Association of Research Companies [ABEP], 2006).
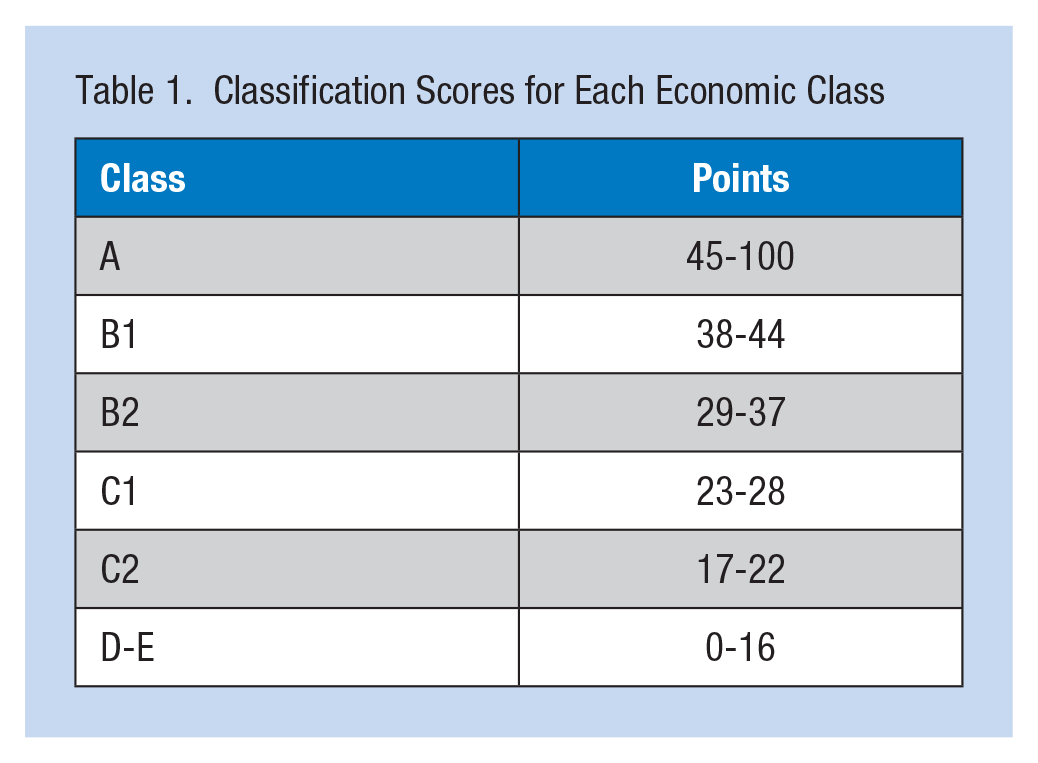
This questionnaire measures the purchasing power of homogeneous groups of individuals, categorizing their economic class from A to E (i.e., A class has the greatest purchasing power and E class has the lowest purchasing power). The questionnaire measures the number of electronic devices (e.g., computers, TVs, dishwashers, refrigerators, microwave ovens, DVD players, and washing machines and dryers), number of vehicles and motorcycles, number of housekeepers, and number of existing bathrooms in the household of each interviewee. The survey also evaluates the education of the head of the family, housing conditions with regard to sanitation, and the existence of paved roads. All variables are assigned a score that are added together and range from 0 to 100 points creating classifications as shown in Table 1.
Classification Scores for Each Economic Class
Quality of Life
The ATC perception of quality of life was measured using the WHOQOL-Brief questionnaire (World Health Organization Quality of Life Group, 1998) which consists of 26 items, with subscales of Physical Domain, Psychological Domain, Environmental Domain, Social Relationships Domain, and Overall Quality of Life. This methodology was suggested by the World Health Organization (WHO).
Physical Activity
Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ), Version 8 Short Form based on a normal week. This questionnaire was developed by the WHO and validated in Brazil and other countries (Ainsworth, Macera, & Jones, 2006; Baranowski, 1988; Craig et al., 2003; Fogelholm et al., 2006; Hallal, Victora, Wells, & Lima, 2003; Mader, Martin, Schutz, & Marti, 2006; Matsudo et al., 2001; Pardini et al., 2001). This study sample was classified into four levels of physical activity (sedentary, insufficiently active, active, and very active) by Metabolic Equivalent in minutes per week (MET/week) of physical activity.
Nutritional Status
To measure nutritional status, the researchers calculated body mass index (BMI)—body mass (kg) divided by participant height squared (m2). The researchers adopted classification criteria proposed by the WHO (WHO/Food and Agriculture Organization Expert Consultation, 2003):
Underweight (BMI < 18.5),
Normal weight (18.5 < BMI < 24.9),
Overweight (BMI > 24.9).
Body mass was verified using international standards (Gordon, Chumlea, & Roche, 1991) on a calibrated digital scale (Healthmeter brand) with capacity up to 150 kg. Height was measured using a wall stadiometer with precision of 0.1 cm (Sanny brand).
Body Composition
Body composition was assessed using a tetrapolar bioelectrical impedance (model BIA 310e, Biodynamics Body Composition, Seattle, Washington, USA). Surface electrodes were placed at four anatomical points: back, right wrist, chest, and right ankle (Heyward & Stolarczyk, 2002). The classification criteria to assess percentage of body fat were suggested by Lohman, Roche, and Martorell (1994). To decrease confounding, the following protocol was required: no eating or drinking for 4 hours before the test, no physical activity during the previous 12 hours, empty bladder, no alcoholic beverages for 48 hours, and no diuretics in the 7 days preceding the test (Heyward & Stolarczyk, 2002).
Blood Pressure
To measure systolic (SBP) and diastolic blood pressure (DBP), the researchers used an automatic device (Omron brand), previously calibrated; blood pressures were measured after the participant spent 15 minutes in a sitting position. Blood pressures were classified using the Brazilian Guidelines for Hypertension (Brazilian Society of Cardiology/Brazilian Society of Hypertension/Brazilian Society of Nephrology [SBC], 2010).
Sleep
Sleep time was estimated by the Munich Type Questionnaire for shift workers (Juda, Vetter, & Roenneberg, 2013) using minutes of sleep the night before each workshift. Thus, the researchers measured four sleep times for Shift 1 (6:00 a.m. to 12:00 p.m.), Shift 2 (12:00 p.m. to 6:00 p.m.), Shift 3 (6:00 p.m. to 12:00 a.m.), and Shift 4 (12:00 a.m. to 6:00 a.m.).
Data Collection
The questionnaires used for data collection were presented individually to ATC at the workplace and included an explanation of the study and the questionnaire. The questionnaires were returned to the researchers by the participants within 30 days.
The research was approved by the Research Ethics Committee of the Faculty of Medical Sciences, State University of Campinas (UNICAMP), under No. 62824, complying with the norms of Resolution 466/2012 for research on human subjects and authorized by Empresa Brasileira de Infraestrutura Aeroportuária.
Data Analyses
The sample was assessed statistically for normality using the Shapiro–Wilk’s test. Once adherence to the Gauss curve was confirmed, the data were treated as parametric using Pearson and Spearman correlation tests to determine the association between variables (p < .05). The statistical analysis also included a descriptive analysis based on measurements of central tendency, dispersion, and distribution of frequencies in accordance with the profiles of study individuals. The statistical software Bioestat 5.0 was used for all analyses.
Results
Thirty ATC participated in the study (e.g., nutritional status, body composition, and blood pressure measurements). Of these, 27 ATC responded to the questionnaires about quality of life, socioeconomic data, and level of physical activity and 23 responded to the sleep questionnaire.
The ATC were 42 years of age on average, 70% of the sample was male, 46.7% was married; they had completed more than 15 years of schooling (56.7%), averaged 8 years in the job, and were most likely to come from social class B1 (46.7%) in an index that range from A1 (higher-income class) to E (lower-income class). Regarding the level of physical activity, the researchers found that 43.3% of the ATC were sedentary or insufficiently active and 56.7% were active or very active (Table 2).
Distribution of Socioeconomic Variables of ATC, São Paulo, Brazil, 2013
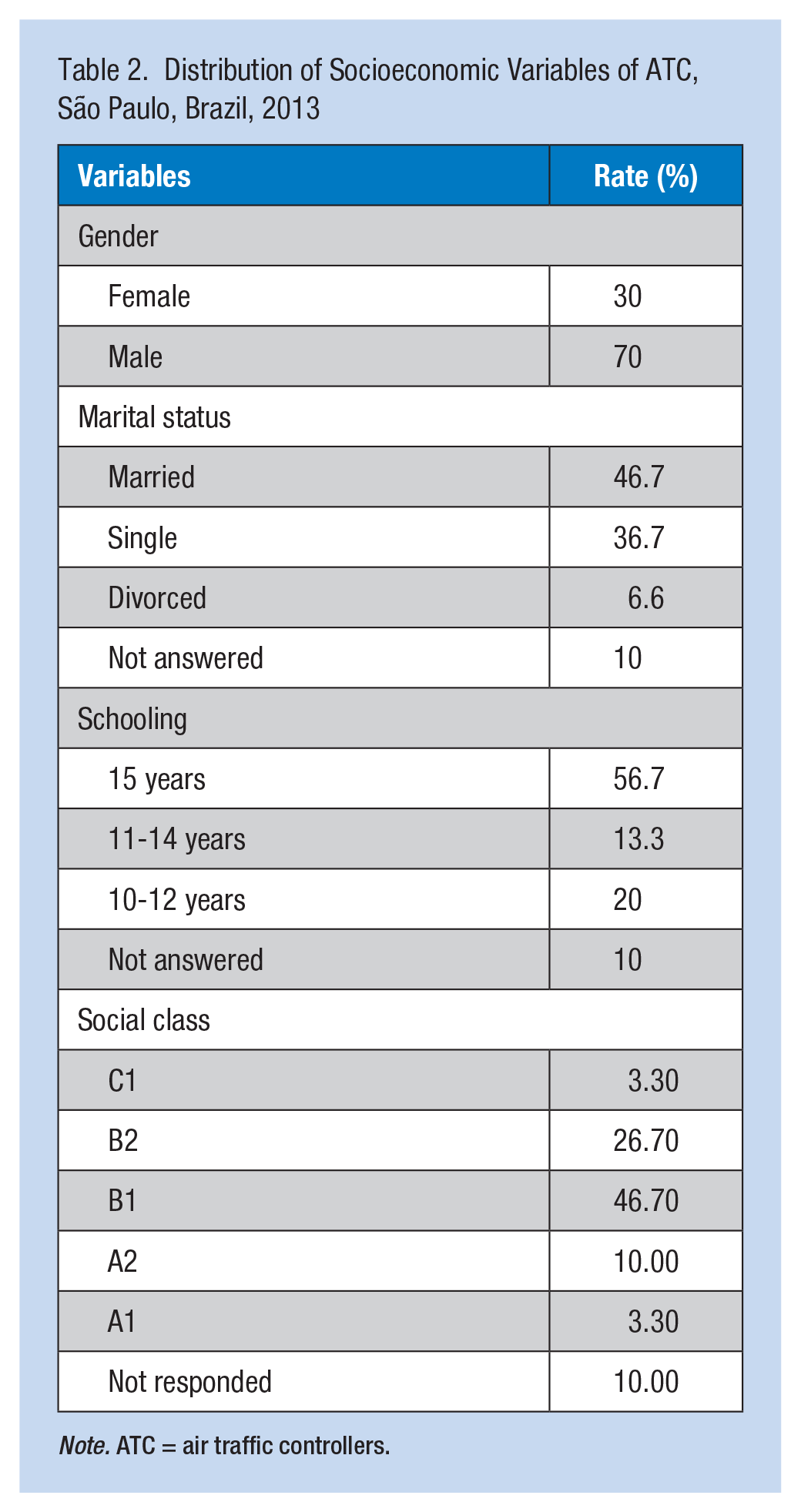
Note. ATC = air traffic controllers.
The variables related to health, quality of life, and physical activity are presented in Table 2, with a BMI average of 26.37 (±3.53 SD) indicating overweight. The distribution showed that 76% of the participants were overweight and obese. Body mass index showed an average of 27.35% (± 5.76 SD), above-average value of normalcy, with 47% of ATC showing excess body fat, putting participants at risk of developing obesity-related diseases. Blood pressure showed average values within the normal range. However, 20% of ATC had values greater than 140/90, indicating hypertension Stage 1 (SBC, 2010).
Overall quality of life showed the highest average value of 68.05 (±17.44 SD) and the physical domain showed the lowest score of 55.29 (±10.45 SD). The average values for METs (metabolic equivalents per week) were close to the minimum values delineated by the WHO (2010), higher than 1,200 METs. However, a high rate of sedentarianism and insufficiently active participants contributed to this finding.
Sleep hours were shorter on working days with the average being 366.58 (±52.42 SD) minutes compared with days off work averaging 488.60 (±136.30) minutes (Table 3). The correlation analysis showed that longer sleep hours was correlated with the perception of better quality of life (r = .667) and longer sleep hours during the work week was correlated with better perception of the work environment (r = .4634; Table 4).
Descriptive Statistics of the Variables for Health, Quality of Life, and Physical Activity of ATC, São Paulo, Brazil, 2013
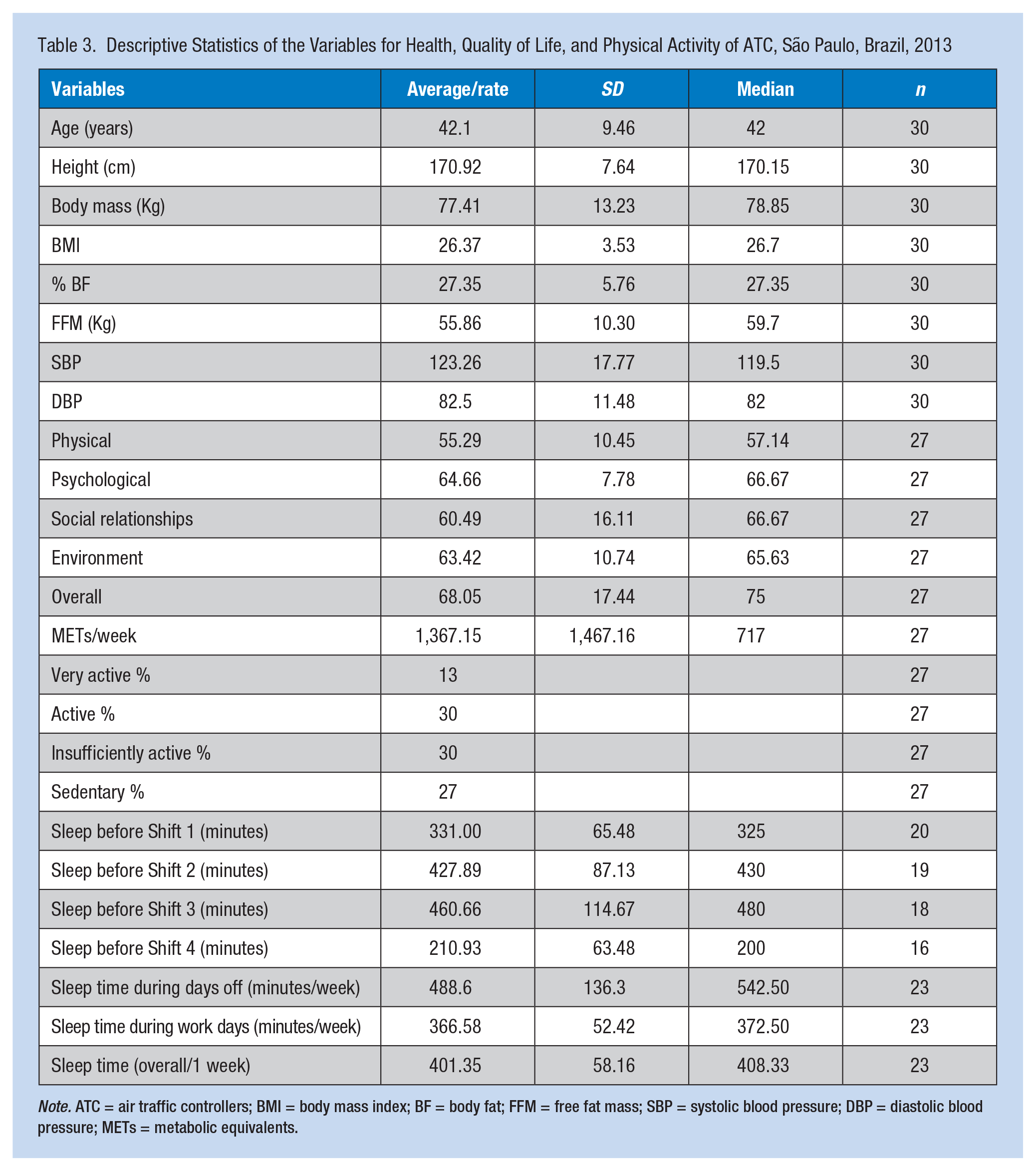
Note. ATC = air traffic controllers; BMI = body mass index; BF = body fat; FFM = free fat mass; SBP = systolic blood pressure; DBP = diastolic blood pressure; METs = metabolic equivalents.
Correlation of Variable Sleep Duration and the Quality of Life, Anthropometric, and Blood Pressure Variables for ATCs, São Paulo/Brazil, 2013
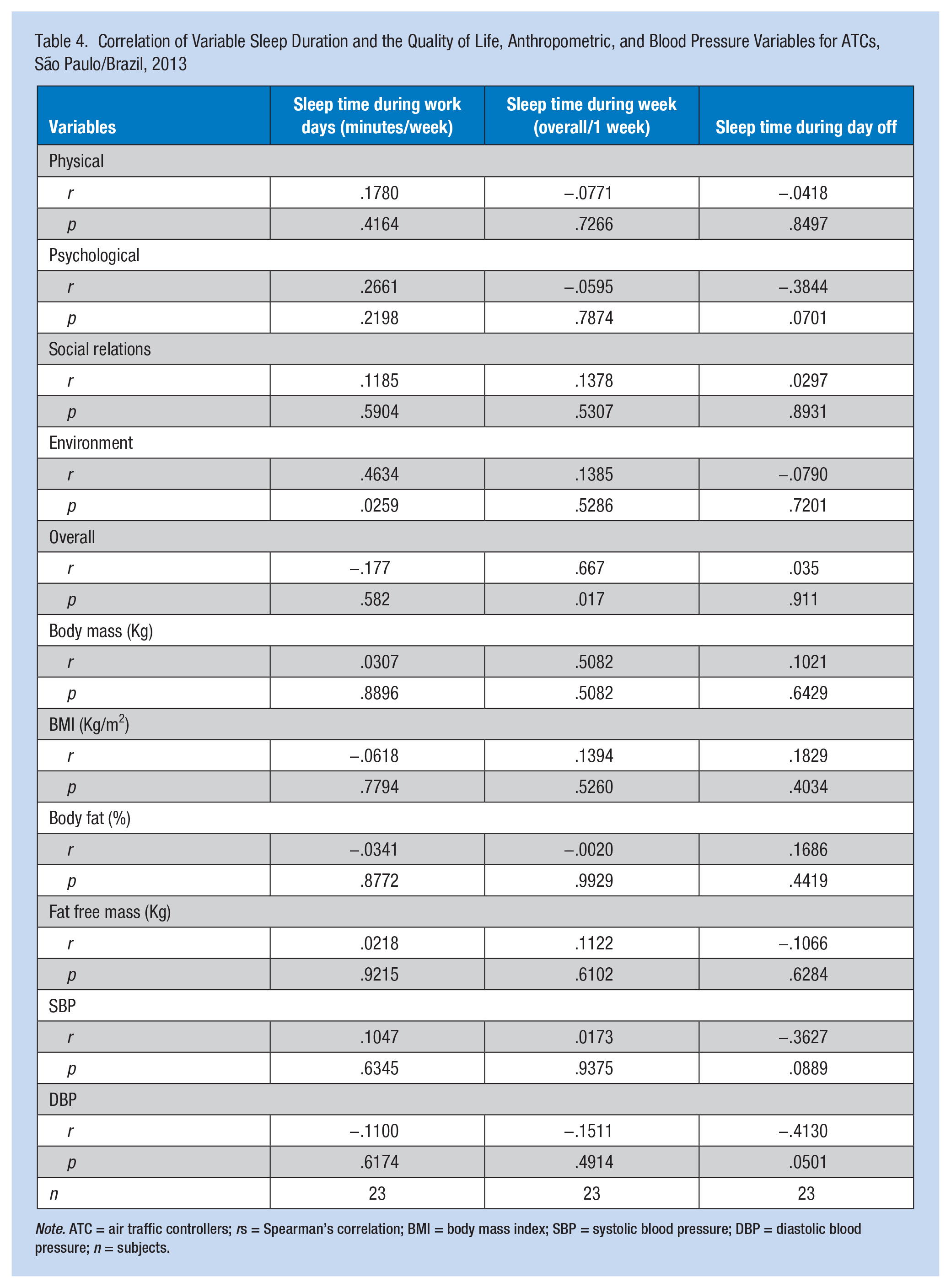
Note. ATC = air traffic controllers; rs = Spearman’s correlation; BMI = body mass index; SBP = systolic blood pressure; DBP = diastolic blood pressure; n = subjects.
Discussion
Age was considered a relevant criterion for the job of ATC, because older participants reported difficulty coping with stress and fatigue. Older workers sleep less, and their circadian rhythms are more easily disrupted by unstable sleep patterns. However, younger workers are inexperienced (Marcil & Vincent, 2000). This study identified that most ATC were male young adults, average age of 42 years, and average tenure 17 years. Socioeconomic data showed a predominance of Social Class B1, education more than 11 years with proficiency in English, and annual income between US$24,402 and US$30,503. The average socioeconomic class for the Brazilian population in 2013 was Social Class C: 8 years of schooling and annual average income of US$13,000 (Instituto Brasileiro de Geografia e Estatística [IBGE], 2014). Air traffic controllers must interact with colleagues and other stakeholders (e.g., pilots), have knowledge of applicable hardware and software as well as the work environment, and adhere to organizational expectations (Vargas, Guimarães, & Sant’Ana, 2012).
The current workshift model was 6 hours of work and 12 hours of rest, 4 days worked and 2 days off. This model is the most appropriate for ATC because it minimizes chronic desynchronization associated with slower rotations (Comperatore & Krueger, 1990; Dahlgren, 1981; Luna, 1997).
The identification of overweight, excess body fat, and blood pressure readings above the normal range in 20% of participants indicated the need to improve these health indicators. These data corroborate other studies that reported a relationship between workshift and metabolic disorders (e.g., insulin resistance, dyslipidemias, metabolic syndrome and obesity; Bechtold, Brown, Luckman, & Piggins, 2008; Fonken et al., 2010). These changes occur because circadian rhythms and metabolism are intrinsically related (Eckel-Mahan & Sassone-Corsi, 2009; Salgado-Delgado, Angeles-Castellanos, Saderi, Buijs, & Escobar, 2010; Turek et al., 2005) and may lead to the development of non-transmittable chronic diseases (NTCD) such as hypertension; diabetes mellitus (type 2); cardiovascular, cardiorespiratory, and joint diseases; and cancer (Eyre et al., 2004; Jacoby, 2004; Stein & Colditz, 2004).
Another reality of working shifts is sleep deprivation. Nightshift workers have greater sleep deprivation associated with fatigue and sleepiness, undesirable conditions for ATC which requires concentration when lives are at stake. The National Sleep Foundation (NSF; 2011) recommends minimum sleep of 7 to 9 hours per night. Signal and Gander (2007) concluded that employers should require flight controllers a minimum of 6 hours (360 minutes) of sleep before starting work, mainly when workers work the nightshift, to minimize the effects of sleep deprivation on fatigue and work performance.
This study showed that minimum sleep time was only achieved during Shifts 2 (12:00 p.m. to 6:00 p.m.) and 3 (6:00 p.m. and 12:00 a.m.). Night and morning shifts showed the shortest sleep hours (3 hours, 30 minutes and 5 hours, 50 minutes, respectively), highlighting that sleep deprivation is critical for these workers to perform their duties safely. The distance between the workplace and worker residences also determines the need for workers to awaken several hours before the workshift; the morning shift beginning at 6 a.m. is more likely to hinder night sleep (Seligmann-Silva, 1994). All of these factors combined may influence the negative perception of ATC quality of life.
According to Maciel et al. (2014), higher levels of physical activity are associated with better perceived quality of life, mainly in terms of physical aspects and social relations. This study demonstrated lower quality of life scores for physical aspects (55.29) and social relations (60.49) and a rate of sedentary and insufficiently active of 57%, similar to Maciel et al. (2013) and Maciel et al. (2014).
If the researchers considered the variation of quality of life score 0 (minimum value) to 100 (maximum value) and values in the last quartile indicate better quality of life, the Maciel et al. study calculated scores above 75, indicating positive quality of life. This high score was not found in this study; all the scores were between 55 and 68, showing a perception of poorer quality of life.
The researchers believe rotating workshifts, strict schedule, high demand for attention, and excessive responsibility contribute to ATCs’ negative perception of quality of life found in this study. According to Costa, Sartori, and Akerstedt (2006), work-related stress significantly influences individuals’ well-being and their social lives. This result also supports the low scores for social relations.
Yumang-Ross and Burns (2014) suggested that worker health, ergonomics, lighting, temperature, regular breaks, and benefits of napping could reduce workers’ fatigue and improve their quality of life. In this context, knowing that workshift may affect health, sleep, and quality of life, health professionals, including occupational health nurses, must develop programs that prioritize the prevention and early identification of health problems that could be adversely affected by work tasks, raise awareness, and encourage ATC to adopt preventive behaviors.
Conclusion
This study concluded that the group of ATC studied is overweight, has excess body fat, has elevated blood pressure, and is physically inactive, suggesting increased risk for chronic non-transmittable diseases. The sleep analysis showed significant sleep deprivation caused by working night and morning shifts, compromising worker performance, health, and quality of life.
Perceptions of quality of life were found to be more negative, mainly in terms of physical aspects and social relations. Thus, actions to ensure a minimum of 6 hours of rest before the nightshift were associated with establishing awareness and adequacy of work environments to stimulate physical activity and healthy eating habits.
Applying Research to Practice
Research shows the need to develop health promotion strategies for air traffic controllers that encourage physical activity, healthy eating, and sleep hygiene. It draws attention to the importance of adequacy of work schedules based on scientific research. Air navigation workers are at risk of developing chronic diseases and are working in a state of fatigue, compromising flight safety. This situation happens throughout the world, because the adopted scale models are not always adequate for the maintenance of workers’ health.
Footnotes
Acknowledgements
The authors thank all volunteers in the study, INFRAERO for the opportunity, and FAPESP for the financial support.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the São Paulo Research Foundation—FAPESP [2012-13884-1].
Author Biographies
Jaqueline Girnos Sonati is a nutritionist, a post doctorate in occupational health in the Nursing School at State University of Campinas, and professor in the School of Nutrition at University of Taubaté–São Paulo.
Milva Maria Figueiredo De Martino is a nurse and professor in the Nursing School at State University of Campinas–São Paulo.
Roberto Vilarta is a physiotherapist and professor of the Faculty of Physical Education, State University of Campinas–São Paulo.
Érika da Silva Maciel is a Physical Education Professor, a post doctorate in food sciences at the University of São Paulo, and a professor of the Faculty in Physical Education at Lutheran University Center Palmas–Tocantins.
Renato José Ferreira Sonati is a pilot and captain for Brazilian Airline and Research at State University of Campinas–São Paulo.
Paulo Cézar Paduan is a pilot and captain for Brazilian Airline and Research at State University of Campinas–São Paulo.
{kind=link}