
Abstract
This study was designed to determine the effect of an academic–workplace partnership intervention, “3,000 more steps,” on improving physical activity (PA) and body composition of workers, and compare the characteristics of those workers who completed and did not complete the program. Participants were 70 sedentary office workers from an airline company. Pedometers determined their daily steps, and body composition was compared before and after the 8-week intervention; 39 of 70 (55.7%) participants completed the program. Daily steps increased from 5,811 to 9,240, and fat mass, waist–hip ratio, and body mass index (BMI) decreased for the completers. Non-completers had lower average PA and higher average fat mass at baseline than did completers. Overall, a workplace PA program could be successfully undertaken by occupational health nurses and a research team in partnership. However, to implement a cost-effective intervention program for inactive workers, further research is needed to ascertain why some workers do not complete the program.
Lack of physical activity (PA) is the fourth most frequent cause of mortality worldwide, resulting in 3.2 million deaths annually (World Health Organization [WHO], 2014). PA is declining in the home, at the workplace, and at school (WHO, 2013). In 2008, the WHO reported that globally about one third of adults over 15 years of age have a sedentary lifestyle (WHO, 2008). Recent statistics show that only 23% of Korean adults engage in the recommended level of moderate or vigorous leisure-time PA compared with 50% of American adults (Healthy People 2020, 2012; Ministry of Health and Welfare & Korea Centers for Disease Control Prevention, 2013; WHO, 2011).
Korean adults work significantly longer hours (i.e., an average of 2,090 hours each year) compared with the Organization for Economic Cooperation and Development (OECD) country average of 1,776 hours per year (OECD, 2013). Sedentary workers spend 50% of their time at work resulting in fewer opportunities to participate in PA; obesity is an outcome of this lifestyle (Chan, Ryan, & Tudor-Locke, 2004). Thus, the workplace is an ideal setting to offer sedentary workers structured activities to improve PA (Conn, Hafdahl, Cooper, Brown, & Lusk, 2009; WHO, 2013).
Scientific evidence supports that worksite PA programs improve worker health and worksite outcomes (Aldana, Merrill, Price, Hardy, & Hager, 2005; Conn et al., 2009). Recent trends suggest that comprehensive worksite health promotion and disease management programs emphasize individualized risk reduction for all employees, particularly at-risk employees (Pelletier, 2011).
To achieve health benefits, moderate aerobic exercise for at least 150 minutes per week, 30 minutes per day 5 days each week, is recommended for adults aged 18 to 64 years (WHO, 2011). If this goal is converted into steps, adults must walk 3,000 more-than-usual steps per day at least 5 days each week to reach the WHO’s recommended exercise level (Marshall et al., 2009). A step count goal is commonly used to increase PA (Jensen, Roy, Buchanan, & Berg, 2004), and pedometers are widely used as objective measurement tools. Systematic reviews show strong evidence that tailored interventions using pedometers is effective for sedentary individuals (Ogilvie et al., 2007).
Significant resources must be invested to develop and implement health promotion programs. Companies are increasingly demanding clinical and cost outcomes to justify corporate investments in workplace health promotion interventions (Pelletier, 2011). However, 25% to 65% of participants did not complete these programs (Atkins et al., 1990; Chan et al., 2004; Dishman, DeJoy, Wilson, & Vandenberg, 2009; Dishman, Oldenburg, O’Neal, & Shephard, 1998; Toft et al., 2007). A high non-completer rate affects programs’ cost-effectiveness because these workers do not receive program benefits. However, few worksite PA interventions have explored why employees fail to complete these programs.
This pilot study’s purpose was to investigate the effects of the “3,000 more steps” program, developed and implemented through an academic–workplace partnership to improve PA and body composition. The study further investigated the reasons workers failed to complete the program by comparing the characteristics of the program’s completers and non-completers.
Method
The researchers used an 8-week single-group pre-posttest design to evaluate the “3,000 more steps” program. The intervention ran from March 28, 2012, to April 5, 2012, and was conducted at a commercial airline company in Seoul, South Korea. A convenience sample of 70 eligible workers was recruited via the company’s intranet bulletin board. Self-report eligibility criteria included the following: age 30 to 55 years, white-collar employee, mobile phone user, no illnesses preventing the worker from walking, currently exercising less than 3 times per week, and not currently enrolled in other health promotion programs. Participant were considered non-completers if they missed the last monitoring session.
Measures
Primary outcome measures were changes in PA and body composition at 8 weeks. Secondary outcomes were changes in perceived exercise self-efficacy and exercise benefits.
Primary outcomes
PA was measured using a pedometer to record daily accumulated steps (Yamax CW700/701, Yamax Corporation, Tokyo, Japan). This model demonstrated acceptable reliability for use in research studies. Yamax Digi-Walker models demonstrated acceptable accuracy (within ±3% of the actual steps taken) and reliability (Cronbach’s alpha ≥ 0.80) in a previous study (Schneider, Crouter, Lukajic, & Bassett, 2003). Participants were instructed to wear their pedometer during waking hours.
A body composition analyzer (Inbody 720, Biospace, Seoul, Korea) was used to measure fat mass, waist–hip ratio, and body mass index (BMI). Participants were instructed to wear light clothes and stand upright, stepping on the foot electrodes and loosely gripping the hand electrodes.
Secondary outcomes
Perceived exercise self-efficacy was measured using a translated version (Shin, Jang, & Pender, 2001) of the Exercise Self-Efficacy scale (Bandura, 1997), 18 questions with a range of scores from 0 to 100. A higher score represents a higher level of exercise self-efficacy. The Cronbach’s alpha for this instrument was .90 in the present study.
Perceived exercise benefit was measured using a translated version (Jang & Shin, 1999) of the Exercise Benefit/Barrier scale (Sechrist, Walker, & Pender, 1987), 27 questions with answers ranging from 1 (absolutely not) to 4 (very much so). A higher score represents a more positive perception about the benefits of exercise. Thirteen questions about the barriers to exercise had answers ranging from 1 (very much so) to 4 (absolutely not); the higher the score, the lower the barriers to exercise. In both domains, higher scores signified that exercise was perceived positively. Therefore, the barriers to and benefits of exercise were integrated into a single variable in this study; possible scores ranged from 1 to 4, the average score of each question. Cronbach’s alpha was .78 for this instrument in the present study.
Demographic characteristics included age, gender, marital status, household income, job experience, chronic illnesses, smoking habit, and previous exercise habit.
Intervention
The principles of community-based research (Israel, Schulz, Parker, & Becker, 1998) were used to establish this academic–workplace partnership intervention. The principle investigator had previous experience working as an occupational health nurse at the intervention workplace; therefore, the researchers had an understanding of workplace characteristics and effective strategies for establishing the partnership.
Six individuals formed the steering committee for “3,000 more steps”; the executive director, medical team manager, two occupational health nurses, and two researchers were involved throughout the intervention’s development, implementation, and evaluation.
Social cognitive theory is widely used as the theoretical base for PA programs. In particular, self-efficacy is a construct that has been found to play a pivotal role in behavioral change, and its effectiveness in PA promotion has been demonstrated in previous studies (Darker, French, Eves, & Sniehotta, 2010; Kaewthummanukul & Brown, 2006). This program was developed by focusing on increasing self-efficacy as suggested by social cognitive theory. The method and application used in the program are shown in Table 1. The program incorporated the WHO’s suggested PA level (number of steps); thus, the program was named “3,000 more steps” (Marshall et al., 2009).
Intervention Methods and Applications
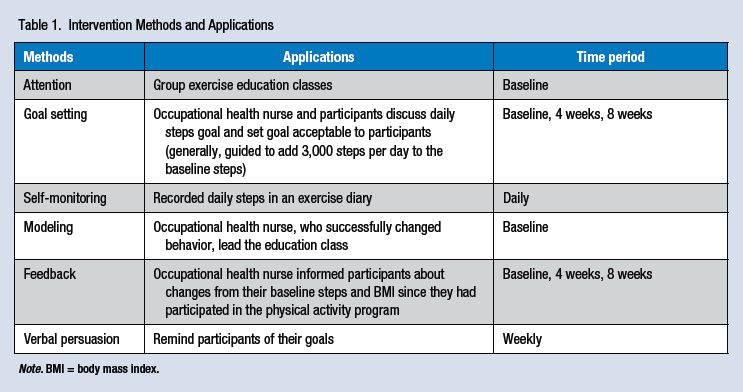
Note. BMI = body mass index.
One week before baseline data collection, participants were given pedometers and directed to go about their daily lives as usual for at least 3 days using their pedometers. The next week, at the end of the baseline investigation stage, an occupational health nurse provided a 30-minute lesson about the health effects of exercise. Body composition analysis and the survey were offered to all participants after the lesson. Then participants learned about their body composition through one-on-one consultation with an occupational health nurse and established their PA goals for the next 4 weeks based on their current average daily steps. As a general rule, the PA goal was set by adding 3,000 steps to their regular activity (e.g., household chores, working hours, commuting hours, and leisure activities) and participants decided the level they wanted to attain. Participants visited the worksite occupational clinic Weeks 4 and 8 to re-measure body composition and set new goals.
All enrolled participants received a booklet and a pedometer. Participants who completed evaluations at Weeks 4 and 8 were given a gift worth US$15 (e.g., jump rope, vitamins) after each visit.
Data Analysis
Collected data were analyzed using IBM SPSS Statistics 20.0; pre- and post-intervention values on the measures were compared by paired t test. To assess differences in primary outcomes, secondary outcomes, and general characteristics between program completers and non-completers, the χ2 test and Student’s t test were used.
Ethics
This study was approved by the institutional review board (IRB No. 2011-0018). The purpose, procedure, and anonymity policy were explained to all participants before the program’s commencement and informed written consent was obtained from all participants. All participants were informed of their right to leave the program at any time during the study.
Results
General Participant Characteristics
Table 2 shows participants’ (N = 70) general characteristics. The average age was 38 years (SD = 8.14), sex distribution was equal, and a majority of participants were married. Average monthly household income was US$5,982 (SD = 2,562), and their average work period was 162 months (SD = 86.86). Some participants had chronic illnesses (24.3%), smoked (8.6%), and previously exercised regularly (17.1%).
Comparison of Program Completers and Non-Completers
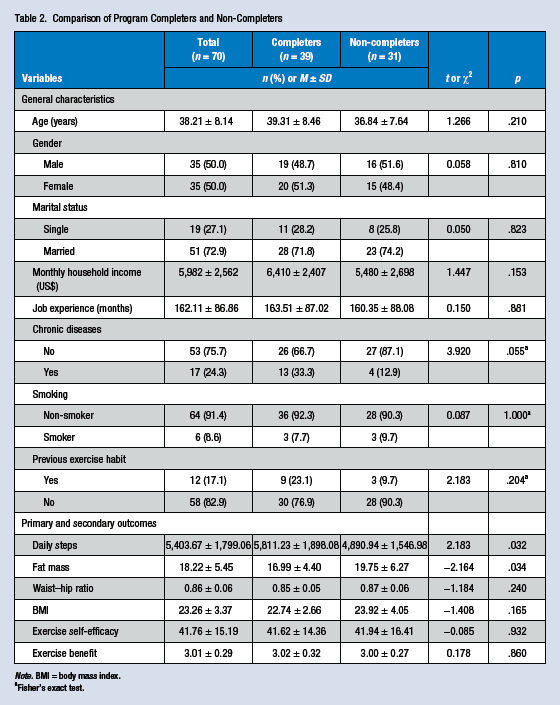
Note. BMI = body mass index.
Fisher’s exact test.
Changes in Primary and Secondary Outcomes for Program Completers
Table 3 shows the results of the primary and secondary outcomes that changed through the 8-week intervention program. For primary outcomes, the daily number of steps was 5,811 at pre-intervention, which rose by 3,429 steps to 9,240 after 8 weeks (t = −6.617, p < .001). At post-intervention, fat mass (t = 2.916, p = .006), waist–hip ratio (t = 4.729, p < .001), and BMI (t = 3.663, p = .001) showed significant decreases. Exercise self-efficacy was 41.62 pre-intervention, rising to 42.80 after 8 weeks; however, this finding was not statistically significant. Perceived benefit of exercise was 3.02 pre-intervention and 3.03 after 8 weeks; this finding was not statistically significant.
Changes in Primary and Secondary Outcomes in Program Completers (n = 39)
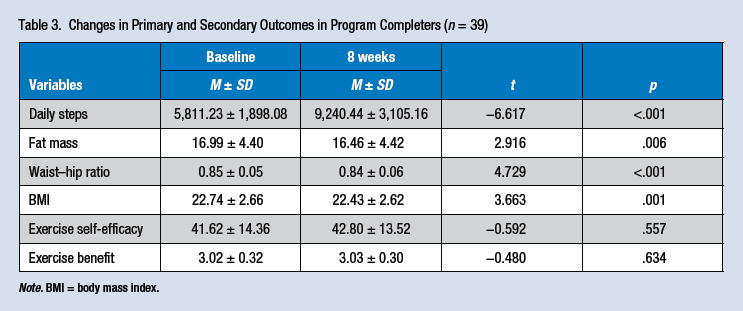
Note. BMI = body mass index.
Comparison Between Program Completers and Non-Completers
This study began with 70 study participants, but only 39 workers finished the entire 8-week program. Table 2 shows a comparison of the general characteristics and primary and secondary outcomes between program completers and non-completers at baseline. The number of daily steps for the completers was 5,811, and for the non-completers 4,890 (t = 2.183, p = .032). A statistically significant difference between fat mass of the program completers (17.0%) and the non-completers (19.8%; t = −2.164, p = .034) was also found.
Eight of the 31 non-completers replied when called or emailed about their reasons for not completing the program. They noted frequent business trips, vacations, work business, and difficulties wearing the pedometer. In addition, workers commented they had “a loss of motivation to continue participating after discouraging goal-reaching efforts at the initial stages of the program” and “being monitored was uncomfortable.”
Discussion
The 39 completers transitioned from an “inactive” group, with a daily average of 5,811 steps pre-intervention, to a “relatively active” group, with a daily average of 9,240 steps, an increase of 3,429 (Tudor-Locke & Bassett, 2004). Participants established their goals twice during the intervention period, at baseline and after the fourth week. The goal was set by adding 3,000 steps per day to the average number of steps at baseline. In addition, a goal was set to maintain their current level when their daily average reached 10,000 steps. Therefore, if program completers recorded an average of 9,240 steps, they were close to the goal of the “3,000 more steps” intervention. In addition, noticeable improvements in fat mass, waist–hip ratio, and BMI were achieved.
The program completers showed a significant increase post-intervention in primary outcomes, but no significant difference in self-efficacy or perceived benefits of exercise. In Clarke et al.’s (2007) research targeting obese women, the researchers reported that PA level and self-efficacy significantly increased post-intervention. Even in an intervention study targeting college women, the group with greater participation had greater increases in self-efficacy and perceived benefit scores than did the group with lower participation (D’Alonzo, Stevenson, & Davis, 2004). However, De Cocker, De Bourdeaudhuij, and Cardon (2008) reported that an intervention group using a pedometer and receiving cognitive and behavioral support showed no differences in PA increase compared with the group that only used a pedometer. This finding demonstrates that simply providing a pedometer was enough to increase PA without specifically addressing cognitive and behavioral factors.
Participants were considered non-completers if they missed the last monitoring session. During the 8 weeks of intervention, 31 participants did not complete the program, a non-completion rate of 44.3%. Considering the program’s voluntary nature, workers who chose to complete the worksite PA program could possess other characteristics, such as more motivated regarding PA, than non-participants (Aldana et al., 2005; Bravata et al., 2007; Dishman et al., 2009). More than half (16) of the participants left the program before Week 4, during the early stage of the intervention. In a study that targeted women for a 16-week aerobic exercise program, 82.5% left the program in the early stages, and 43.5% left the program before the end of the first week (Arikawa, O’Dougherty, Kaufman, Schmitz, & Kurzer, 2012). This finding suggests the need for a variety of strategies to prevent individuals from leaving the program in the early intervention phase.
To support the adoption and integration of worksite PA interventions, meaningful incentives and awards should be provided to the program’s participants. Incentives should encourage participants’ internal motivation to be physically active (Pronk & Kottke, 2009). In this study, participants received a pedometer at enrollment and a gift worth US$15 (e.g., jump rope, vitamins) after each monitoring visit. It could be that those gifts did not appeal to well-educated, white-collar workers; in addition, although incentives might increase response rate, monetary incentives, especially prepaid incentives, are more effective than gifts in survey research (Singer & Ye, 2013). Further studies are needed to ascertain which incentives are most effective for retaining participants in PA workplace interventions.
Eight workers responded when contacted about their reasons for leaving the program before completion. Common responses were that they lacked time to participate due to frequent business trips and busy work schedules; others identified difficulty wearing the pedometer and loss of motivation to participate after discouraging efforts at the program’s outset. In a health promotion program targeting construction workers, the main reason for leaving the program was loss of interest or lack of motivation (Groeneveld, Proper, van der Beek, Hildebrandt, & van Mechelen, 2009). Another key reason is lack of time (Arikawa et al., 2012). Those results are consistent with the present study’s findings.
Leaving the program due to busy work schedules could be a convenient excuse. Monitoring took place at the workplace occupational health clinic providing easy access for workers. Participants were informed about the monitoring schedules 1 week in advance through text messages and emails, and were encouraged to make an appointment at a convenient time during a 1-week period. Therefore, future research with in-depth analysis is needed to ascertain the actual reasons participants do not complete these programs.
Baseline measurements were compared to determine differences in characteristics between the 39 program completers and 31 non-completers. The average step number for non-completers was 4,890 steps; this number was significantly less than the program completers’ 5,811 steps. Arikawa et al. (2012) indicated that the baseline PA level is a significant predictor of program adherence because the chances of finishing the program are higher if the PA level is high at baseline. In addition, non-completers had higher fat mass compared with completers. Previous research has also shown that those individuals who are more obese are more likely to participate in diet and exercise interventions but are also more likely to leave programs prior to completion (Toft et al., 2007). It may be that those individuals most likely to gain the most benefit from a PA intervention program have the greatest risk of non-completion. Therefore, intervention programs targeting obese and sedentary workers must include various evidence-based intervention strategies.
Limitations
This study examined the intervention effects on a single group, limiting its ability to differentiate the effects of social cognitive factors and pedometers on sedentary workers’ PA levels. Further studies using multiple treatments and a controlled design are needed to determine the difference between groups whose intervention uses social cognitive factors and pedometers and groups whose intervention only uses pedometers.
The program completers demonstrated increased PA and improved body composition after the relatively short period of 8 weeks. However, it is unknown if these improvements continued long term. An academic–workplace partnership was pursued and occupational health nurses, a manager, and an executive member participated in all program components, including designing the intervention, recruiting the participants, and providing incentives. Workers had no opportunities to participate in these aspects of the program.
The authors compared the characteristics of the program’s completers and non-completers; however, employees who participated in this worksite PA program could possess characteristics that differ from non-participants. To increase worksite PA program participation, future studies should again examine the reasons for non-participation.
Implications for Practice
This study confirmed that through collaboration and appropriate division of roles, a workplace intervention could be undertaken successfully by a partnership between occupational health nurses and researchers. The 8-week program assisted program completers to increase their daily average steps by 3,429, thereby transforming them from an “inactive” group to a “relatively active” one.
However, 44.3% of participants left the program during the 8-week intervention; half of the non-completers left the program during the intervention’s beginning stages. To operate a successful program to improve workers’ health, a steering committee consisting of occupational health nurses, researchers, and workers is needed. This committee composition would enable workers to provide critical input, such as the types of interventions that most interest them and attractive incentives for program participation and retention. Because busy workers can leave the program due to frequent travel, occupational health nurses should consider PA programs for employees who travel frequently.
Applying Research to Practice
Pedometer-based tailored worksite health promotion programs can increase physical activity and improve health outcomes in sedentary office workers. Various strategies should be implemented in the early intervention phase to prevent high risk workers (e.g., more obese and inactive individuals) from leaving the program. A steering committee consisting of occupational health nurses, researchers, and workers can play a pivotal role in facilitating active participation and high retention of inactive workers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Dr. Duckhee Chae has had more than 15 years of OHN experience. She currently teaches community health nursing and conducts research on health promotion for workers and cultural competence of health care workers.
Mrs. Suhee Kim is a graduate student currently working on her doctoral dissertation. She is interested in community health nursing, especially about the physical activity of workers and the obesity of adolescents.
Dr. Yunhee Park has had more than 10 years of nursing experience. She is interested in HIV and heart disease of workers and conducts research on health promotion for workers.
Mrs. Youngmee Hwang is manager of Asiana Medical Services. She has worked as an OHN more than 10 years, improving workers’ health.