
Abstract
A 22-year-old man sought care at an orthopedic clinic for acute plantar fasciitis. He reported that he had begun an intensive exercise program to prepare himself for Marine Corps Officer Candidate School. Pes Planus, or flat feet, was noted on physical examination. This article reviews the diagnoses of pes planus and plantar fasciitis as well as current intervention strategies.
A 22-year-old man presented in an orthopedic clinic complaining of pain in the left plantar heel for the past month. Pain was worse with high-impact activities, moving from a sitting to a standing position or getting out of bed in the morning; however, pain decreased after a few steps. The client stated that he had been in an intense workout regimen for the past 6 months and was about to enter the Marine Corps Officer Training Program that requires each candidate to run long distances while carrying heavy equipment. He denied other health problems or past surgeries and stated that he might take an ibuprofen on occasion for generalized muscle strains.
During the physical examination, tenderness and pain were documented on the origins of the plantar fascia from the medial tubercle of the calcaneus. X rays revealed no structural abnormalities. Also noted on physical examination, the client had bilateral flat feet. The diagnosis was plantar fasciitis.
Pes Planus or Flat Feet
Pes planus, or flat feet, is a condition in which the feet have a flat longitudinal arch that comes into nearly complete contact with the floor when standing, and results in excessive pronation of the foot (Buchbinder, 2004). No universal clinical guidelines detail the parameters of normal arch height (Ashford, Kippen, & Rome, 2009). Three types of pes planus have been documented. Rigid pes planus is defined as congenital, rigid, or spastic deformity. Flexible pes planus is an acquired joint disorder that results in a valgus foot deformity (Banwell, Mackintosh, & Thewlis, 2014). Posterior tibial dysfunction pes planus occurs when the arch of the foot provides an elastic component between the forefoot and the hind foot that dissipates the forces during weight bearing. In pes planus, the head of the talus bone is displaced medially and distally from the navicular, which results in stretching the tibialis posterior muscles, leading to loss of function in the medial longitudinal arch (Banwell et al., 2014).
Approximately 23% of the population has one type of pes planus (Banwell et al., 2014). Symptoms may include foot pain in the arch and heel, and fatigue with prolonged standing. The etiology of pes planus may include a history of excessive rear foot eversion, abnormal foot and ankle loading forces, and altered muscle activation with ambulation (Ashford et al., 2009). Factors that contribute to pes planus are excessive tension in the triceps surae, obesity, posterior tibial dysfunction, or ligamentous laxity in the spring ligament, plantar fascia, or other supporting plantar ligaments (Ashford et al., 2009). Long-term consequences of untreated pes planus include Achilles tendinopathy, osteoarthritis, and associated patellofemoral disorders (Banwell et al., 2014). A diagnosis is dependent on visual inspection of the foot and the “wet footprint test” that involves placing the feet on a wet, soft surface and noting the footprint left on the surface. Radiographs may not be necessary for diagnosis (Ashford et al., 2009). Pes planus may contribute to decreased mobility and acute or chronic injuries (Ashford et al., 2009).
Interventions
If needed, footwear consisting of a rigid, semi-rigid, or soft arch support or orthotic may provide support and pain relief. Orthotics may improve excessive rear foot eversions and abnormal loading forces on the feet (Ashford et al., 2009). Anti-pronatory strapping and stretching exercises may also be considered (Ashford et al., 2009). For optimal benefit of foot orthosis, custom-molded orthotics should be considered (Hossain & Jobanputra, 2011).
Plantar Fasciitis
Plantar fasciitis can be caused by an acute injury, but leads to a debilitating condition such as plantar fasciosis, a chronic degenerative condition (Neufeld & Cerrato, 2008). Plantar fasciitis may be referred to as “heel pain syndrome,” and it is the inflammation of the plantar fascia and the surrounding perifascial structures. The inflammatory response is the result of microtears of the fascia, collagen necrosis, angiofibroblastic hyperplasia, and chrondroid metaplasia resulting in pain (Buchbinder, 2004).
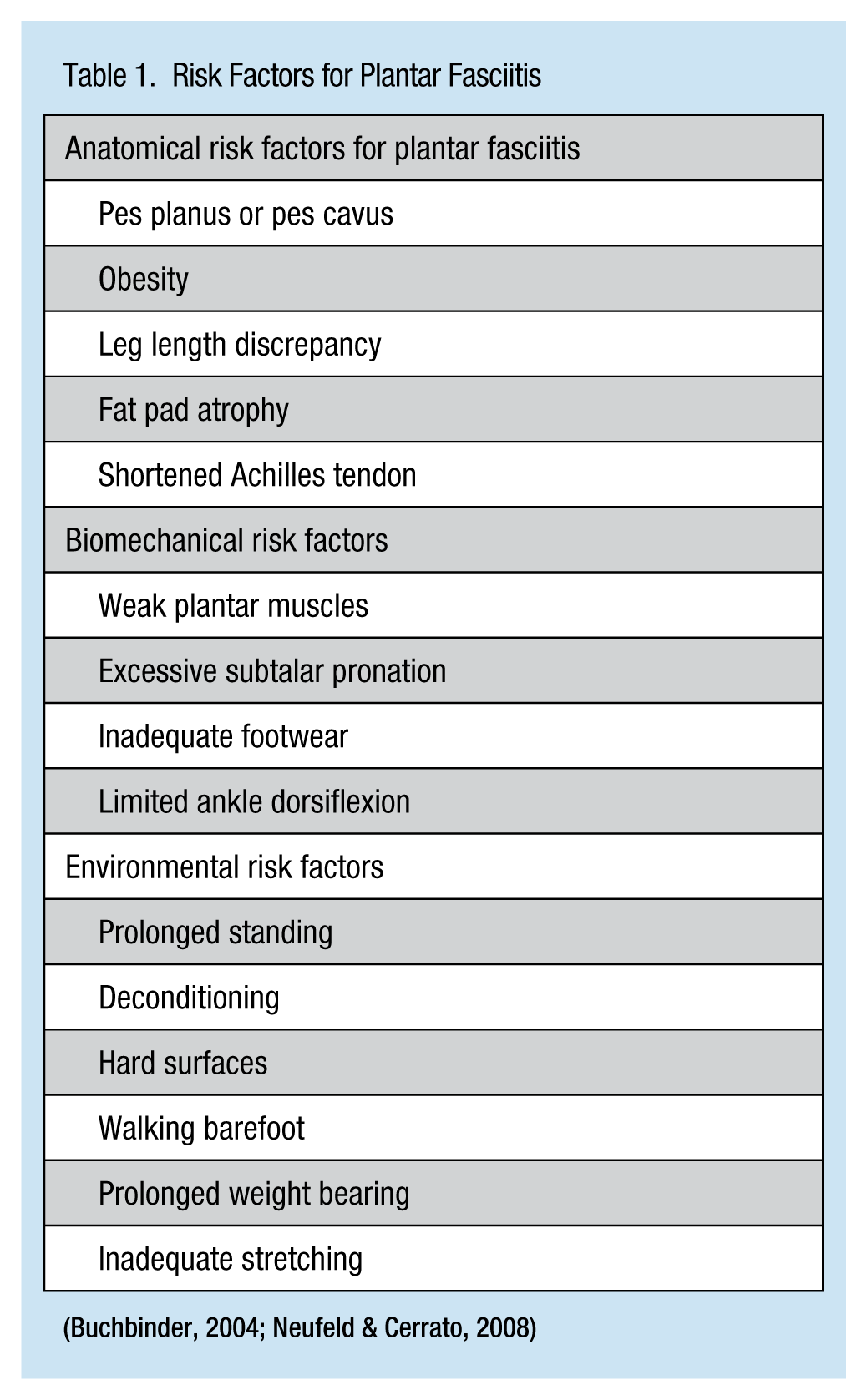
It is estimated that 1 in 10 individuals will experience plantar fasciitis during their lifetime (Neufeld & Cerrato, 2008). Risk factors include running and other high-impact activities, occupations that require prolonged standing, pes planus or pes canvus (high arches), limited ankle dorsiflexion less than 10°, and obesity (Buchbinder, 2004; see Table 1).
Risk Factors for Plantar Fasciitis
The plantar fascia originates in the anteromedial aspect of the calcaneus and spreads to all five digits in the foot that forms the longitudinal arch. The plantar fascia is an inelastic band and when walking, tension increases on this fascia. There is also a fibrofatty subcutaneous tissue beneath the fascia that absorbs the majority of the body weight (Buchbinder, 2004). A fat pad on the calcaneus also absorbs these increased loading forces. These protective areas diminish with age (Buchbinder, 2004).
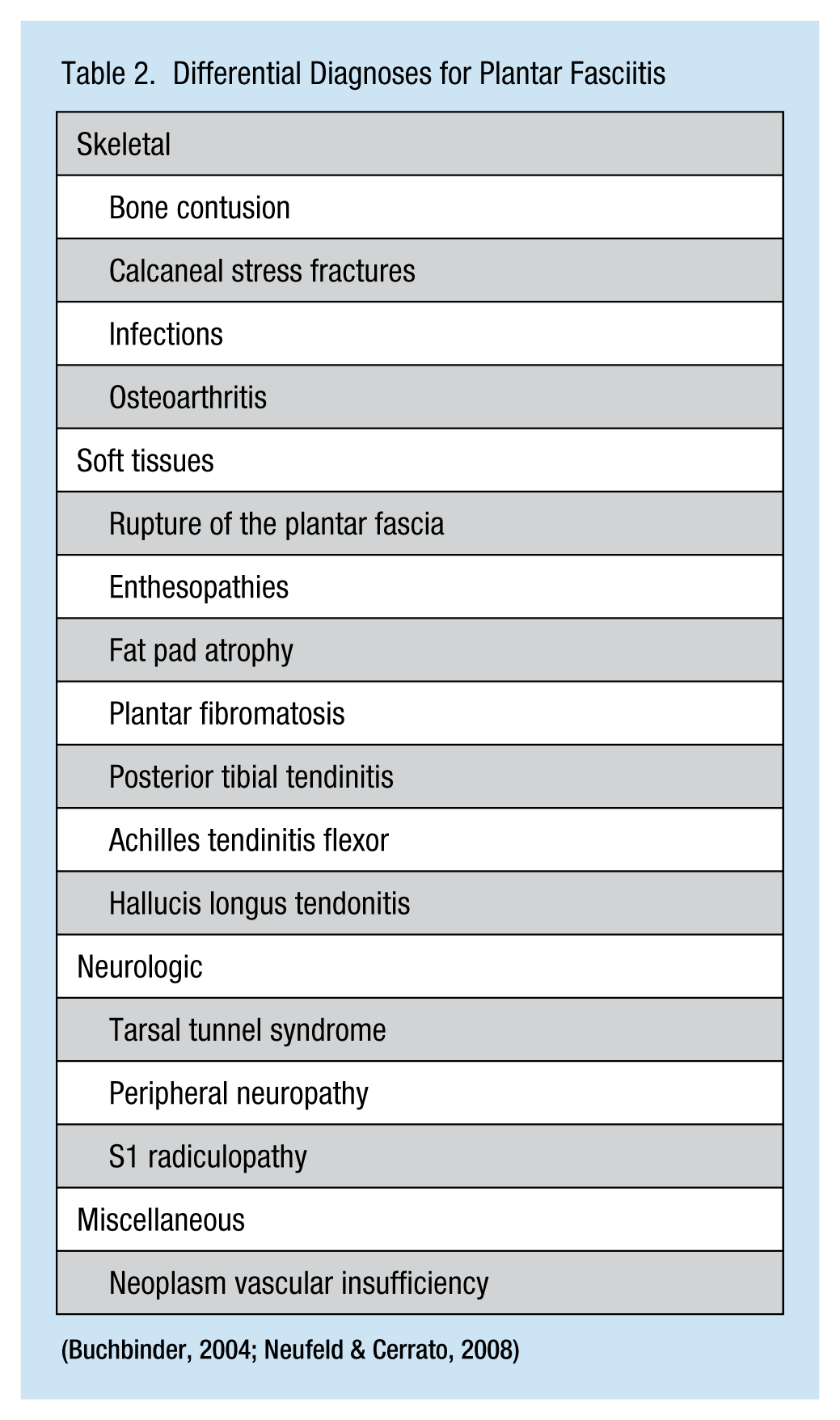
Individuals usually report a gradual onset of inferior heel pain that is worse when getting out of bed and walking a few steps; pain increases with high-impact activities or after prolonged standing. Pain is localized to the insertion of the plantar aponeurosis at the medical tubercle of the calcaneus (Buchbinder, 2004). Associated paresthesias are common (Buchbinder, 2004). Differential diagnoses are found in Table 2. During physical examination, any deformities or contractures, such as pes planus and leg length discrepancies, should be noted. Inspection consists of assessing the Achilles tendon/muscle and noting any contractures. A full lower body neurologic examination should be conducted to identify any neurologic deficits that may be associated with an S1 radiculopathy. X rays can be used to identify calcaneal stress fractures. Magnetic resonance imaging (MRI) may be ordered to visualize the plantar fascia, revealing plantar fascia thickness with edema and microtears (Buchbinder, 2004).
Differential Diagnoses for Plantar Fasciitis
Interventions
Conservative treatment is the best practice for plantar fasciitis. A course of anti-inflammatory medications reduces inflammation and pain. Foot orthoses are designed to relieve the biomechanical load during weight bearing as well as decrease excessive pronation. Foot orthotics may be referred to as “arch supports,” which are made of prefabricated silicone or rubber heel cups, felt pads, and custom arch supports. Arch supports provide stabilization of the mid-foot structure and reduce loading forces (Dyck & Boyajian-O’Neil, 2004). Adequate footwear with well-supported arches and a minimal heel height of 1 inch is recommended for prolonged standing and walking (Dyck & Boyajian-O’Neil, 2004).
Physical therapy may consist of icing, moist heat, and massage. A stretching program optimizes tissue tension and provides increased mobility that targets the plantar fascia and gastrocsoleus–Achilles complex (Dyck & Boyajian-O’Neil, 2004). Home exercises may consist of rolling a tennis ball under the arch of the foot (Dyck & Boyajian-O’Neil, 2003). Steroid injections may be considered but have limited effectiveness (Lemont, Ammirati, & Usen, 2003). Botulinum toxin A may be effective, but needs further investigation (Lemont et al., 2003). Extracorporeal shock-wave therapy may be used to stimulate healing of the soft tissues and promote vascularization by releasing local growth factors and inhibiting pain receptors; however, the effectiveness of this therapy has not been demonstrated (Buchbinder, 2004). Plantar fasciitis may be considered self-limiting; however, for persistent cases, a plantar fasciotomy may be considered.
Implications for Occupational Health Nurses
In the occupational setting, employees required to stand for the majority of their shifts may be at risk of developing plantar fasciitis. During pre-placement screening, the occupational health nurse should inspect the feet to assess for flat feet or high arches and other risk factors for plantar fasciitis, especially if the worker’s job description requires excessive walking or prolonged standing. Recommendations may include footwear fitted for comfort and arch supports and mid-soles that absorb forces during prolonged standing and walking (Buchbinder, 2004).
If employees develop plantar fasciitis, they may be given sitting duties to relieve the micro trauma caused by repetitive overload. Non-steroidal anti-inflammatory medications may be prescribed as well as physical therapy for conservative treatment. If symptoms do not resolve in a timely manner, podiatry may be consulted.
Conclusion
Under military physical requirements, pes planus presents no structural or biomechanical limitations and, therefore, should not be a disqualifying characteristic for future Marine Corps officers. For this individual, foot orthotics for prolonged standing and ambulation may help. Due to his history of pes planus, the future Marine Corps officer may be at risk of developing further episodes of plantar fasciitis. However, plantar fasciitis may be a self-limiting physical condition, but the individual may need to continue routine stretching exercises, wear comfortable shoes with arch supports, and take anti-inflammatory medications when needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann R. Lurati, ARNP, DNP, ACNP-BC, COHN-S, is an occupational health nurse practitioner at the University of South Florida.