
Abstract
L.Y., a 52-year-old project manager, had a series of minor epistaxis episodes while at work. After seeing his primary care physician, he was diagnosed with anemia which was attributed to the epistaxis. After being evaluated by an ear, nose, and throat (ENT) specialist for treatment of the epistaxis, anemia continued. Eventually, he was diagnosed with celiac disease. Implications for health coaching are explored.
Keywords
L.Y., a 52-year-old male, was experiencing episodic epistaxis and periods of not feeling well at work. The frequency of epistaxis, weakness, and lightheadedness was alarming to his manager. L.Y. was sent to the occupational and environmental health nurse for evaluation. A comprehensive health history revealed seven episodes of epistaxis while at work over the past month. In this evaluation, he commented that seasonal allergies caused him sinus problems including nosebleeds. He could not recall the number of nosebleeds at home as it was too many to remember. He stated he had at least one minor nosebleed per week. He also stated he did not feel well and did not understand his lack of energy. Other health history data revealed hypertension, hypercholesterolemia, gout, prostate enlargement, and seasonal allergies. L.Y. provided documents from his last physician appointment. Notes on the blood work from his primary care physician (PCP) instructed him to take iron tablets for anemia. He had not yet purchased iron tablets.
Motivational interviewing was implemented to engage L.Y. in health coaching. He asked for information on anemia and iron tablets. Permission was granted to inquire about his medications (Table 1) and to provide evidence-based health information on anemia and iron tablets. Goals were mutually established, and L.Y. agreed to talk with his PCP before the next health coaching appointment in 2 weeks.
Daily Medications
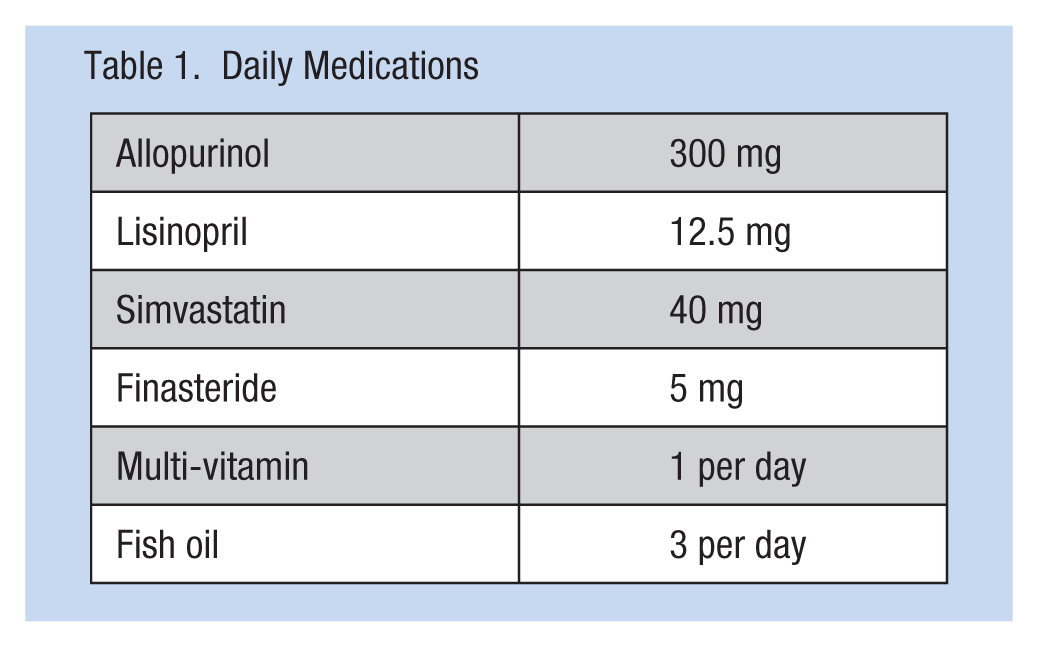
L.Y. is a 5 feet 8 inch male weighing 211 pounds. His vital signs were as follows: temperature 97.9 F, heart rate 88 beats per minute, respiratory rate 10 per minute, and blood pressure 140/80.
One week later, L.Y. met with his PCP and was given a referral to seek further evaluation by an ENT specialist. While waiting for the ENT appointment, L.Y. had three more episodes of epistaxis at work. The ENT evaluated L.Y. and scheduled him for sinus surgery. The surgical treatment was successful as he had no further epistaxis while at work or home.
Three weeks later, L.Y. returned to the clinic with a complaint of a painful left great toe. He reported that he was out of his gout medication. Through health coaching, a new plan was established, and L.Y. called his PCP’s office for a medication refill. The prescription was renewed over the phone. He was prescribed Indomethacin 50 mg three times a day as needed during episodes of gout.
One week later, L.Y. returned to his PCP for quarterly blood work and renewal of his antihypertensive medications. Soon after, L.Y. was accompanied to the occupational health (OH) clinic by his manager because he was emotionally upset. Health coaching techniques were used to understand the situation; L.Y. told the occupational and environmental health nurse he was convinced he had colon cancer. Motivational interviewing techniques were used to help L.Y. gain emotional control and establish an action plan.
L.Y. was referred to a gastrointestinal specialist for an esophagogastroduodenoscopy (ESG) and colonoscopy. After both diagnostics were completed, he was informed he might have celiac disease. The ESG revealed L.Y. had gastritis, esophagitis, and duodenitis. A biopsy of the duodenal tissue revealed irregular mucosa with lymphocytic infiltration.
The microscopic duodenum tissue biopsy showed atrophy and flattening abnormalities of the villous, elongation of the crypt and chronic inflammation of the tissue (Figure 1).
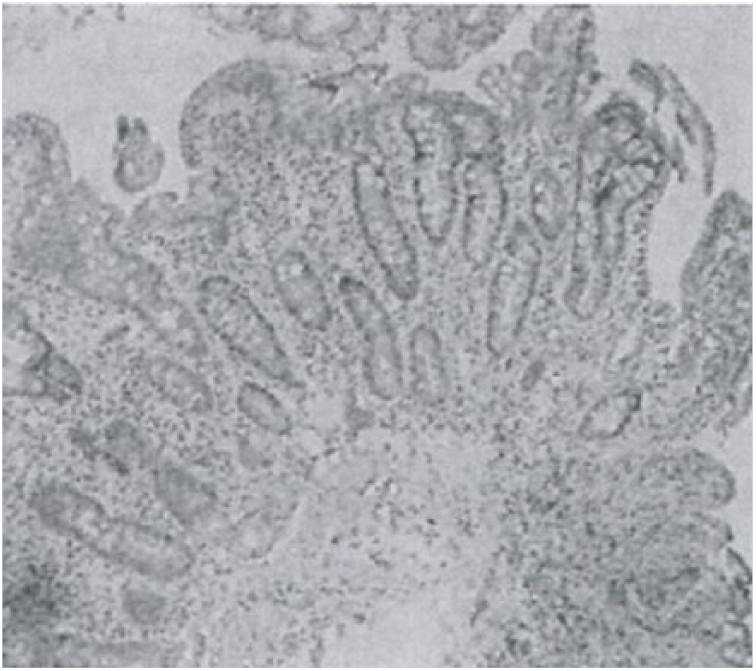
Duodenum tissue biopsy.
The physician’s operative report noted L.Y. should have a celiac panel and, if confirmation testing was positive for antibody against gluten, begin a gluten-free diet. The colonoscopy revealed several benign polyps, which were removed successfully.
The comprehensive panel for confirming celiac disease was positive (Table 2). L.Y.’s. physician ordered a gluten-free diet. He had no family history of celiac disease although his siblings had a plethora of other autoimmune disorders.
Celiac Disease Comprehensive Panel Results Confirming Celiac Disease
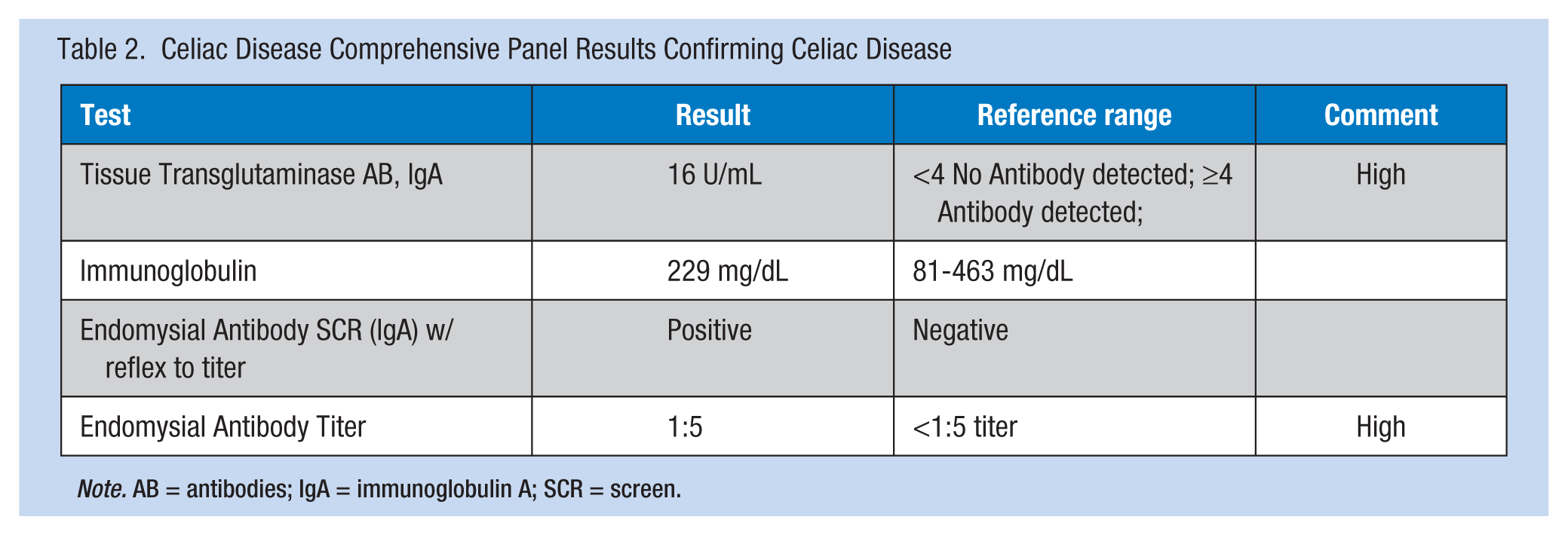
Note. AB = antibodies; IgA = immunoglobulin A; SCR = screen.
L.Y. returned to the OH clinic asking for information about gluten-free diets. Motivational interviewing was used by the nurse to provide information on gluten-free diets and reliable websites for gluten-free information. L.Y. and his wife followed the plan from the health coaching session to make dietary changes. A tour of the workplace cafeteria and vending machines demonstrated to L.Y. he could eat a gluten-free diet while at work.
After 4 months of dietary change, L.Y. returned to his physician for additional laboratory screenings to monitor his celiac disease. Results of the blood test for tissue transglutaminase antibodies, immunoglobulin A were negative.
Celiac Disease
Celiac disease is an autoimmune disorder affecting 1% to 3% of the global population and is a global health concern requiring a multidisciplinary approach for care and treatment (Husby et al., 2012; Rubio-Tapia & Murray, 2010).Celiac disease can occur at almost any age with cases ranging from childhood to adulthood. The development of this disease can be linked to consumption of gluten proteins and a genetic predisposition; most patients will have the human leukocyte antigen (HLA), HLA-DQ2 or HLA-DQ8 (Presutti, Cangemi, Cassidy, & Hill, 2007), and atrophy of the intestinal villous (Green & Jabri, 2003). This disease is known to cause inflammation of the mucosa in the small intestine; however, it can also affect the skin, joints, uterus, brain, heart, and other organs (Martin, 2007). Individuals at increased risk for celiac disease are those with another autoimmune disorder, type 1 diabetes mellitus, Turner syndrome, or Down’s syndrome (Ryan & Grossman, 2011).
Randolph (2012) stated gluten is found in a number of foods such as Kamut®, rye, spelt, barley, wheat, wheat-related grains, sauces, soups, candies, marinades, and processed meats. These foods are contraindicated for a gluten-free diet. The National Digestive Diseases Information Clearinghouse (2012) identified other products with gluten including envelopes, stamps, lip balm, and medications.
Treatment is based on elimination of gluten from the diet. Some food labels are easy to read and understand, but other food labels may provide variations on gluten product ingredients with which the worker will need to become familiar. Mobile applications can identify acceptable products for a gluten-free diet when grocery shopping or eating in a restaurant. Thompson (2006) stated variations on gluten-containing products include semolina, self-rising flour, white flour, and enriched flour. Barley-containing products include those with malt, including some beers.
Implications for Practice
As this case shows, some employees contact the occupational and environmental health nurse for health coaching, health education, and emotional support. The occupational and environmental health nurse can support workers who may have celiac disease by providing health education and raising awareness (Randolph, 2012). The nurse is in a unique position to use health coaching to help workers adopt lifestyle changes that affect their overall health by guiding the conversation and assisting workers in setting their agendas and goals.
Health education can be incorporated in a health coaching session after gaining permission from the employee. Once permission is granted, the occupational and environmental health nurse should provide evidence-based health education on gluten-free foods, how to identify foods that can be safely consumed and foods to avoid, planning foods for travel, and locating gluten-free restaurants. Reliable resources can be found in Table 3. Part of health coaching is to gain commitment from workers to accomplish goals, praising workers for reaching goals, and providing feedback and exploring ambivalence when no progress is achieved. The goal of health coaching is to assist workers in reaching established health goals.
Reliable Resources
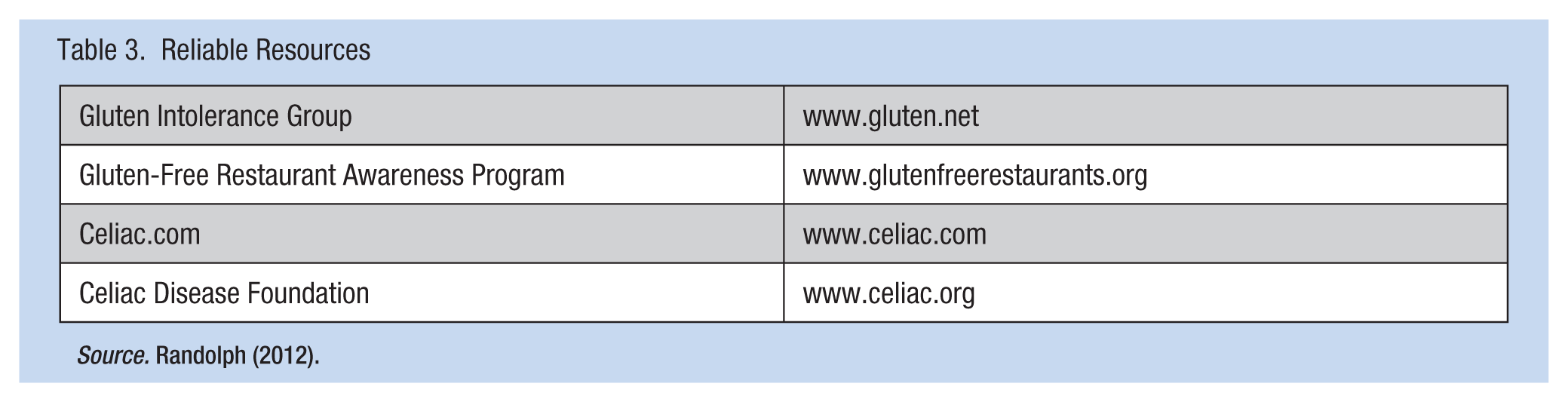
Source. Randolph (2012).
Conclusion
L.Y. is among a growing number of workers diagnosed with celiac disease. The occupational and environmental health nurse can support workers by using health coaching to assist workers to adopt a gluten-free diet, evaluate restaurant menus, eat a healthy diet while traveling, and manage a gluten-free diet by using mobile applications (Table 4). L.Y. became vigilant about his diet. His family purged food products from the home pantry, refrigerator, and freezer. With support from the occupational and environmental health nurse, L.Y. took charge of his health and set goals to alleviate his symptoms. Anemia resolved and L.Y.’s physical health status improved. After 6 weeks on a gluten-free diet, L.Y.’s celiac disease comprehensive panel returned to normal.
Mobile Application
Note. GF = gluten free.
Footnotes
Acknowledgements
The author wishes to thank Irene M. Cheung MSN, RN, for her assistance in proofreading and editing.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Letha Smith, MS, RN, COHN-S, FAAOHN, is an occupational health nurse in Irving, Texas and is a member of the North Texas Association of Occupational Health Nurses.