
Abstract
Lifting and holding patients’ limbs while preparing the skin for orthopedic surgeries may be a lengthy process causing work-related musculoskeletal disorders (MSDs) for preoperative team members. Studies reported weight limits for lifting and holding limbs; whenever this weight is greater than a specific amount, additional staff or assistive devices are needed because nurses and support staff working in orthopedic operating rooms (ORs) are at high risk of MSDs. The aim of this study was to demonstrate the design, construction, and effectiveness of a limb-lifting assistive device installed in the OR of 5 Azar Hospital affiliated with Golestan University of Medical Sciences and used during the surgical preparation process.
One of the major sources of surgical site infection (SSI) is microorganisms on the patient’s skin (Cheadle, 2006), and ineffective preoperative skin preparation is one of the risk factors for development of SSIs (Mangram, Horan, Pearson, Silver, & Jarvis, 1999). Thus, proper preparation of the surgical site by the operative team (i.e., nurses or technicians) can prevent SSIs (Owens & Stoessel, 2008).
During the preparation process before orthopedic surgeries, preoperative team members lift and hold patients’ limbs for up to 3 minutes using one or both hands. This manual process exerts strong forces on preoperative team members’ shoulder and back muscles and joints and may lead to work-related musculoskeletal disorders (MSDs; Waters et al., 2011). Neck and shoulder complaints are more prevalent among operating room (OR) nurses compared with other nurses (Bos, Krol, van der Star, & Groothoff, 2007). In research by Choobineh, Movahed, Tabatabaie, and Kumashiro (2010), OR nurses’ lower back pain was their most common symptom after manual material handling (MMH) activities, and nurses believed that musculoskeletal problems could lead to job change (Choobineh et al., 2010).
Maximum weights to be lifted and held for up to 2 minutes for a one-handed lift of particular parts of a patient’s body was assumed to be 5.03 kg and for a two-handed lift was assumed to be 10.1 kg. Whenever these weight limits are exceeded, additional staff or assistive devices are needed to minimize the risk of muscle fatigue and MSDs (Waters et al., 2011).
As nurses and other staff are at risk of developing work-related MSDs while lifting and holding limbs in orthopedic practice settings (Waters et al., 2009), use of an assistive device for lifting and holding a patient’s limb during the surgical preparation process could be beneficial for both the patient and preoperative team members. Thus, the aim of this study was to demonstrate the design, construction, and effectiveness of a limb-lifting assistive device installed in the OR of 5 Azar Hospital affiliated with Golestan University of Medical Sciences and used during the surgical preparation process.
Design and Construction
This limb-lifting assistive device was designed and constructed to lift and hold patients’ limbs during the prepping process for orthopedic surgeries. Before it was constructed, no standard devices were used for lifting and holding patients’ limbs during the preparation process. In the traditional standard manual process, one nurse lifted and held the patient’s limb for several minutes while another nurse prepared the skin for surgery, leading to increased risk for MSDs for the nurse lifting and holding the patient’s limb.
The limb-lifting/holding device was constructed with six parts: (1) motor and gearbox, (2) unit control, (3) wire rope, (4) pulley, (5) hook, and (6) fixer (Figures 1A and 1B). Motor, gearbox, and unit control were covered by a removable metal frame. The device has an 8-hour rechargeable battery and can be connected to a power source directly, as well. All components of this device, except the hook, can be sterilized simultaneously during sterilization of the OR. The hook, connected to the patient’s limb, is disposable; its minimum width and diameter are designed to prevent the patient’s limb from being compressed.
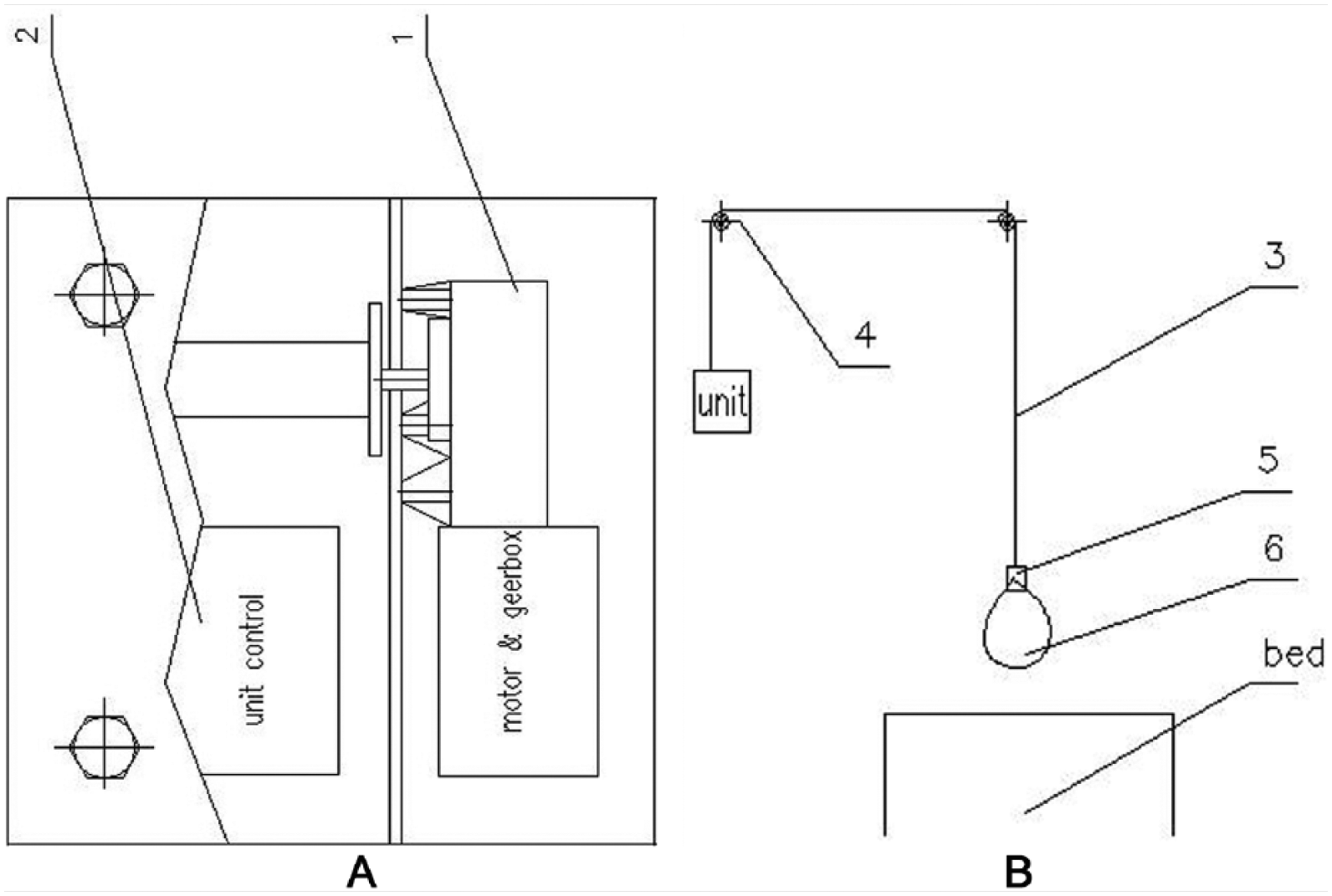
Plan of designed assistive device.
Trained staff and orthopedic surgeons can use this device during surgery and the prepping process. It is installed on the wall of the OR and the wire rope is driven by a pulley from above the patient’s bed. After the patient is anesthetized and positioned for limb prepping and surgery, the hook is connected to the limb. The device is turned on, and by pressing the up and down buttons of the remote control, appropriate height and angle of the limb can be set and modified during the preparation process and surgery. The process also protects the limb from damage to the surgical site or further injury (e.g., fracture). When the prepping process is completed, the patient’s limb is located in the sterile area to avoid contamination. Figure 2 shows the use of this device in the OR.
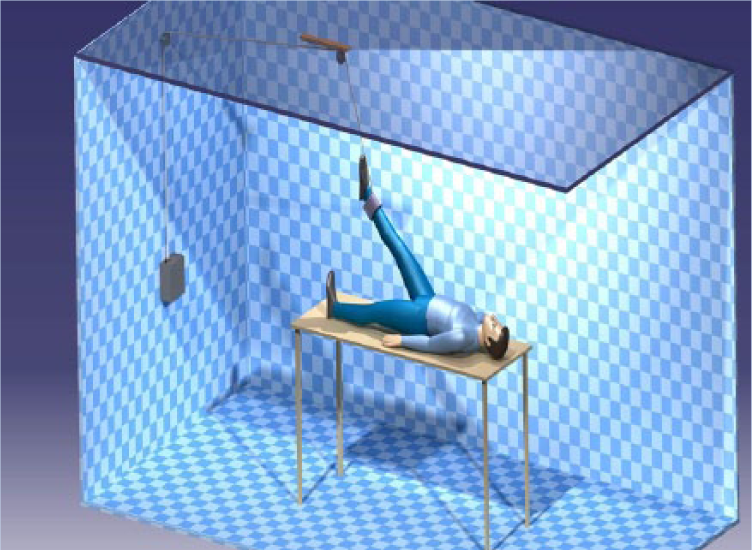
Schematic view of the designed assistive device.
Effectiveness Testing
To evaluate the efficacy of using the device during the surgical preparation process, a single blind randomized clinical trial was conducted with 48 patients who underwent orthopedic surgeries in 5 Azar Hospital affiliated with Golestan University of Medical Sciences in 2013. The study was reviewed and approved by the Golestan Research Ethics Committee.
In this study, the patients were randomly assigned to two groups. In the intervention group, patients’ limbs were held and lifted by the assistive device during the preparation process; for the control group, OR nurses lifted and held the limbs with one or two hands (traditional method). Study variables included gender of the OR nurses, duration of the preparation process, number of nurses involved in the preparation process, and OR nurses’ satisfaction.
SPSS Version 16 was used to analyze data. To test the association between categorical variables, chi square test was used or two-tailed Fisher exact test was used if the expected cell frequencies were too small. Independent-sample t test was used for continuous variables. A p value less than .05 was considered statistically significant. In both intervention and control groups, the majority of limbs lifted were feet (95.83% and 58.33%, respectively).
Table 1 shows demographic characteristics, frequency distribution, and mean of studied variables in the sample. No significant differences were found between the two groups in terms of gender ratios (p = .773). Use of the assistive device resulted in faster surgical preparation in the intervention group compared with the control group (p < .0001).
Demographic Characteristics of Population Studied, Frequency Distribution, and Mean of Studied Variables
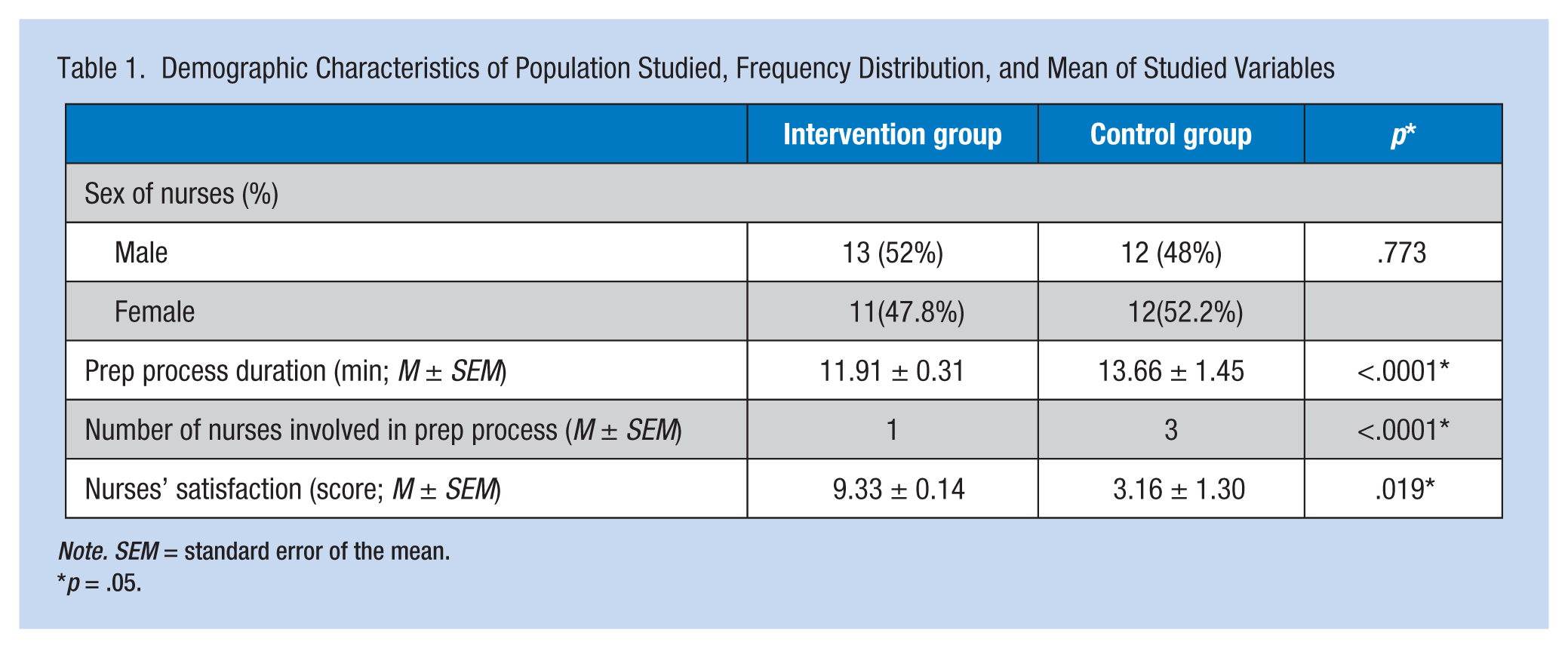
Note. SEM = standard error of the mean.
p = .05.
Furthermore, the number of nurses involved in the preparation process was reduced in the intervention group compared with the control group (p < .0001). In addition, satisfaction of nurses in both groups was measured by Visual Analogue Scale (VAS) with a range of 0 to 10, with 10 being the most satisfied. The mean satisfaction score was higher in the intervention group compared with the control group (p < .0001).
Implications for Occupational Health Nurses
Whereas occupational health nurses have a major role in the prevention of injuries to hospital staff, they should investigate the feasibility of implementing limb-lifting devices such as the one described in this study if traditional, manual processes are currently used. Return on the financial investment can be realized quickly when fewer injuries occur and fewer staff are needed. Employee health nurses should consider measuring adverse patient incidents using manual and mechanized surgical prepping in institutions that adopt limb-lifting devices.
Conclusion
Lifting and holding patients’ limbs during the surgical preparation process, using the assistive device, had the following advantages for preoperative team members: facilitating the preparation process by reducing the duration of the process and number of nurses involved in it. In addition, nurses who used this assistive device were more satisfied with their work compared with those who used the traditional manual preparation method.
It could be inferred that use of this assistive device may reduce injuries to patients during the preparation process and the rate of MSDs among OR nurses; however, further prospective investigations are needed.
Thus, to reduce muscle fatigue and the risk of MSDs related to inconsistency between staff physical capabilities and weight of patients’ limbs, time to complete the preparation process, and the number of nurses needed for limb preparation, the use of this assistive device is recommended.
Footnotes
Acknowledgements
The authors thank the clinical research development unit (CRDU) of 5 Azar Hospital affiliated with Golestan University of Medical Sciences (Gorgan, Iran) for their consultations, operating room (OR) nurses and patients for their participation, and invention and innovation committee of research and technology department of Golestan University of Medical Sciences for financial support (Grant No. 2588), review, and scientific approval of this device.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported financially by Grant (No. 2588) of research and technology department of Golestan University of Medical Sciences, Gorgan, Iran.
Author Biographies
Mohammad Taghi Mojeni is an operating room nurse in Gorgan, Iran.
Soroosh Aminolsharieh Najafi graduated in medicine in 2013 from Golestan University of Medical Sciences, Gorgan, Iran. He has several publications in different fields in medicine.
Mahin Nomali completed her BS in nursing with first class honors in 2012 from Golestan University of Medical Sciences, Gorgan, Iran. She has been a member of the International Council of Nurses since 2012. She has an effective involvemet in research activities and several paper publications. In addition, she has experience as an emergency nurse at the general hospital and as clinical assistant researcher at the research and technology department of Golestan University of Medical Sciences, Gorgan, Iran.