
Abstract
This article provides an update of the current status of cardiovascular disease (CVD) in the United States, including a brief review of the underlying pathophysiology and epidemiology. This article presents a discussion of the latest American Heart Association guidelines that introduce the concept of promoting ideal cardiovascular health, defined by seven identified metrics. Specific CVD risk factors and utilization of the 10-year CVD event prediction calculator are discussed. In addition, current management recommendations of health-related conditions that increase risk for CVD, such as hypertension and hypercholesterolemia, are provided. Finally, a discussion of detailed evidence-based lifestyle recommendations to promote cardiovascular health and reduce CVD risks concludes the update.
Cardiovascular disease (CVD) is the number one cause of death in the United States and globally, affecting both men and women. The World Health Organization (WHO) estimates that CVD claimed 17 million lives worldwide in 2012, and this number is predicted to double in the next 15 years (WHO, 2015). One of three deaths in the United States is attributable to CVD (Mozaffarian et al., 2015a). To begin addressing this universal problem, the WHO created an Atlas of Heart Disease and Stroke aimed at reducing CVD risks by educating policy makers, organizations, and health professionals who can affect population health (WHO, 2015). In an effort to reduce morbidity and mortality related to CVD, the American Heart Association (AHA) developed an online resource center to promote workplace health (AHA, 2015). Although there are many types of heart and artery diseases (including valvular heart disease, heart failure, arrhythmias, peripheral arterial disease, and aneurysms), the emphasis of the WHO and AHA health promotion efforts and the focus of this update article are atherosclerotic heart disease and stroke.
Pathophysiology and Epidemiology
Atherosclerosis
Atherosclerosis is a complex disease that limits perfusion throughout the body and can significantly affect vital organs. Inflammation is the underlying trigger that initiates the atherosclerotic process, perpetuates plaque development, and stimulates continued accumulation of plaque components that can eventually form a thrombus (Brashers, 2015). The outcome of untreated atherosclerosis is decreased blood flow in the micro and macro vascular systems. Atherosclerosis in the heart or brain significantly increases the risk of myocardial infarction or stroke.
Heart Disease
One of the interesting findings in heart statistics is that over the past decade, the death rate from heart disease fell by 39% in the United States (Mozaffarian et al., 2015b). During the same time period, procedures and surgeries for heart disease increased by 28% due to the development of new treatments that have improved outcomes (Mozaffarian et al., 2015b). Despite this small bit of good news, the pervasiveness of atherosclerotic heart disease continues to be of great concern and remains the leading cause of death among both men and women, accounting for one of seven deaths in the United States (Mozaffarian et al., 2015b). More women than men die from heart disease today, and the number of deaths in women aged 35 to 44 years has increased over the past 5 years (Gulati, Shaw, & Bairey Merz, 2012; Mosca et al., 2011; Roger et al., 2011).
Stroke
Deaths from strokes declined by 21% between 2001 and 2011; new medications and procedures might have also improved this trend (Mozaffarian et al., 2015a, 2015b). Yet, stroke is the fourth leading cause of death and is currently the number one cause of disability in the United States (Mozaffarian et al., 2015b). African Americans are twice as likely to suffer a stroke compared with their White counterparts (Lehmkuhl et al., 2012; Malarkey, Jarjoura, & Klatt, 2013; Mozaffarian et al., 2015b).
Clearly, the most current heart disease and stroke statistics paint a picture of the far-reaching impact of CVD in the United States. Both men and women from all ethnic groups are at risk for developing atherosclerosis and suffering a subsequent CVD event. In an effort to use the current data on the risks for heart disease and stroke, several professional organizations collaborated over the last year to initiate a new approach to addressing the issue of CVD through education and prevention.
New Approach to CVD and Cardiovascular Health
Rather than simply focusing on the perpetual problem of CVD, the new approach emphasizes promoting “Ideal Cardiovascular Health” (Eckel et al., 2014). CVD may affect individuals’ abilities to enjoy a productive job or fulfilling hobbies and can elicit worry or cause a burden for family members who have to undertake additional duties. Individuals, families, and businesses may feel an economic strain related to CVD. Consequently, the new guidelines endeavor to refocus from the aftermath of CVD to prevention of CVD through health promotion. The AHA, along with the American College of Cardiology (ACC) and the National Heart Blood and Lung Institute, developed evidence-based lifestyle management guidelines to prevent CVD and promote cardiovascular health (Eckel et al., 2014). “Current evidence supports a range of complementary strategies to improve cardiovascular health” (Mozaffarian et al., 2015a, p. 435).
Ideal Cardiovascular Health
The new AHA guidelines promote the concept of ideal cardiovascular health, characterized by specific behaviors and physiological measurements determined by a scientific review of the published literature (Eckel et al., 2014; Goff et al., 2014; Mozaffarian et al., 2015a). The seven delineated health metrics for ideal cardiovascular health are not smoking, engaging in sufficient physical activity, eating a healthy diet, and maintaining a normal body weight, optimal total cholesterol level, normal blood pressure, and normal fasting blood glucose in the absence of drug treatment (Table 1; Mozaffarian et al., 2015a). The aim of this new focus is to generate ideas and implement strategies and incentives across health care systems, in communities, schools, businesses, and at home that can contribute to the promotion of cardiovascular health (Mozaffarian et al., 2015a).
Delineated Health Metrics for Ideal Cardiovascular Health
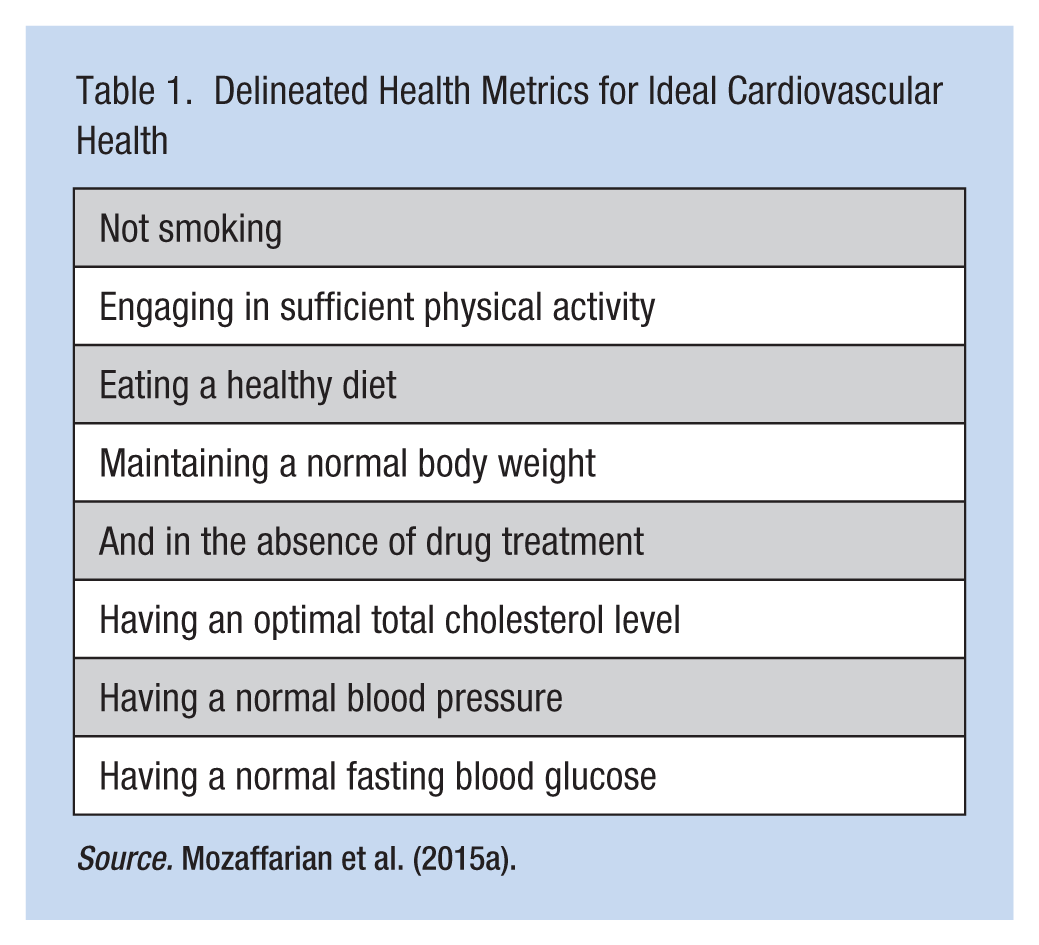
Source. Mozaffarian et al. (2015a).
CVD Risk Factors
According to the statistical update by the AHA, American’s overall cardiovascular health status is poor (Mozaffarian et al., 2015b). Identifying CVD risks is an imperative first step toward improving cardiovascular health because the information from risk assessments can guide the development of a risk reduction plan. Evidence supports evaluation of the following CVD risks that are in opposition to ideal health metrics: smoking, lack of physical activity, unhealthy diet, overweight or obesity, hyperlipidemia, hypertension, diabetes mellitus, and family history of CVD (Goff et al., 2014; Mozaffarian et al., 2015a). Experts note that when designing risk reduction plans, consideration of additional unique CVD risk factors such as C-reactive protein, coronary calcium score, and ankle brachial index may be beneficial (Goff et al., 2014).
Clearly, assessment and treatment of CVD risks are vital because atherosclerosis develops over decades. Reducing the cumulative exposure to the effects of any modifiable CVD risks is crucial. Understanding the current status of population CVD risks can provide a foundation for risk appraisal and is the purpose of the 2015 Heart Disease and Stroke Statistics Update, which compiled the following data (Mozaffarian et al., 2015a).
Approximately 30% of deaths in the United States from heart disease are attributable to smoking and exposure to secondhand smoke. Currently, 20% of men and 16% of women in the United States smoke cigarettes. The economic burden associated with the health care costs and lost productivity from the effects of smoking is greater than US$289 billion.
Only half of adults meet the recommended aerobic physical activity guidelines; one of three does not participate in any physical activity.
Less than 1% of Americans more than 21 years old meet the AHA definition of a healthy diet, and 69% of adults are overweight or obese.
Forty-three percent of Americans have a total cholesterol level over 200 mg/dL, and one of three has an elevated low-density lipoprotein (LDL) level.
80 million Americans have hypertension, and only 54% of these individuals have their blood pressure adequately controlled through treatment.
Type 2 diabetes mellitus affects 1 of 10 adults in the United States, and this prevalence is expected to increase.
A positive family history of CVD in a first-degree relative increases the likelihood of having heart disease or a stroke by 45% to 50%. Clustering of both environmental lifestyle factors and genetic influences contribute to CVD family history.
C-reactive protein levels, coronary calcium score, and ankle brachial index have all been shown to be associated with increased incidence of CVD events and may inform CVD risk reduction treatment decisions.
CVD Risk Assessment Calculator
The latest AHA guidelines recommend assessing traditional CVD risk factors every 4 to 6 years in 20- to 49-year-old adults who have no known CVD (Goff et al., 2014). In adults aged 40 to 79 years without known CVD, the assessment should also include an estimation of 10-year risk of first atherosclerotic cardiovascular event, defined as a myocardial infarction or stroke, using an evidence-based prediction calculator every 4 to 6 years (Goff et al., 2014). The CVD risk calculator application is available on the web and for handheld devices at the following sites:
Specific information that must be entered into the risk calculation includes gender, age, total cholesterol, high-density lipoprotein, and systolic blood pressure, whether taking medication for hypertension, a diabetes diagnosis, and personal smoking history (Goff et al., 2014). The calculator then produces a risk percentage as a prediction suffering an atherosclerotic cardiovascular event within the next 10 years. CVD treatment decisions can then be based on this risk percentage.
Promotion of Cardiovascular Health
As previously noted, the assessment and treatment of identified CVD risks are imperative to promote ideal cardiovascular health. Occupational health nurses can focus on some of these CVD risk factors while working with their clients by measuring blood pressure, cholesterol, and blood sugar, as well as providing instruction about lifestyle choices. Being aware of the most recently published guidelines for each of these CVD risk factors can provide a foundation for nurses to advocate for wellness programs and provide personal health education in the workplace. Current evidence-based diagnosis and management recommendations for hypertension, hypercholesterolemia, diabetes, and related CVD lifestyle choices are noted below.
Blood Pressure
During 2014, updated hypertension management guidelines were released that defined new target blood pressure levels for adults based on age and health-related conditions. Individuals under age 60 years, as well as those with diabetes or chronic kidney disease, should aim for a blood pressure of 140/90 or lower (Page, 2014). The target level for those 60 to 79 years of age without defined health-related conditions is now 150/90 (Page, 2014). Many people in the United States have undiagnosed or undertreated hypertension that contributes to increasing CVD risk over time (Wall, Hannan, & Wright, 2014).
Cholesterol
In 2013, new cholesterol guidelines to reduce atherosclerotic cardiovascular risk in adults were published based on fasting LDL level, presence of disease, and use of the 10-year CVD risk calculator described earlier in this article (Stone et al., 2014). The evidence-based recommendations indicated that statin therapy is likely to benefit four defined groups: those with existent clinical CVD, with an LDL equal to or greater than 190mg/dL, with a 10-year estimated CVD risk of 7.5% or greater, and over age 50 years with a diagnosis of diabetes (Stone et al., 2014). Statin medication to lower cholesterol should be considered for primary prevention of CVD and to reduce the risk of a CVD event in adults who fall into any of these categories.
Blood Glucose
Maintenance of a normal fasting blood sugar between 100 and 126 is also recommended as a metric of cardiovascular health. The most recent diabetes guidelines include information about pre-diabetes and obesity treatment recommendations (American Diabetes Association, 2014; Garber et al., 2013). Diabetes management details are beyond the scope of this article, but the lifestyle discussion below is applicable to preventing and controlling diabetes.
Lifestyle
Primary CVD prevention and risk reduction through a healthy lifestyle are the basis of the updated AHA and ACC guideline on lifestyle management and support the concept of ideal cardiovascular health (Eckel et al., 2014). General nutritional recommendations are to eat a diet that emphasizes fruits, vegetables, whole grains, low-fat dairy products, poultry, fish, legumes, and non-tropical oils and nuts, while limiting red meat, sweets, and sugar-sweetened beverages (Eckel et al., 2014). Specific dietary advice is provided to address CVD risks based on evidence in the literature. Examples include reducing saturated fat intake to 5% to 6%, limiting calories from trans-fat to aid in lowering LDL cholesterol, and decreasing sodium intake to between 1500mg and 2000mg a day to lower blood pressure (Eckel et al., 2014). In addition to healthy eating, all individuals should engage in aerobic physical activity for a minimum of three to four times a week for 40 minutes to promote ideal cardiovascular health.
Finally, stress reduction activities are another important aspect of a healthy lifestyle that nurses can encourage. Research shows that negative psychological stress produces a variety of physiologic changes that lead to inflammation, the underlying trigger for atherosclerosis, and other chronic diseases (Forshee, Clayton, & McCance, 2010; Ippoliti, Canitano, & Businaro, 2013; Iwata, Ota, & Duman, 2013). Many therapies and activities have been shown to reduce stress, including exercise, yoga, music therapy, progressive relaxation, and mindfulness (Khoury et al., 2013). One study found that participation in 6 to 8 weeks of mindfulness practice at work resulted in significantly less perceived stress, less reported work burnout, and improved sleep and general health (Malarkey et al., 2013). Thus, occupational health nurses may be in an ideal setting to promote stress reduction and improve cardiovascular health.
Conclusion
Current evidence indicates that CVD remains the leading cause of death for both men and women. “Ideal cardiovascular health” is a new approach focusing on specific recommendations. The process of health promotion starts with the assessment and identification of CVD risk factors using evidence-based recommendations aimed at reducing risk and improving cardiovascular health. Occupational health nurses can use this information to communicate with organizations that promote wellness programs aimed at improving cardiovascular health for all.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Dr. Pearson is director of a family nurse practitioner program and has several decades of experience working with cardiovascular patients in a variety of clinical settings. She has completed multiple research studies focused on cardiovascular disease in women and has provided presentations on cardiovascular related topics to both professional and public audiences.