
Abstract
A 52-year-old female working as a registered nurse in the ICU developed tremors with fine motor activities in stressful situations. She was evaluated by a neurologist and was diagnosed with physiological tremors. Implications for practice are explored.
AG, a 52-year-old female, practiced as a registered nurse in the intensive care unit at night. During a code, AG was attempting to place an arterial line, but developed tremors. Another nurse was assigned to place the arterial line. AG stated that she started to develop the “shakes” in her early 30s while working as a surgical technician in ENT (ear, nose, and throat) surgery. She was attempting to grab small ear tubes with a long forceps when her right dominant hand developed a tremor. AG felt that she was “pressured” by the surgeon to quickly hand him the tubes. She developed tremors and accompanying symptoms, such as tachycardia and diaphoresis, in other stressful situations, such as flying. Accompanying symptoms that she reported were an increased heart rate and perspiration. Once the airplane flew into heavy turbulence, her right hand shook uncontrollably. AG also reported that when she attempted fine motor activities during stressful situations, she developed tremors. She stated that at times she had difficulty holding her cell phone due to tremors; this happened when a family member called her with bad news. A physician recommended that AG be evaluated for possible essential tremors.
During the assessment, AG denied any medical or surgical concerns. She reported taking an ibuprofen on occasion for non-specific musculoskeletal pain. She denied having any allergies and did not recall any family history of neurological disorders. She denied resting tremors, gait disturbances, bradykinesias, rigidity, or micrographia. She denied any history of alcohol or illegal drug use or exposures to environmental toxins.
During her neurological examination, cranial nerves 2 to 12 were grossly intact. Muscle tone was adequate with sensory and motor function intact. The sensory examination included nerve testing for pressure and touch using vibration and pinprick, and the motor examination tested for skeletal muscle strength and tone. Gait was normal, and assessment of the cerebellum revealed no abnormalities. An MRI eliminated multiple sclerosis or other neurodegenerative disorders as diagnoses. A thyroid panel as well as a complete blood count (CBC) and complete metabolic panel (CMP) revealed no abnormalities.
Tremors
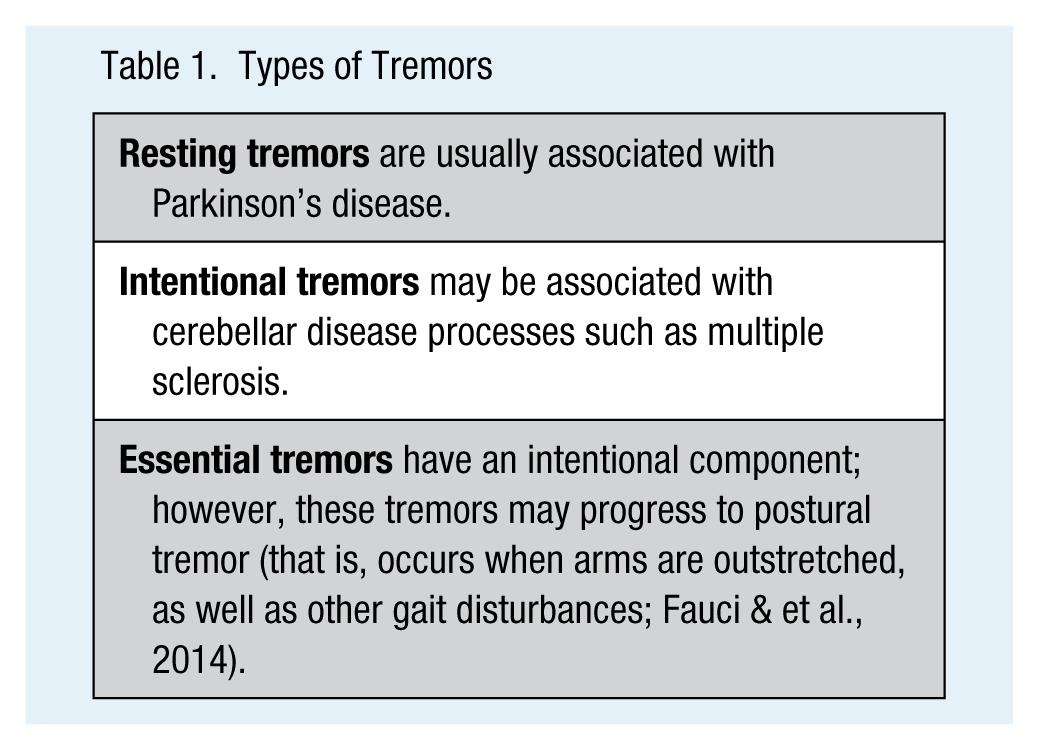
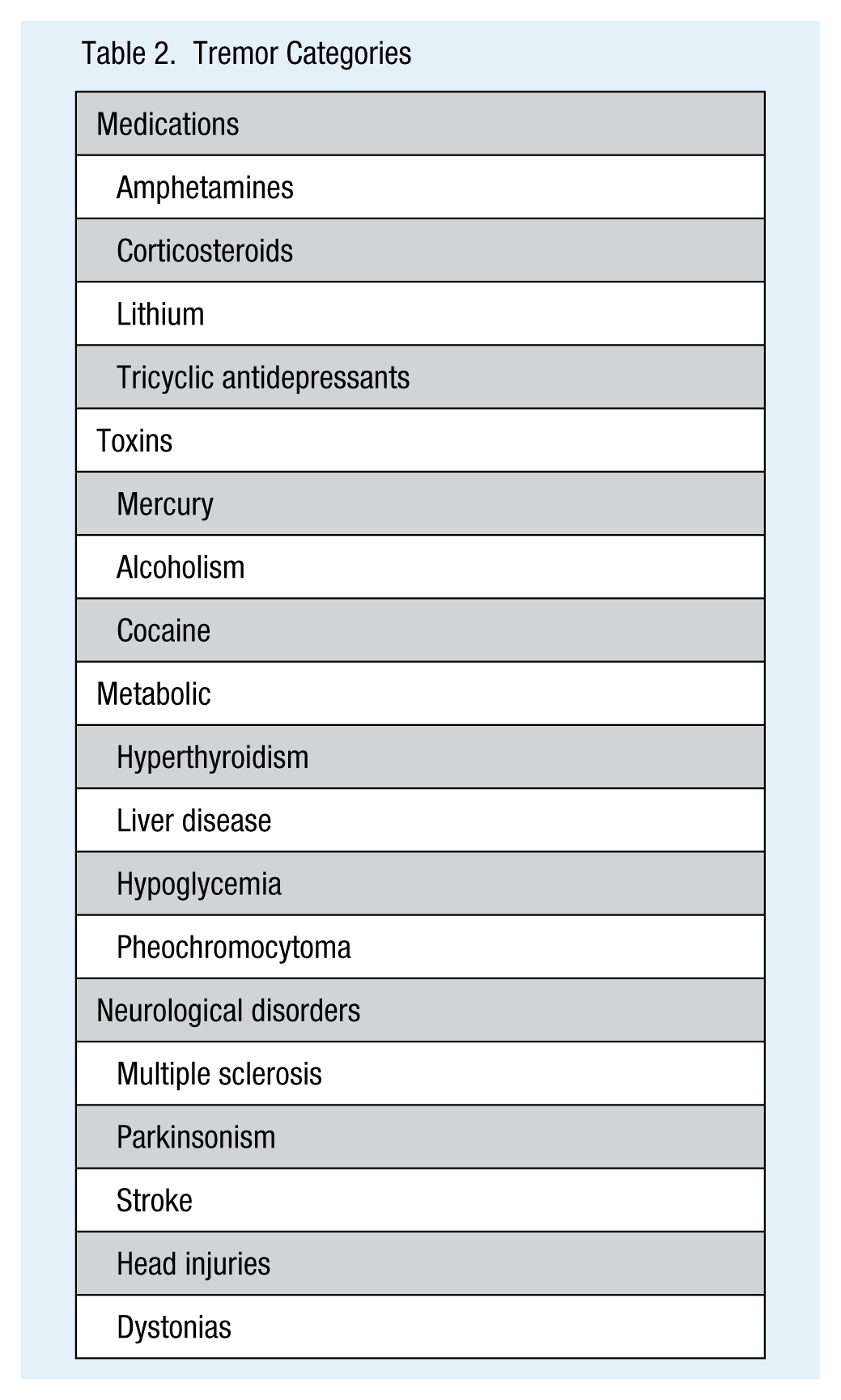
Tremors are a hyperkinetic disorder (see Table 1). A tremor is a high frequency (i.e., 4 to 12 hertz depending on type of tremor) involuntary oscillation of a body limb, usually in a rhythmic, regular, and repetitive pattern (Bruno et al., 2012). The differential diagnosis of tremors is critical to provide appropriate treatment and workplace accommodations. The exact pathology may not be understood; however, generally it is believed that tremors result from lesions in the ventrolateral nucleus of the thalamus (Goroll & Mulley, 2014). Tremors can also be associated with diseases of the cerebellum or extrapyramid areas as in the case of stroke, Parkinson’s disease, or multiple sclerosis (Fauci et al., 2012; see Table 2).
Types of Tremors
Tremor Categories
Evaluation of tremors consists of a history, physical examination, and radiography such as MRI of the brain. The history includes medications and exposure to toxins, metabolic disorders, or any other neurological disorders (Rajput & Rajput, 2014). Tremors with ataxia or other abnormal cerebellar findings (e.g., finger to nose test) should be investigated further (Rajput & Rajput, 2014). In addition, gait instability, rigidity, and bradykinesia could indicate Parkinson’s disease (Rajput & Rajput, 2014). Tremors that improve with rest and present as sustained involuntary muscle contractions may indicate a dystonia (Louis, 2014). The physical examination includes a full neurological examination to evaluate if the tremor worsens with activity. Additional testing may involve asking the client to hold both hands outstretched for a minute or write a sentence. An electromyography (EMG) may be used to specify the type of tremor, as well as a thyroid panel, CBC, and CMP to eliminate liver or renal disease from consideration (Goroll & Mulley, 2014).
Essential Tremors
Essential tremors, considered intentional or action tremors, are a common neurological disorder of involuntary movement that affects mainly the upper limbs (Sullivan, Hauser, & Zesiewicz, 2004). These tremors present when hands are outstretched and are least likely to present when the arms are at rest. Essential tremors may worsen with fine motor activity but need not be associated with purposeful movement (Louis, 2014). These tremors occur when in a postural or kinetic position and are usually bilateral and symmetric (Bruno & et al., 2012). Essential tremors usually start in one upper limb and then progress to both limbs and even the head. The frequency of these tremors can range from 8 to 12 Hz, the frequency increasing with age.
Essential tremors are a progressive disorder that may begin in childhood; the prevalence increases with age. An estimated 5 to 10 million individuals in the United States suffer from this disorder (Fauci et al., 2012). The disease appears to have a genetic component, an autosomal dominant pattern linked to loci on chromosome 3q13 and 2p22-25 (Fauci et al., 2012). Intentional tremors are present during purposeful movement toward a target and are tested during the finger to nose examination in a neurological examination. The neurological examination may be normal; however, upon finger to nose testing, an intentional tremor may appear (Fauci et al., 2012).
Essential tremors are believed to be caused by a deficiency of gamma-aminobutyric acid (GABA) at the alpha 1-subunit and treatment includes medications such as anticonvulsants that impact GABAergic neurotransmission (Bruno et al., 2012). These tremors also may be treated with medications such as beta-blockers or anti-seizure medications; however, primidone is a first-line medication (Sullivan et al., 2004). In addition, essential tremors may respond to benzodiazepines as well (Goroll & Mulley, 2014). Workplace accommodations may include using weighted instruments; however, due to the progressive nature of the tremors, workers may become permanently disabled.
Physiological Tremors
Physiologic or postural tremors are usually associated with stressful situations or physical exhaustion (Goroll & Mulley, 2014). These tremors range from 8 to 10 Hz and may occur during movement. No genotype has been identified. This type of tremor is usually not associated with any neurological disorder; however, these tremors may be a symptom of metabolic disorders or exposure to toxins (Fauci et al., 2012). These tremors are a consequence of over stimulation of the beta-adrenergic receptors by elevated levels of catecholamines (Fauci et al., 2012). Physiological tremors may occur in anyone; therefore, family history is not necessary (Rajput & Rajput, 2014). No treatment is generally recommended; however, some patients find that taking benzodiazepines during stressful situations may relieve symptoms (Fauci et al., 2012).
Implications for Practice
Occupational health nurses must understand the etiology and diagnosis of tremor because some forms of tremor may be related to underlying pathology. Employees with tremors may require medications and workplace accommodation with weighted instruments such as with writing equipment. The goal is to diminish the tremor so the employee can continue working and avoid disability. Fine motor activities may be affected; an occupational therapy consult may be warranted.
Conclusion
Based on the history, a normal physical examination, and a normal diagnostic screening, AG was diagnosed with physiological tremors that required no treatment. However, she transferred to same day surgery which she found to be “less stressful.” Rest was recommended, and she found that working dayshift provided her with an adequate sleep cycle.
Footnotes
Acknowledgements
The author thanks Hera Stephens, MD, Candace Burns, ARNP, PhD, and Barb Maxwell, RN, MHA, COHN-S.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann Lurati is an occupational health nurse practitioner in Tampa, Florida, specializing in toxicology and risk assessment.