
Abstract
The AAOHN Competency document is one of the core documents that define occupational health nursing practice. This article provides a description of the process used to update the competencies, as well as a description of the new competencies.
Keywords
Competencies for Occupational and Environmental Health Registered Nurses (RN)
Occupational and environmental health nursing is a subspecialty of public/community health nursing, with unique knowledge and skill sets not found in other nursing specialties. The American Association of Occupational Health Nurses, Inc. (AAOHN) has developed several documents (i.e., The Code of Ethics and Interpretive Statements, Standards of Occupational and Environmental Health Nursing, Competencies in Occupational and Environmental Health Nursing, and The Fundamentals of Occupational and Environmental Health Nursing, AAOHN Core Curriculum 4th Edition) that serve as the framework for the specialty practice of occupational and environmental health nursing. Together, these documents:
define the scope of occupational and environmental health nursing;
provide an ethical framework for occupational and environmental health nursing practice;
delineate principles supporting essential practice knowledge;
describe the abilities required for competent practice; and
provide a comprehensive resource for occupational and environmental health nurses.
All practicing occupational and environmental health nurses must adhere to various standards, regulations, and guidelines that apply to delivery of nursing care in their practice settings. The AAOHN foundational documents are an invaluable source of information for all occupational and environmental health nurses to assure delivery of competent, ethical, and legal nursing care.
It is incumbent upon the profession to maintain the documents describing the competencies required for occupational and environmental health nurses. AAOHN first established competencies for occupational and environmental health nurses in 1999, detailed by nine categories and three competency levels (AAOHN, 1999). The competencies were revised in 2003 and 2007, still retaining the nine categories and the levels of competent, proficient, and expert. Each revision attempted to simplify the language; shorten, streamline and reduce duplication in the competencies to clarify them for the profession, individual nurses and employers; and provide a baseline for certification support, performance evaluations, and developmental plans (AAOHN, 2003; AAOHN, 2007).
Since the last update of the AAOHN competencies was published, occupational and environmental health nursing has evolved, necessitating an in-depth review of existing competencies. New terminology and scientific evidence have expanded the knowledge base for practice. The United States (U.S.) healthcare system has changed dramatically. Numerous occupational and environmental health nurses have assumed global responsibilities for the health and safety of workers outside the US, and many workforces include expatriates and frequent international visitors and workers. Likewise, the specialty now includes more advanced practice nurses than was the case in 2007, and AAOHN expanded membership to include Licensed Practical/Vocational Nurses (LPN/LVN) in 2011. In 2014, the AAOHN Board of Directors created a Task Force of experts with diverse occupational and environmental health nursing backgrounds to revise and update the Competencies for Occupational and Environmental Health Nursing.
Competencies reflect the proficiencies required to perform a particular task or play a defined role (Oerman & Gaberson, 2013). Competencies are guidelines applicable to occupational and environmental health nurses who assume a variety of practice roles; competencies address the continuum of practice experiences. AAOHN (1999) defines competencies as outcome-oriented statements that describe the mastery of a particular skill or ability. To maintain competence, each health care professional is expected to manage an evolving scope of practice. Competencies do not address educational preparation or licensure. In addition to registered nurses (RNs) working in occupational health, LPN/LVNs may provide supportive, technical services in an occupational setting; but they must always work under supervision of (registered) nursing or medical personnel (AAOHN Position Statement, 2012). All nurses can enroll in continuing education courses offered by AAOHN and other organizations to learn the basics of occupational health nursing, and develop specific knowledge and skills to deliver occupational programs and services, such as spirometry and audiometry screenings. AAOHN specifically encourages LPNs/LVNs and non-BSN-prepared RNs to complete university degrees. Since LPNs/LVNs must have technical tasks delegated to them by RNs or medical personnel, these revised competencies are specifically written for registered professional nurses who work in occupational and environmental health.
Methods
To establish content validity (Grant & Davis, 1997), the Task Force included AAOHN members who practice across multiple geographic locations and represent single and multi-nurse units and hospitals/healthcare, manufacturing, education, global and military sectors. They practice clinically as BSNs and nurse practitioners, risk management/safety/environmental professionals, case managers, health promotion/wellness/chronic disease managers, consultants, and researchers.
Four members of the Task Force and the chair were doctorally-prepared clinicians, academicians, or researchers. Five more members were master’s-prepared clinicians with significant experience in their practices. Three were BSN-prepared and one had a diploma in nursing. Ten members were certified occupational health nurses (COHN or COHN-S). Every member had published in a peer-reviewed occupational health nursing journal or book. Several members had presented continuing education seminars and others had taught academic courses in occupational health nursing. Several Task Force members had served in elected positions in AAOHN at the national and/or state level. All members of the team contributed individually to the development, revision, and approval of the final version of the competencies document.
During eight telephone and one face-to-face meeting held over 15 months during 2014 and 2015, the Task Force extensively reviewed the literature, specifically documents containing the competencies of other professions (ACHE, 2012; ACOEM, 2014; Council on Linkages Between Academia and Public Health Practice, 2010; Fouad et al, 2009; Interprofessional Education Collaborative Expert Panel, 2011) and drew upon their own expertise to provide a framework for the revised document. The Task Force agreed that more emphasis should be placed on wellness and health promotion, evidence-based practice, and caring for the working populations and communities that occupational and environmental health nurses serve. The Task Force drafted a document containing four categories under which 22 competencies were organized (Table). The Task Force used a two-round modified Delphi process to validate their work (Lee, Johnson, Newhouse & Warren, 2013).
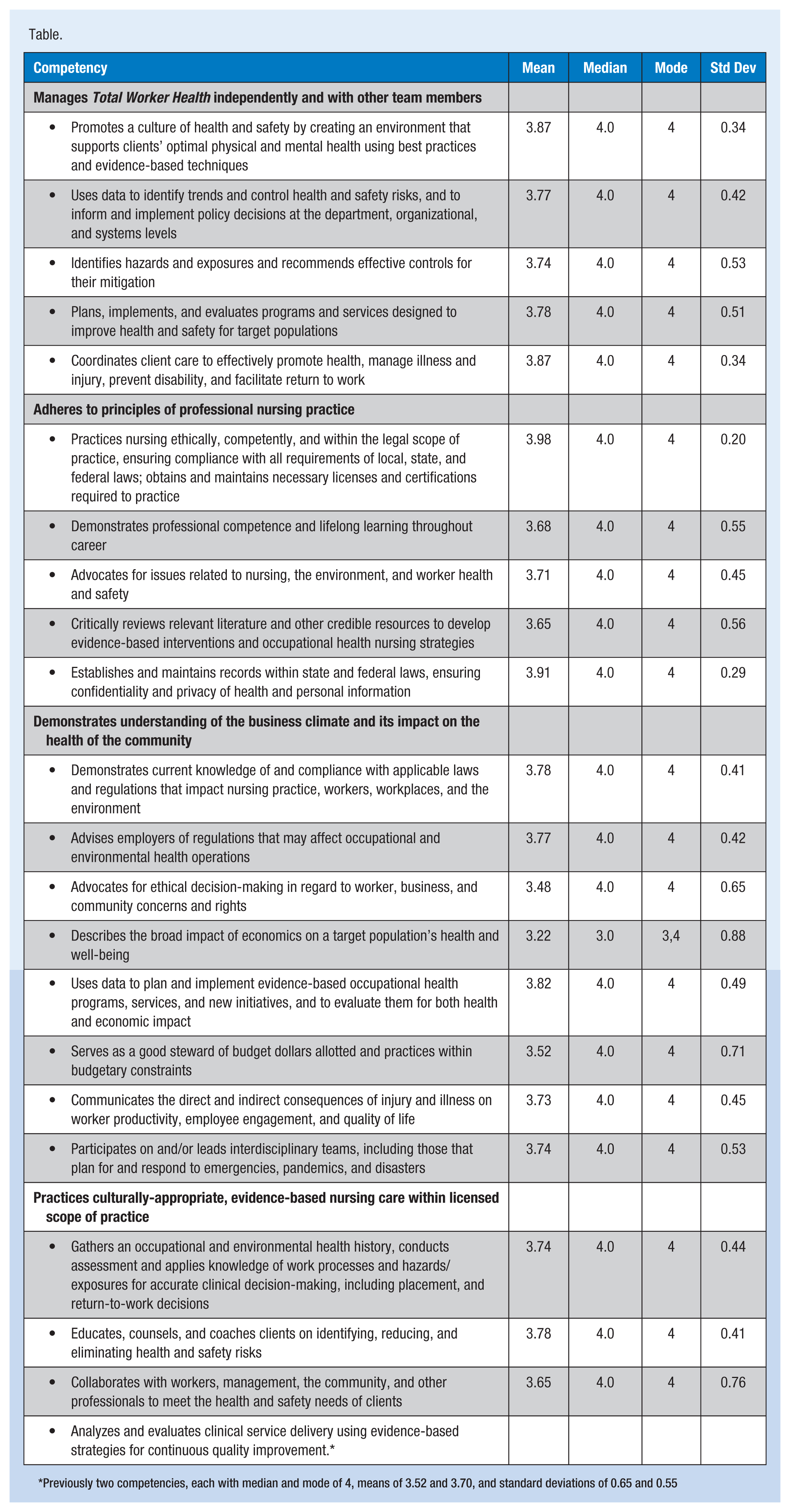
Previously two competencies, each with median and mode of 4, means of 3.52 and 3.70, and standard deviations of 0.65 and 0.55
The Delphi method is widely used to build consensus on a topic. Its advantages are anonymity and the avoidance of bias due to the influence of a single individual (Huss & Shadford, 2007). The Task Force identified a second panel of thirty geographically-dispersed occupational and environmental health nurse experts representing diverse industries, universities providing occupational and environmental health nursing continuing education and advanced degrees, managers of occupational health programs, RNs and occupational health nurse practitioners, to participate as competency reviewers. Two iterations were reviewed to achieve consensus by the review panel (Polit & Beck, 2008).
The thirty occupational and environmental health nurse expert reviewers were contacted via email and asked to complete an on-line survey. For each competency, reviewers were asked to rate the competency’s relevance on a 4-point Likert scale: Not relevant, Somewhat Relevant, Quite Relevant, or Highly Relevant. The second question for each competency asked whether the item was well-written and distinct (yes/no). Each competency included a comment box as well as an opportunity to provide general comments at the end of the survey. Reviewers were asked to complete the survey within two weeks, at which time the survey was closed and results were analyzed.
Prior to sending the survey for the first round of the Delphi process, the Task Force agreed that to be included in the final document, a competency had to have a median score of at least 3.25, with 70% of the responding experts scoring the competency as Quite Relevant or Highly Relevant (3 or 4).
For the first round, only 13 experts (43%) completed the survey. Based on the feedback received from those experts, the Task Force revised the competencies. These revisions were included in the survey for the second round. Prior to the second modified-Delphi round, the 30 experts were contacted via email to alert them of the survey that would be arriving shortly. The link to the survey was then sent via email from AAOHN staff, rather than an automated Survey Monkey email. Expert panelists were given two weeks to complete the survey. A reminder email was sent in the middle of the second week to all participants, encouraging them to complete the survey if they had not already done so.
Task Force members who attended the Committees Meeting at the 2015 AAOHN Conference in Boston in March, discussed the results and the feedback received. Changes were made to some competencies based on feedback from the Delphi panelists. One competency did not achieve the a-priori requirement of a median score of at least 3.25, so Task Force members were surveyed to determine whether the competency should be included as written.
Results
For the second round, 23 experts (77%) completed the survey. Nearly all competencies met the a-priori standards of a median score of at least 3.25 with 70% of the responding experts scoring the competency as Quite Relevant or Highly Relevant (3 or 4) (Table). Many comments were submitted, and explanations in this article address the concerns voiced by the experts. The resulting 22 competencies divided among four categories are discussed here.
Manages Total Worker Health Independently and With Other Team Members
Adheres to Principles of Professional Nursing Practice
Demonstrates Understanding of the Business Climate and Its Impact on the Health of the Community
Practices Culturally-Appropriate, Evidence-Based Nursing Care within Licensed Scope of Practice
Discussion
Fifteen experts (65%) included general comments about the competencies. Several comments indicated satisfaction with the broad approach to these competencies. One respondent felt that primary care was not sufficiently addressed in these competencies, despite the fact that on-site primary care is becoming more common. Another expert noted that the focus on economics and cost could be reduced in favor of more emphasis on prevention.
One reviewer suggested the competencies may not be met by occupational and environmental health nurses with less than a master’s degree, and another was concerned that the competencies reflect the subspecialty and not just nursing in general (“…so that not any RN can come in and practice in our specialty…”). Although no specific reference is made to OSHA, ADA, FMLA, or other legislation, the competency of adherence to regulations essentially eliminates from practice those nurses who do not have that knowledge base. Occupational and environmental health nurses can demonstrate their competency via certification as a Certified Occupational Health Nurse (COHN) or Certified Occupational Health Nurse Specialist (COHN-S). The path to certification in occupational and environmental health nursing is through the American Board of Occupational Health Nurses, Inc. (ABOHN), an independent nursing specialty certification board. ABOHN’s certification examinations are based on AAOHN’s Competencies for Occupational and Environmental Health Nursing. Qualification for the examination does not require master’s preparation. However, becoming a COHN or a COHN-S requires that nurses sitting for the examination have education and experience related to each of the Occupational and Environmental Health Nursing Competencies to establish a foundation for occupational and environmental health nurses to improve their practices throughout their careers.
The majority of experts who participated in the modified Delphi process of validating these competencies agreed that they are appropriate and comprehensive, though 100% agreement on every competency was not achieved. AAOHN revises competencies as necessary, and these competencies will likely be modified in years to come. AAOHN is grateful to the members who participated on the Task Force, as well as those who critically reviewed the competencies during the modified Delphi process.
Footnotes
Task Force
Eileen Lukes, PhD, RN, COHN-S, CCM, FAAOHN, Chair; Kathryn Duffy, MS, ANP-C, COHN-S; Cindy Groves, BSN, RN, COHN-S; Pam Hart, MPH, RN, COHN-S, CSP; Ann Lachat, RN, BSN, FAAOHN, COHN-S/CM; Yolanda Lang, PhD, MSN, CRNP, COHN, FAAOHN; Sheila Litchfield, BSN, RN, FAAOHN, COHN-S (Retired); Linda McCauley, PhD, RN, FAAN, FAAOHN; Susan Randolph, MSN, RN, COHN-S, FAAOHN; Mary Gene Ryan, MPH, BSN, COHN-S/SM, CSP, FAAOHN; Pat Strasser, PhD, RN, COHN-S/CM, FAAOHN; Joy Wachs, PhD, RN, FAAOHN; Tammy Watts, MS, RN, OHNP-BC; Chris Zichello, RN, COHN-S, CSHM, ARM, CSPHP, FAAOHN
Reviewers
Phyllis A. Berryman, MBA, RN, COHN-S/CM, FAAOHN; Pat Bertsche, PhD, MPH, RN, COHN-S, FAAOHN; Barbara Burgel PhD, RN, FAAN, COHN-S, FAAOHN; Candace Burns, PhD, ARNP; Francis Childre, MS, RN, COHN-S, FAAOHN; Jane Christianson, PhD, RN; Butch de Castro PhD, MSN/MPH, RN; Deb Fell-Carson, MSPH, RN, COHN-S, FAAOHN; Kimberly Gordon, MSN, MA, BSN, RN, COHN-S, FAAOHN; Karen Griffith, MBA, BSN, RN, COHN-S; Annette Haag, MA, RN, COHN-S/CM, FAAOHN; Oisaeng Hong, PhD, RN, FAAN; Nadine Jones, MPH, RN, COHN-S/CM; Sharon Kemerer, MSN, RN, COHN-S/CM; Diane Layne, MPH, RN, COHN-S/CM; Peggy Manuszak, MS, RN, COHN-S/CM, FAAOHN; Karen Mastroianni, EdD, MPH, BSN, RN, COHN-S; Marjorie McCullough, PhD, RN; Pat McGovern, PhD, MPH, RN; Pam Moore, EdD, MPH, RN, FAAOHN; Kimberly Olszewski, DNP, RN, CRNP, COHN-S/CM, FAAOHN; Lizbeth J. Proffitt, MSN, COHN-S/CM; Lisa Pompeii, PhD, RN, COHN-S, FAAOHN; Deborah Reed, PhD, MSPH, RN; Wendie Robbins, PhD, FAAN; Deb Roy, RN, COHN-S, CET, CSP, FAAOHN; Jeanne Tomlinson, MSN, RN, COHN-S, FAAOHN; Mary Lou Wassel, MEd, RN, COHN-S/CM, CSP, FAAOHN; Helen Williams, MSN, APN-BC, GNP-BC, COHN-S, CCM; Kathy Zorb, MPH, RN, COHN-S/CM
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.