
Abstract
Meal breaks promote occupational health and safety; however, less is known about supervisors’ support for nurses’ meal breaks. In this study, the researchers tested whether the frequency of meal breaks was positively related to supervisors’ support of nurses’ meal breaks, and whether more frequent meal breaks were associated with less psychological distress. This study is based on a cross-sectional survey of 1,595 hospital nurses working on 85 units supervised by nursing directors. Specific meal-break support was measured at the nursing director level; frequency of meal breaks and psychological distress were measured at the individual nurse level. Multilevel adjusted models showed a positive association between supervisors’ support for meal breaks and the frequency of nurses’ meal breaks (β = .16, p < .001). Moreover, nurses who took meal breaks more frequently reported lower psychological distress (β = −.09, p < .05). Meal breaks might be daily opportunities to promote mental health and fatigue recovery and provide downtime.
The organization of breaks and rest periods has repercussions for occupational health and safety (Johnson & Lipscomb, 2006). Multiple studies have established that breaks reduce a myriad of adverse occupational outcomes (Tucker, 2003; Tucker, Lombardi, Smith, & Folkard, 2006), including mental health problems (Geiger-brown, Muntaner, Lipscomb, & Trinkoff, 2004). Moreover, workplace intervention research has demonstrated that the introduction or enforcement of breaks can reduce occupational stress and work-related illnesses (Silverstein & Clark, 2004). Review studies have highlighted two areas for further research to better illuminate the causal pathways linking breaks with health outcomes: the assessment of workplace factors that influence break practices, including psychosocial predictors (Tucker, 2003), and the differentiation of health effects by specific types of breaks (Trougakos & Hideg, 2009). In this study, the researchers addressed these gaps, focusing on a particular type of break, meal breaks, to estimate their association with workers’ mental health in a sample of hospital nurses. The researchers focused on supervisors’ meal break support as a psychosocial occupational factor that could influence workers’ break practices and their health and safety.
Scientific Gaps on the Health Effects of Breaks
Although studies have examined the association between work breaks and health outcomes based on the onset or timing of breaks, less is known about the activities or behaviors workers engage in during breaks. By analyzing specific types of breaks, their impact on worker health and safety could be better understood. Meal breaks have received particular attention because they are subject to labor regulations and are a marker of quality employment (Ghai, 2006). Too little time and inappropriate conditions for meal breaks are barriers to healthy eating (Faugier, Lancaster, Pickles, & Dobson, 2001) and are related to low job satisfaction (Sveinsdottir, Biering, & Ramel, 2006).
Although the evidence suggests that organizational arrangements unsupportive of breaks are harmful, less is known about workplace factors that could influence, support, or facilitate these practices. With the exception of worksite interventions, little research has attempted to disentangle individual (e.g., needs and preferences) versus external factors that affect the association between breaks and health outcomes (Tucker, 2003). The assessment of interpersonal characteristics as determinants of break practices may shed light on which external and modifiable psychosocial workplace factors affect both workers’ breaks and health outcomes.
Interpersonal relationships between supervisors and workers are salient indicators of the psychosocial work environment. Supervisors’ support, defined as the availability and quality of assistance that support workers’ behaviors, is a workplace factor with implications for workers’ well-being (Kossek, Pichler, Bodner, & Hammer, 2011). Supervisory support could be manifested in the provision of resources such as information, appraisal, or instrumental assistance (Berkman & Glass, 2000). Furthermore, the content and type of support, either general perceptions of assistance, action, or context-specific help, might inform more clearly how supervisors influence both organizational behaviors and workers’ health. In this sense, a meta-analytic study based on 85 articles concluded that specific supervisors’ support for work–family interface was a stronger predictor of better integration of these domains compared with the effect of general supervisors’ support (Kossek et al., 2011). It is possible, then, that supervisors’ specific support might be more relevant to elicit intended behaviors, above and beyond general perceptions that supervisors are helpful.
Breaks and Health Among Patient Care Workers
Patients care workers are exposed to multiple time-related demands, increasing their risk for adverse occupational health outcomes (Brown & Brooks, 2002). Many nurses do not take regular breaks (Khowaja, Merchant, & Hirani, 2005), and frequently cited reasons include job demands, understaffing, and non-supportive supervisory styles (Shields & Wilkins, 2006). Anecdotal evidence suggests that supportive supervisory styles in which supervisors, nursing staff, and patients plan meal breaks together not only facilitate taking breaks but could also foment social support among coworkers and supervisors (Stefancyk, 2009). The potential influence of nursing directors on workers’ meal breaks, however, requires further investigation. A few studies have assessed the effect of management and supervisors’ attitudes on nurses’ mental health (O’Donnell, Ertel, & Berkman, 2011). Although social support from supervisors has been linked to fewer sleep problems and musculoskeletal disorder (MSD) symptoms and healthier behaviors (Sembajwe et al., 2013; Sorensen et al., 2011), it is unclear whether supervisors’ general or specific support could influence the frequency of workers’ breaks and consequent health outcomes.
More puzzling is the inconclusive evidence regarding the mental health effects of break practices among nurses (Camerino et al., 2008). Although some studies have shown that consecutive shifts without break periods were linked to mental health problems (Geiger-brown et al., 2004), other studies have concluded that neither the number of breaks per day nor the length of meal breaks was associated with mental health (Nabe-Nielsen, Garde, & Diderichsen, 2011). The evidence regarding other outcomes is also mixed; a study among hospital nurses found no association between lack of breaks and MSD symptoms (Lipscomb, Trinkoff, Geiger-Brown, & Brady, 2002), although another longitudinal assessment found that lower frequency of breaks per day predicted more low back symptoms (e.g., pain, numbness, tingling, aching, stiffness, or burning) 1 year later (Trinkoff, Le, Geiger-Brown, Lipscomb, & Lang, 2006). Studies have found that nurses who took more breaks averaged higher job satisfaction and lower body mass index compared with nurses who took breaks less frequently (Han, Trinkoff, Storr, & Geiger-Brown, 2011; Nahm, Warren, Zhu, An, & Brown, 2012).
Study Aims
The aims of this study were twofold: first, to test whether nurses’ frequency of meal breaks was influenced by break-specific supervisor support, and second, to determine whether higher frequency of nurses’ meal breaks were associated with lower psychological distress. The setting for this study was two teaching hospitals in the Boston area that were part of the same health care organization. Hospital nursing directors supervised a group of workers or a unit. The researchers contemplated a multilevel framework where break-specific support (i.e., facilitation of meal breaks) was measured at the nursing director level, and psychological distress was measured at the individual nurse level. In addition, they assessed general supervisor support (i.e., reports of the extent to which nurse participants perceived their supervisors to be helpful) measured at the individual nurse level. Three main hypotheses were tested:
Method
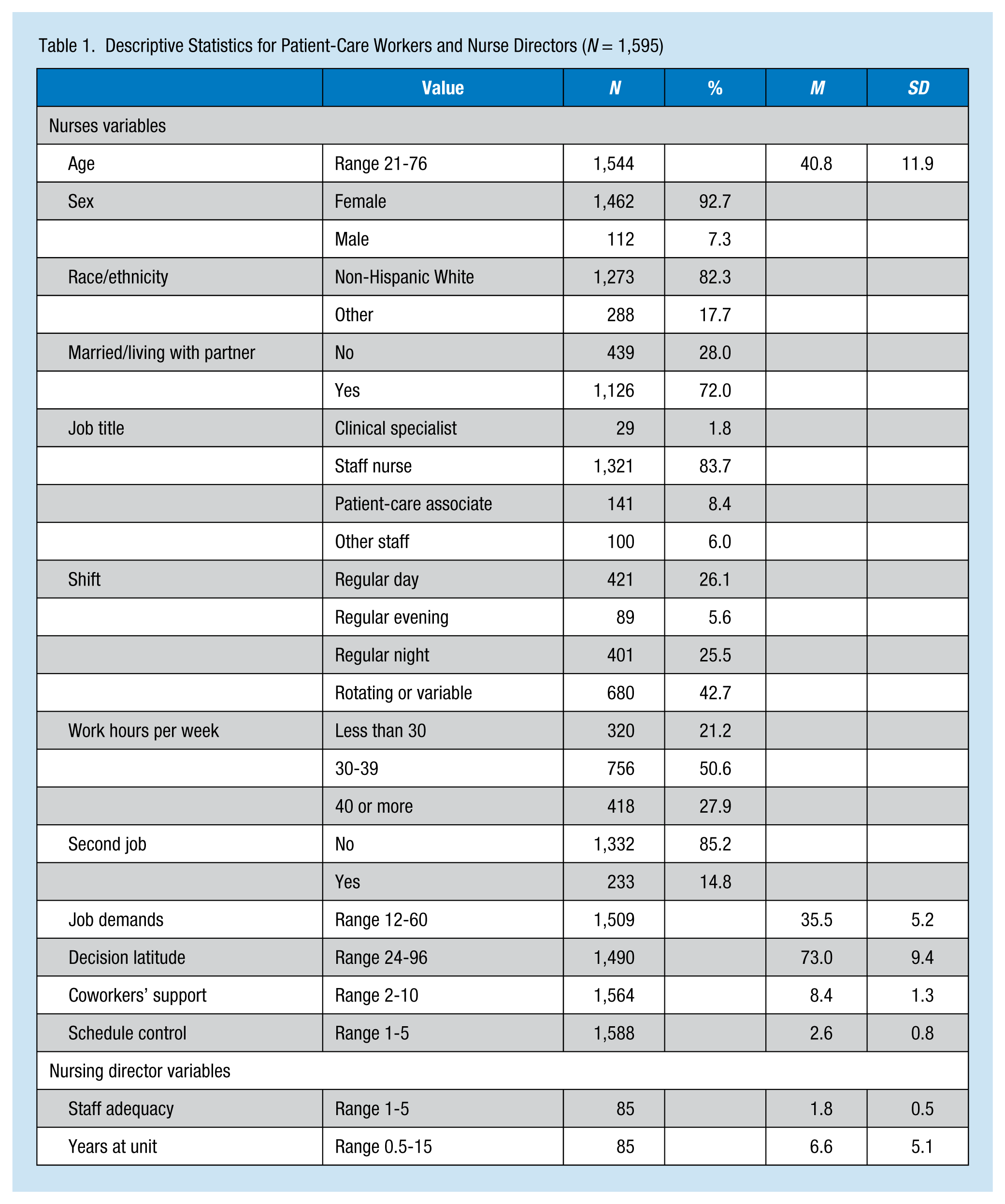
Data were collected via a cross-sectional survey administered to nurses in two Boston teaching hospitals between September 2012 and January 2013. A random sample of eligible workers (n = 2,000) was invited to complete the survey. Eligible workers included all registered nurses (RNs), licensed practical nurses (LPNs), and patient-care associates (PCAs), employed for 20 hr or more per week. Excluded participants were other health care professionals (e.g., physical therapy, occupational therapy), administrative staff, workers on extended leave more than 12 weeks, and traveling or contract/per diem nurses. Participants were included in the dataset if they completed at least half of the online survey, for a response rate of 79.5% (n = 1,595). Patient-care staff works in units or groups supervised by a nursing director. On each unit, the most senior manager, responsible for policy and procedure decision making, was selected to be the unit manager. A total of 87 managers were asked to complete the survey, and of those, 79 completed at least 50% of the questionnaire, for a response rate of 90.6%. Table 1 includes the sample size for each variable, where only one variable (decision latitude) exceeded more than 5% of missing data (n = 105, 6.5%). Appropriate Institutional Review Boards approved the study.
Descriptive Statistics for Patient-Care Workers and Nurse Directors (N = 1,595)
Measures
Psychological distress
This construct was measured with the K6 questionnaire (Kessler et al., 2010), which has six items measuring the frequency of anxiety and depression symptoms during the last 30 days. A descriptive summary score was created, adding items’ responses so that higher scores indicated more psychological distress (range = 0-24). The K6 had adequate internal consistency for this sample, with a Cronbach’s alpha of .80. Per recommendation of the K6 developers, descriptive scores were complemented with item-response theory (IRT) calibration. IRT scores were used for hypothesis testing. IRT individual analytical scores were calculated using a two-parameter logistic model, which yielded a continuous score for intensity of depression and anxiety symptoms. The individual IRT scores quantified the standardized difference for each individual from the center of the K6 distribution (i.e., the point upon which higher scores are more indicative of potential clinical cases).
Meal break frequency
The researchers developed a questionnaire to measure meal break practices based on formative qualitative research. Frequency of nurses’ meal breaks was measured with the following question: “How often are you able to take your full meal break?” A full meal break was defined as taking at least 30 min to eat a meal, as established in the state’s labor code. This question was coded using a 5-point Likert-type scale from 1 (never) to 5 (always).
Supervisor support
Specific support for meal breaks was determined by asking nursing directors to respond to the following statement: “Staff is supported in leaving the unit for meal breaks.” Responses were coded on a 5-point Likert-type scale from 1 (strongly disagree) to 5 (strongly agree). The researchers also controlled for supervisors’ general support, which was measured by three questions extracted from the Job Content Questionnaire (JCQ; Karasek et al., 1998), asking nurses if they considered their supervisor to be helpful in completing their job duties (i.e., “If needed, I can get support and help with my work from my immediate supervisor”). This supervisor support scale had a Cronbach’s alpha of .87.
Control Variables
Worker-level sociodemographic potential confounders included (a) age, (b) sex, (c) race/ethnicity, and (d) marital status. Potential occupational confounders included (e) job title (i.e., RN, PCA, or other nursing support staff), (f) hours worked per week, (g) regular shift (regular day, regular evening, regular night, rotating shifts), and (h) second job status. The researchers used an abbreviated version of the JCQ (Karasek et al., 1998) to control for psychosocial work environment variables such as (i) job demands (i.e., “My job requires working very hard”), (j) decision latitude (i.e., “My job allows me to make a lot of decisions on my own”), and (k) coworkers’ support at work, with three questions about nurses’ perception of colleagues’ help. The researchers also controlled for (l) schedule control, measured with a six-item questionnaire about workers’ perceived control over their work hours (e.g., “I can decide when to take a few hours off”) coded using a 5-point Likert-type scale from 1 “very little” to 5 “very much” (Thomas & Ganster, 1995).
In addition, the researchers controlled for nursing directors’ reports, including (m) years as unit managers and (n) staff inadequacy measured by the Nursing Work Index–Revised Questionnaire (Aiken & Patrician, 2000), a 4-item scale (i.e., “In the last year on your unit, how often have there been enough registered nurses to provide necessary patient care?”) commonly used to determine whether nursing personnel are sufficient to provide patient care. Items were coded using a 5-point Likert-type scale, from 1 “never” to 5 “always.”
Analyses
The authors first described the data and conducted bivariate analyses with the variables of interest. Hypotheses were tested with multilevel modeling because predictors were collected at two levels (individual and supervisor), and also because nurses were nested in units. The association of supervisors’ specific support for meal breaks (Hypothesis 1) was tested with a random intercept model adjusting for control variables, including general supervisor support. The association of nurses’ meal break frequency with psychological distress (Hypothesis 2) was also tested with a random intercept model, adjusting for supervisors’ support and control variables. This model was extended including multiplicative interactive terms between supervisors’ specific support and nurses’ meal break frequency (Hypothesis 3). The researchers standardized continuous measures to ease the interpretation of the coefficients. IRT calibration was performed with MPLUS v. 4.2; all other analyses were conducted with SAS 9.3.
Results
Description of the Sample
The majority of the sample was non-Hispanic White women, with an average age of 40 years (Table 1). Most workers were married or living with a partner. Most workers were RNs (83.3%), working day or rotating shifts, 30 hr or more per week. About one in seven workers had second jobs. Job demands, decision latitude, coworkers’ social support, and schedule control had averages around or higher than the midpoint of their possible values. Most supervisors (80%) reported too few RNs to provide necessary patient care.
Predictors of Meal Breaks
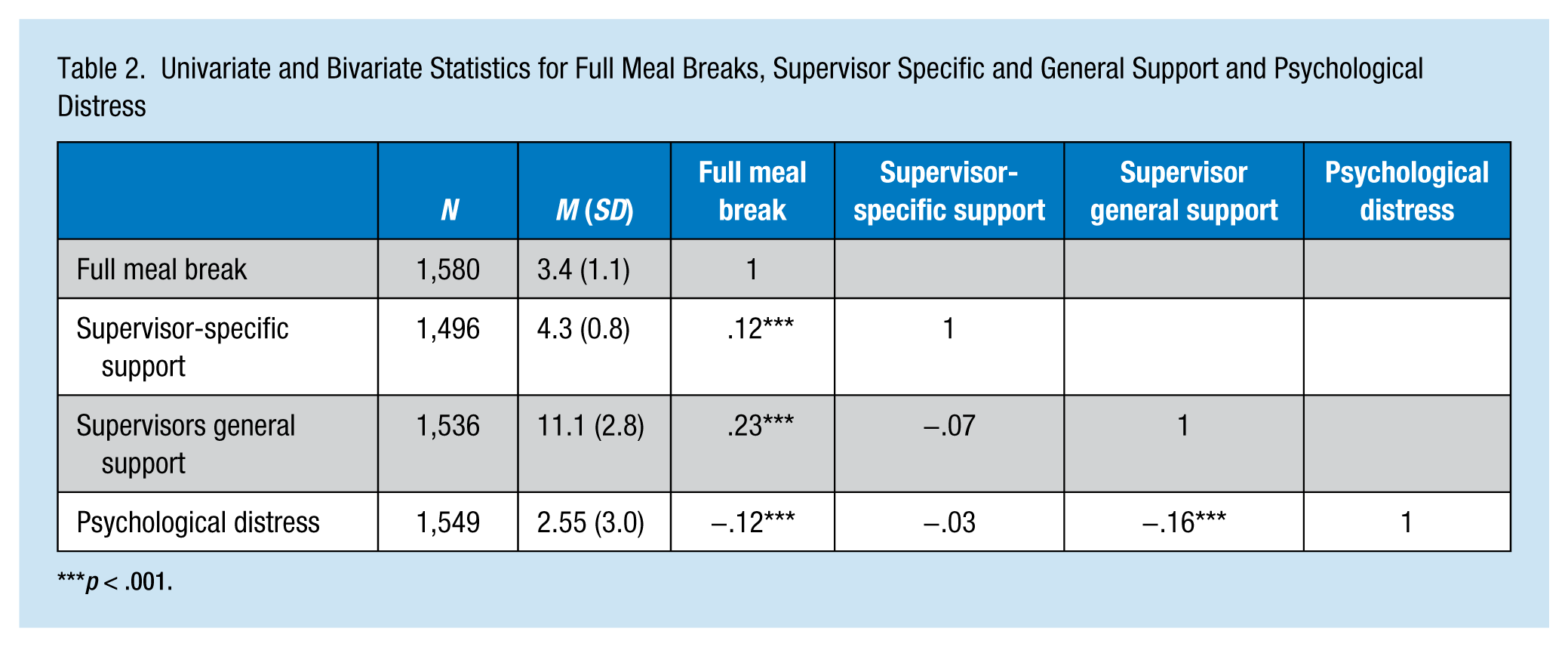
On a 5-point scale from 1 (never) to 5 (always), average nurses’ meal break frequency was 3.4. Supervisors reported that they supported staff members in leaving their units for meal breaks, with a mean score of 4.3 on a 5-point scale. Nurses’ perceived general supervisor support had a mean score of 11 (maximum = 15). Supervisors’ specific and general support were not correlated; however, these two variables were weakly correlated with nurses’ meal break frequency (Table 2).
Univariate and Bivariate Statistics for Full Meal Breaks, Supervisor Specific and General Support and Psychological Distress
p < .001.
The frequency of nurses’ meal breaks varied significantly across units; 17% of the variance was attributable to unit clustering (intraclass correlation = .17). After adjusting for control variables (Table 3), meal break frequency was positively associated with supervisors’ specific break support. However, no statistically significant differences in the magnitude of the effects of general or specific support were found.
Predictors of Full Meal Breaks and Psychological Distress (z Scores)
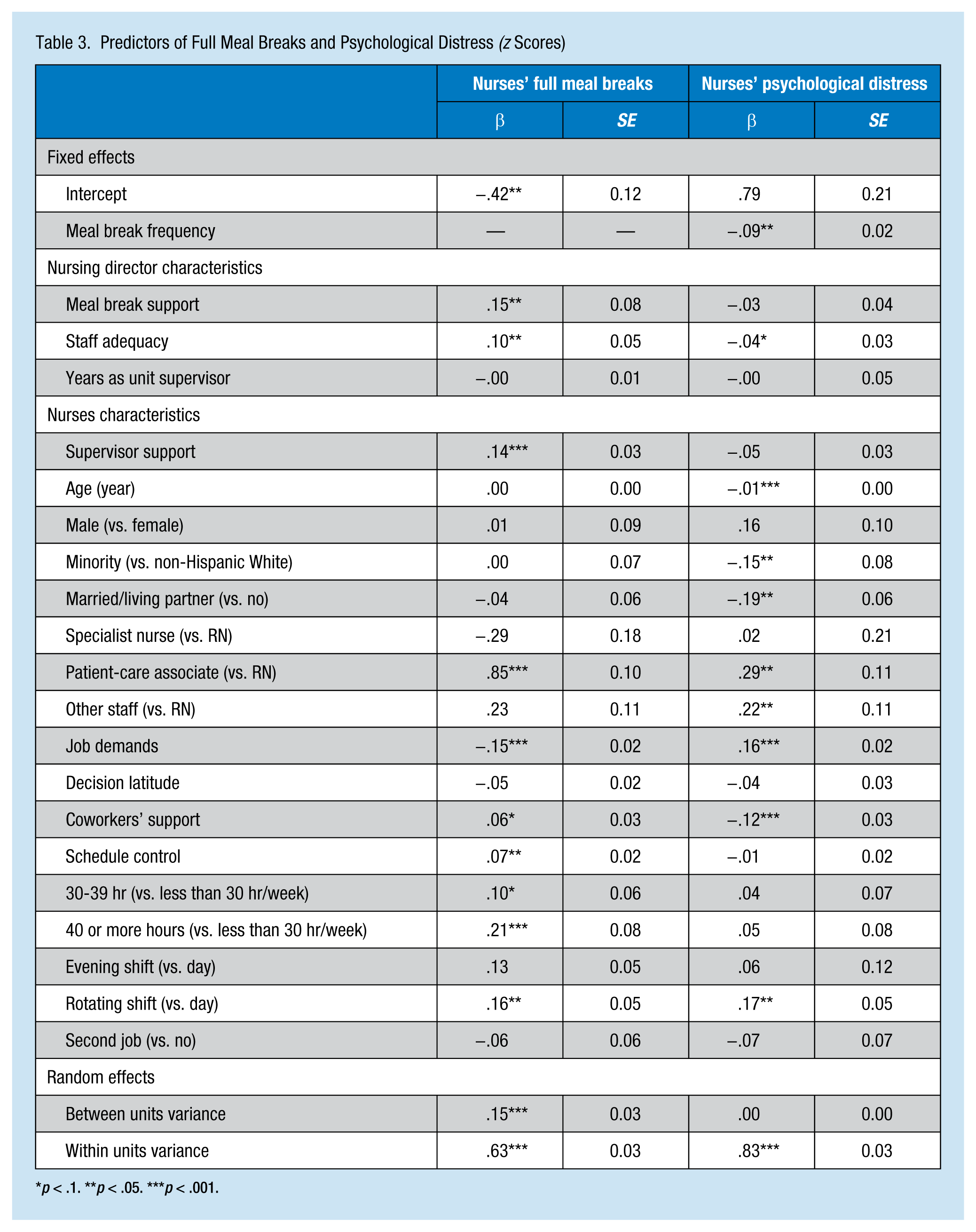
p < .1. **p < .05. ***p < .001.
The authors also found several differences in meal break frequency by occupational characteristics. Compared with RNs, PCAs reported higher frequency of meal breaks. Nurses working more than 30 hr per week reported more meal break frequency than those working less than 30 hr. Nurses working rotating shifts also averaged more meal break frequency than those working regular day shifts. Higher job demands were negatively linked to fewer meal breaks, and higher schedule control and social support from coworkers were positively associated with more meal breaks. Finally, staff adequacy was also significantly correlated with higher frequency of meal breaks.
Associations With Psychological Distress
About a third of the sample did not report any psychological distress symptoms; the K6 median score was 2.0 of a possible 24 points. Correlations showed that nurses’ meal break frequency was associated with psychological distress (Table 2). After adjusting for characteristics of both nurses and their nursing directors, the association between nurses’ meal break frequency and psychological distress was statistically significant. Nevertheless, the magnitude of the correlation was attenuated to about a quarter of the unadjusted association. Neither specific nor general supervisor support for nurses’ breaks was significantly associated with psychological distress, after adjusting for nurses’ meal break frequency and control variables. The interaction effect among psychological distress, nurses’ meal break frequency, and specific supervisor support was not statistically significant (β = .004).
Discussion
The aims of this study were to test whether meal break frequency was influenced by specific supervisors’ support, and then to examine whether meal break frequency was associated with lower psychological distress. Adjusted analyses showed that nurses’ meal break frequency was higher if their supervisors supported this practice. Moreover, increments in the frequency of meal breaks were associated with lower psychological distress.
Although psychological distress was low in this sample of patient care workers (i.e., about a third of nurses reported no distress symptoms during the last 30 days), this risk factor for mental illness (i.e., one of the main causes of work-related disability worldwide) was associated with the frequency of meal breaks. Nursing studies have described meal breaks as short, rushed, and taken in non-private or loud places (Witkoski & Dickson, 2010). Despite these adverse characteristics, enhancing opportunities for meal breaks should be a daily strategy to promote nurses’ mental health. This finding is consistent with other evidence concluding that organizational arrangements that increase workers’ control of their work time could foster better mental health (Grzywacz & Bass, 2003). Meal breaks could positively affect mental health via various pathways, including day-to-day opportunities to recover from fatigue, a pause from patient-care work, socializing with coworkers, and enjoying meals (LaMontagne, Keegel, & Vallance, 2007; Rajaratnam & Arendt, 2001).
From both conceptual and analytical standpoints, the authors considered it critical to analyze organizational factors such as supervisor support that could explain why some workers take more or less breaks. Study findings are partially consistent with other studies concluding that supervisors’ support for specific behaviors could indeed facilitate workers engaging in such behaviors, with more predictive power than general support (Kossek et al., 2011). However, the researchers found no significant difference in the magnitude of the relationship between specific and general support, though both types of support were independent predictors of higher workers’ meal break frequency.
Even though both workers and nursing directors reported high supervisor support, nurses’ reports of meal break frequency were not strongly correlated with supervisors’ reports of support for meal breaks or general support. This discrepancy has been found in other studies about psychosocial and physical work hazards (Carson, Carson, Yallapragada, & Roe, 1998; Winnemuller, Spielholz, Daniell, & Kaufman, 2004); researchers have argued that supervisors overestimate their support, which could explain the low correlation between nurses’ meal break frequency and specific supervisor support.
Study Limitations
The retrospective and self-reported nature of the study measures cannot exclude non-differential misclassification and measurement errors of exposure and outcome. Measures of meal break frequency as well as some control variables such as marital status might not have been entirely sensitive to identifying the precise pathways by which managers could exert influence on workers’ mental health. This imprecision, however, could have biased the estimates downward toward non-association, but the point estimates were still statistically significant. The cross-sectional design and the weak correlation between supervisors’ support and meal break frequency prevented the researchers from testing potential mediational effects of manager’s practices on individual behavior through unit-level changes. Longitudinal studies are needed to test if managers affect individuals’ health directly or mediated through workers’ behaviors.
In addition, the attenuation of the adjusted versus the unadjusted association suggests the presence of residual confounding. Acknowledging the potential influence of unmeasured individual factors such as preferences or needs regarding meal breaks, future studies should rely on designs and analyses that support causal inference. Study data were also limited in identifying environmental factors that influence meal breaks. Studies have documented that suboptimal break room conditions (e.g., appearance, privacy, temperature) might make it less suitable for workers to take breaks, whereas workplace interventions that improve the appearance of break rooms may increase the frequency of breaks (Shields & Wilkins, 2006). Further research should account for physical factors as well as individual preferences to determine pathways connecting work breaks with health outcomes.
This study also had several strengths that positively affect the external and internal validity of the findings. The random representative sample of more than 1,500 workers with a response rate of 79% supports the generalizability of the findings, which could be relevant to other health care institutions. The assessment of several manager- and worker-level characteristics illustrates the relevance of measuring multiple features of actors in the work environment.
Practice Implications and Conclusions
Nurses who took more frequent meal breaks averaged lower psychological distress, and meal breaks were facilitated by specific supervisor support. These relevant findings could inform interventions aimed at improving workers’ mental health, as it demonstrates that specific encouragement has more effect on eliciting intended behaviors, which, in turn, could be related to better health. Integrated interventions should target psychosocial factors such as supervisory support and management styles in conjunction with individual characteristics. Meal breaks should provide daily opportunities for fatigue recovery; for access to healthier, more enjoyable meals; to enjoy meals and leisure or personal time, factors that explain the positive effect of meal breaks on mental health. Organizational policies and practices that support and enforce meal breaks could be relevant strategies for promoting workers’ mental health and well-being.
Applying Research to Practice
Meal breaks are daily opportunities for recovery from fatigue, to facilitate access to healthier meals, to enjoy meals, to have leisure moments or personal downtime. These factors might explain the positive effect on mental health.
Footnotes
Acknowledgements
The authors would like to thank Partners Occupational Health Services, including Marlene Freeley, for their guidance, as well as Karen Hopcia, Elizabeth Taylor, Elizabeth Tucker O’Day, and Terry Orechia. They also thank individuals at each of the hospitals including Jeanette Ives Erickson and Jacqueline Somerville in Patient-Care Services leadership, and Jeff Davis and Julie Celano in Human Resources. In addition, they wish to thank Charlene Feilteau, Mimi O’Connor, Margaret Shaw, Eddie Tan, and Shari Weingarten for their assistance with supporting databases. They also thank Chris Kenwood of New England Research Institute for his statistical and programming support, and Julie Theron, project director, and Linnea Benson-Whelan for their assistance with the production of this manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Institute for Occupational Safety and Health (U19 OH008861) for the Harvard School of Public Health Center for Work, Health, and Well-Being.
Author Biographies
David A. Hurtado, ScD, is a Yerby Postoctoral Research Fellow at the Center for Work, Health and Well-being at the Harvard T.H. Chan School of Public Health. Dr. Hurtado investigates how time arrangements at work impact workers’ heath and well-being.
Candace C. Nelson, ScD, was the Harvard-Liberty Mutual Post-Doctoral Fellow at the Harvard T.H. Chan School of Public Health, Department of Environmental Health.
Dean Hashimoto is the Chief of Occupational and Environmental Medicine, Occupational Health Services, Partners HealthCare System. His research focuses on the impact of regulatory and business systems on the healthcare delivery.
Glorian Sorensen is Professor of Social and Behavioral Sciences at the Harvard T.H. Chan School of Public Health, and Faculty Vice President for Faculty Development at the Dana-Farber Cancer Institute, where she also directs the Center for Community-Based Research. The core of Dr. Sorensen’s cancer prevention research is randomized worksite- and community-based studies that test the effectiveness of theory-driven interventions targeting individual and organizational change.