
Abstract
Background
Valued living is the extent to which an individual’s behavior is consistent with what they believe is important or good. It is unknown whether many complementary and integrative treatments and psychotherapies for posttraumatic stress disorder enhance valued living, and for whom.
Objectives
Measure within- and between-group changes in valued living in Veterans who completed cognitive processing therapy (CPT) and sudarshan kriya yoga (SKY) for posttraumatic stress disorder (PTSD); evaluate moderators of improvement.
Methods
Participants with clinically significant symptoms of PTSD were assigned to CPT, a first line, evidence-based psychotherapy for PTSD or SKY, an emerging breath-based meditation with strong preliminary empirical support in a parallel-groups randomized controlled trial at a single Veterans Affairs healthcare center. The Valuing Questionnaire subscales for progress in valued living (VQ-P) and obstruction in valued living (VQ-O) were exploratory outcome measures. Assessors were blind to treatment assignment.
Results
59 participants completed treatment (29 CPT, 30 SKY). Participants in the CPT group improved from baseline to end of treatment in both VQ-Progress (d=0.55, p=0.02) and VQ–Obstruction (d=-0.51, p=0.03), while the SKY group did not improve on either subscale (d=0.08, p=0.69; d=0.00, p=1.00). However, differences between treatments were not statistically significant (p=0.16, 0.11, respectively). Participants reporting less valued living and more depression symptoms at baseline reported greater improvements in valued living following treatment.
Conclusion
CPT may have a positive effect on valued living. Individuals lower in valued living and with more depression may derive relatively more benefit.
Keywords
Background
Treatments for posttraumatic stress disorder (PTSD) are generally vetted for their efficacy in ameliorating symptoms (e.g.,1,2), with less emphasis on improving functioning.3,4 However, even functional outcomes are generally researcher-defined and may not reflect what individuals believe to be the most important treatment outcome. Indeed, it has been argued that treatments’ focus on symptoms may inadvertently shift individuals’ focus away from what they believe to be most important in life. 5 Accordingly, an alternative construct, valued living, has been proposed as a transdiagnostic treatment goal 6 and therefore an important measure of treatment outcome.
Valued living is defined as engaging in behaviors that an individual believes to be worthy or meaningful (for a technical definition, see 6 ). For example, a parent who values being loving may supervise a child’s education in a patient and attentive way; an individual who values financial security may create a budget. Valued living is correlated with positive constructs such as satisfaction with life and psychological wellbeing. 7 Numerous studies have documented that acceptance and commitment therapy (ACT), which sets enhancing valued living as its primary goal, is effective in improving valued living, though confidence in these findings is somewhat limited by methodological concerns e.g., no control group and/or outcome measure with suboptimal psychometric properties. 8
Little is known about whether treatments other than ACT affect valued living. One study among adults with social anxiety disorder found that cognitive behavioral therapy (CBT) improved valued living more than a waitlist control. 9 Similarly, an analysis of a large clinical sample of outpatients diagnosed primarily with anxiety and depression who were treated with CBT demonstrated an increase in valued living. 10 In contrast, a trial among teenagers with anxiety revealed no change in valued living following CBT. 11 However, it is unknown if PTSD treatments improve valued living. The question may be especially relevant, as the condition is associated with a generalized avoidant coping style that may restrict valued living.12-14
Complementary and integrative health (CIH) interventions, such as mindfulness-based interventions and movement based interventions such as yoga, place less emphasis on “treatment” of specific health conditions and are often considered to enhance “wellness”. 15 However, research has documented many positive effects of CIH practices on PTSD and other outcomes.16-19 Little is known about whether complementary and integrative approaches facilitate valued living. A study of treatments for social anxiety disorder indicated participants in the mindfulness skills group improved in valued living more than participants on a waitlist. 9
Further, little is known about who is likely to improve in valued living during treatment. One study of panic disorder treatment found that those with higher baseline panic symptoms improved more in valued living during treatment. 20 Further identifying who may benefit from treatment may inform treatment selection and treatment development.
A central tenet of ACT is that treatment may improve valued living directly; that it is not necessary for symptoms to remit before progress in valued living may occur. 21 However, little is known about the processes by which valued living may be enhanced by other treatments. For example, a decrease in symptoms could potentiate an increase in valued living, or an improvement in valued living could help improve symptoms. In either of these scenarios, improvement in valued living would be correlated with improvement in symptoms. Alternatively, improvement in valued living and improvement in symptoms may result from independent processes, and as a result be empirically uncorrelated.
The Present Study
We measured valued living as an exploratory outcome in a randomized controlled trial comparing a breath-focused meditation practice, Sudarshan Kriya Yoga (SKY), 22 to an evidence-based psychotherapy, cognitive processing therapy (CPT). 23 Participants were Veterans with symptoms of PTSD. We explored: (1) Whether progress in valued living and obstruction of valued living would improve during PTSD treatment, (2) whether SKY and CPT would be differentially effective in facilitating valued living, (3) whether treatment outcome would vary by demographic and clinical characteristics, and (4) whether improvement in valued living would be related to improvement in PTSD symptoms.
Methods
Participants and Procedure
The trial protocol has been described in detail previously. 22 Briefly, participants volunteered for a single-blind randomized clinical trial of two parallel treatments for PTSD among Veterans. The study was conducted at the War Related Illness and Injury Study Center at the Veterans Affairs Palo Alto Health Care System. Eligibility was assessed via telephone and in person. Inclusion criteria were: (i) Veteran of the U.S. military; and (ii) clinically significant symptoms of PTSD as indicated by a score of ≥38 on the PTSD Checklist Version 5. 24 Exclusion criteria were: (i) concurrent participation in another treatment study; (ii) intention to begin a new trauma-focused therapy during the study period; (iii) mania or psychosis for any reason within the past 6-months; (iv) suicidal or homicidal intent within the past 60 days; (v) substance dependence (other than nicotine) within the past 30 days; (vi) unmanaged seizure disorder; (vii) severe traumatic brain injury; (viii) or initiation of psychotropic medication less than 8 weeks prior to screening.
Eligible participants were randomly assigned to a treatment group in a 1:1 ratio by blindly drawing a sealed envelope from a box created by the study coordinator. In the event that a cohort had an odd number of participants, the study coordinator alternated which treatment the extra envelope contained. Participants completed self-report outcome measures at baseline, which occurred ≤1 week prior to the first treatment session, and end of treatment, which occurred ≤1 week after the final treatment session. Assessors were blinded to treatment, and participants were instructed during assessments not to reveal their assigned treatment. The investigation was carried out in accordance with the latest version of the Declaration of Helsinki. Stanford University Institutional Review Board conducted ethical review and approved the protocol (#32252). Written informed consent of the participants was obtained after the nature of the procedures had been fully explained.
Interventions
Cognitive Processing Therapy
CPT is an evidence-based, trauma-focused psychotherapy. 23 We used the “cognitive only” version of CPT, which excludes the writing and reading of a formal trauma narrative. CPT was given in 12 60-min sessions twice per week for 6-weeks. This treatment emphasizes developing cognitive “restructuring” skills and applying them to challenge negative beliefs (“stuck points”) related to responsibility for the traumatic event(s) and five additional key areas (safety, trust, power/control, esteem, and intimacy). Homework was assigned following each session. All sessions were delivered by licensed or postdoctoral clinical psychologists, all of whom were certified via the VA’s CPT rollout initiative. 25
Sudarshan Kriya Yoga
SKY is a type of yogic breathing practice involving cycles of controlled breathing. It does not emphasize other “limbs”, or components, of yoga, such as physical postures, principles for living, etc. SKY was provided in a group format and all sessions were led by two experienced, certified instructors. Three controlled breathing techniques were taught: (i) three-stage victory breath (ujjayi pranayama), (ii) bellows breath (bhastrika pranayama), and (iii) SKY breath (Sudarshan kriya). We used the non-Sanskrit names to allow greater accessibility to Veterans. Sudarshan Kriya – the central component of SKY – is a cyclical breathing exercise consisting of consecutive slow, medium, and fast breath cycle rates. We used a protocol designed by Project Welcome Home Troops, a project of the International Association for Human Values,22,26 for use with Veterans which was adapted for the present study. Treatment consisted of an initial 5-days intensive group workshop (3 h per day) followed by 10, 60-min sessions given twice per week. Home practice was encouraged but not mandatory.
Measures
The primary outcome measure was the
The
The
Comorbid clinical conditions were assessed using the
Statistical Analyses
Statistical methods were defined prior to analyzing data and are reported as defined. We conducted per-protocol analyses, including only participants who completed treatment. While intent-to-treat analyses, including all participants, may be preferable for analyzing primary outcomes, we sought a direct assessment of the relationship between treatment and an exploratory outcome, uncompromised by participants who did not complete treatment. Treatment completion was defined as attending at least 70% of treatment sessions. The study was powered to test the randomized controlled trial’s primary hypothesis, that SKY would be noninferior to CPT for treating symptoms of PTSD. Both effect sizes and statistical significances are reported for these exploratory analyses with moderate sample sizes.
Outcomes
Change from pre-to posttreatment in VQ-Progress and VQ-Obstruction were first assessed via one-sample t-tests assessing whether change from baseline to end of treatment was significantly different than 0. Second, to assess whether these changes, if any, differed by treatment, we used linear regressions. The dependent variables were change in the valued living variables from baseline to end of treatment. The intercept term indicated the average change across both treatment groups, and a treatment variable indicated whether the change differed between treatments. Average change scores within treatments and differences between treatments were computed. Cohen’s d effect sizes were computed by dividing the change from pretreatment to posttreatment by the baseline standard deviation, with .2 indicating a small effect size, .5 indicating a medium effect size, and .8 indicating a large effect size. 35
Process of Change
We evaluated a process of change in valued living by assessing the relationship between change in PTSD symptoms and change in valued living. This was done using a correlation measuring the extent to which improvement in each VQ subscale (VQ-Progress and VQ–Obstruction) from baseline to end of treatment was associated with improvement in PTSD symptoms (PCL-C) from baseline to end of treatment. Conversely, this could be described as measuring the extent to which improvement in valued living is independent of improvement in PTSD symptoms.
Results
Demographics and Clinical Characteristics
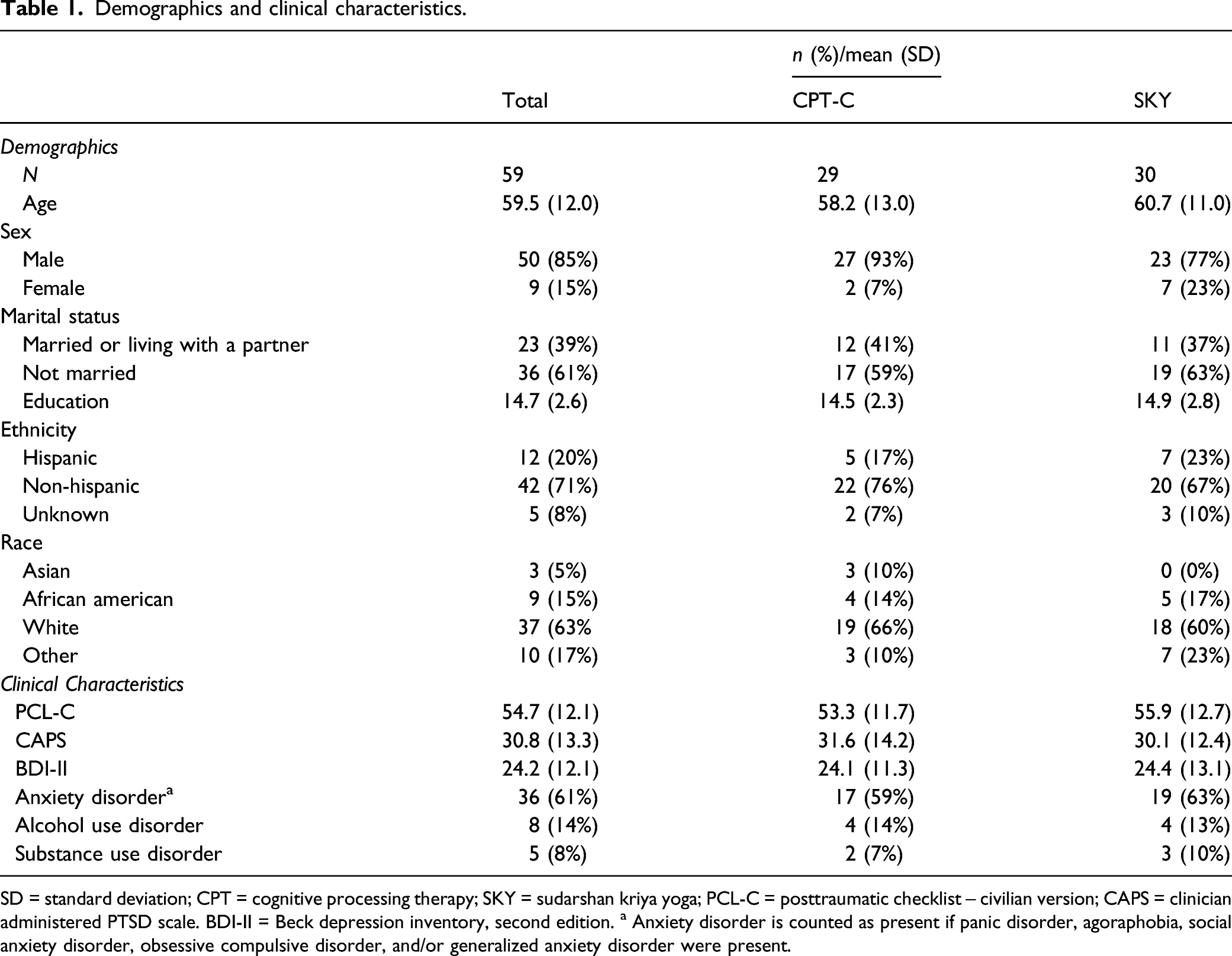
The study was conducted between October 2015 and March 2020. Eighty-five participants were randomized to a treatment (44 CPT, 41 SKY; Figure 1). Fifty-nine completed treatment (29 CPT, 66%; 30 SKY, 73%) defined as attending at least 70% of treatment sessions and were included in the analysis. The sample was predominantly male (n = 50, 85%) and White (n = 37, 63%; Table 1). Mean age was 59 years and the average PCL-C score at baseline was 54.7. CONSORT flow diagram. Demographics and clinical characteristics. SD = standard deviation; CPT = cognitive processing therapy; SKY = sudarshan kriya yoga; PCL-C = posttraumatic checklist – civilian version; CAPS = clinician administered PTSD scale. BDI-II = Beck depression inventory, second edition. a Anxiety disorder is counted as present if panic disorder, agoraphobia, social anxiety disorder, obsessive compulsive disorder, and/or generalized anxiety disorder were present.
Outcome
Change in valued living during treatment.

SD = standard deviation; CI = 95% confidence interval. a Positive baseline to end of treatment change indicates improvement. b Negative baseline to end of treatment change indicates improvement.
Within-treatment comparisons are shown in Table 2 and Figure 2. CPT completers experienced a significant increase in VQ-Progress (mean = 3.4, 95% CI [.6, 6.2], d = .55, p = .02) and a significant decrease in VQ–Obstruction (mean = -3.0, 95% CI [-5.6, -.4], d = -.51, p = .03). In contrast, participants in the SKY group did not improve in VQ-Progress (mean = .6, 95% CI [-2.2, 3.3], d = .08, p = .69) or in VQ-Obstruction (mean = 0.0, 95% CI [-2.6, 2.6], d = .00, p = 1.00). Changes in valued living during treatment. CPT = cognitive processing therapy, SKY = sudarshan kriya yoga, ns = within-group difference from baseline to end of treatment is not statistically significant; * = p < 0.05.
To assess the statistical significance of differences between treatment groups (CPT vs SKY), linear regressions were run with VQ subscales’ change scores as the dependent variable and treatment group (CPT vs SKY) as an independent variable. Differences between treatments were moderate in effect size but not statistically significant for VQ–Progress (between group d = .42, t = -1.43, p = .16) and VQ–Obstruction (between group d = -.44, t = -1.61, p = .11).
Moderation
Moderation.
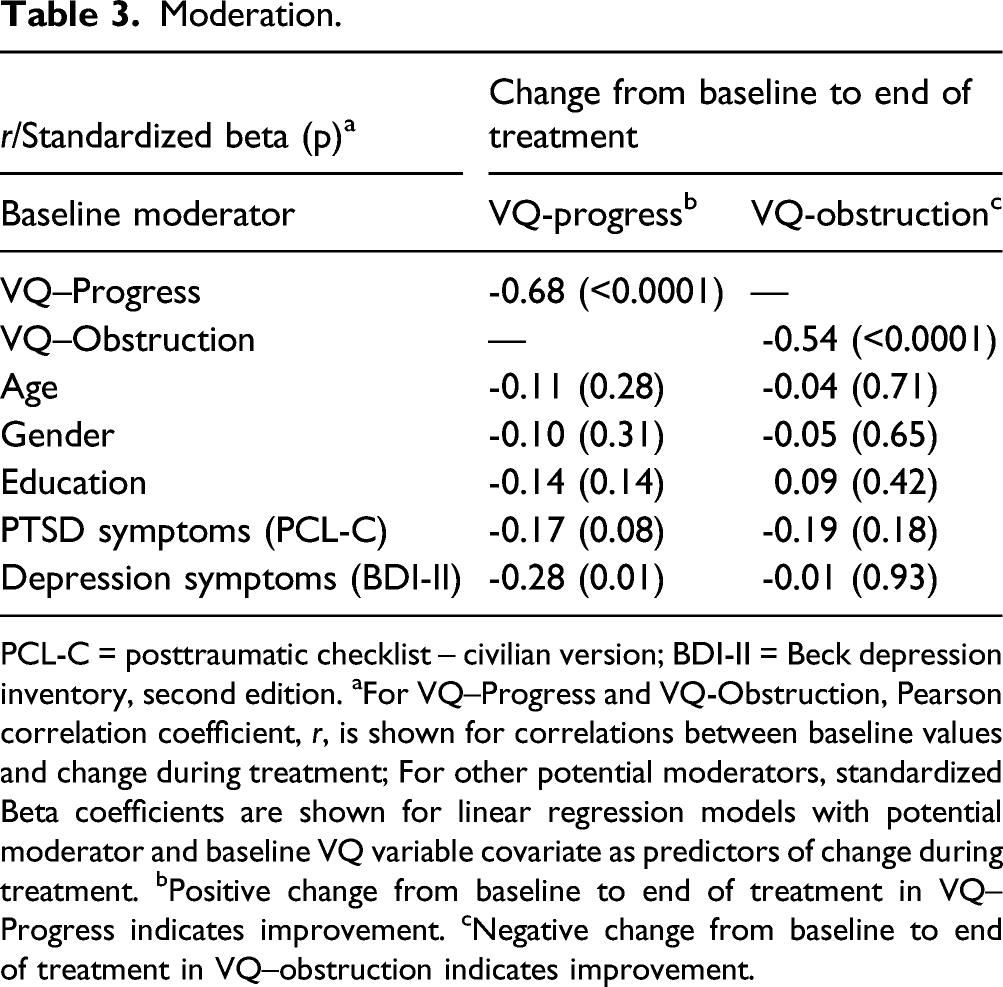
PCL-C = posttraumatic checklist – civilian version; BDI-II = Beck depression inventory, second edition. aFor VQ–Progress and VQ-Obstruction, Pearson correlation coefficient, r, is shown for correlations between baseline values and change during treatment; For other potential moderators, standardized Beta coefficients are shown for linear regression models with potential moderator and baseline VQ variable covariate as predictors of change during treatment. bPositive change from baseline to end of treatment in VQ–Progress indicates improvement. cNegative change from baseline to end of treatment in VQ–obstruction indicates improvement.
Process of Change
Both VQ-Progress and VQ-Obstruction were significantly correlated with PTSD symptoms at baseline. Greater PTSD symptom severity at baseline was moderately related to lower progress in valued living at baseline (r = -.26, p = .045) and, as would be expected, strongly related to greater baseline obstruction of valued living (r = 0.60, p = < .001). However, change in PTSD symptoms during treatment was not associated with change in VQ-Progress (r = -.15, p = .27) or VQ-Obstruction (r = .06, p = .67) during treatment.
Discussion
We explored whether Veterans tended to live more congruently with their values after completing a breath-focused meditation or a first-line psychotherapy for PTSD. Overall, participants showed a small non-statistically significant improvement in valued living following treatment. However, examining each treatment group separately revealed that on average participants in the CPT group experienced an increase in progress in valued living and decrease in obstruction of valued living, both of which were moderate in effect size and statistically significant. This suggests that CPT may improve valued living among Veterans with PTSD. However, confidence in this conclusion is attenuated by the fact that between group differences, though also moderate in effect size, were not statistically significant, perhaps due to the sample size. This extends prior research documenting positive effects of psychotherapies on researcher-defined measures of social and occupational functioning3,4 to show CPT may help individuals in psychotherapy for PTSD live according to what they believe is most important. We did not assess why individuals undergoing CPT improved in valued living, though it is possible that participants applied CPT skills to challenges that interfered with valued living. This result also adds to the nascent literature9-11 suggesting that interventions may improve valued living without targeting it directly.
This is one of the first tests of changes in valued living following a CIH intervention. In contrast to a test of a mindfulness skills intervention for social anxiety disorder, 9 valued living did not increase during SKY treatment. CIH interventions are heterogenous, consisting of a broad variety of techniques that vary in the extent to which treatments address behavior explicitly or promote a model of what “good” or valued living entails. For example, yoga in the west typically consists of physical postures and relaxation. In contrast, traditional yoga practice includes many other components, including adherence to moral imperatives such as truthfulness and the avoidance of harming others. 36 Therefore, further research is indicated to determine which components of yoga and other CIH interventions may improve valued living.
We found valued living improved more during treatment among individuals with relatively lower baseline levels of valued living. This is consistent with a trial of ACT for treatment-resistant panic disorder among adults which showed greater improvement in valued living among those with more severe panic symptoms at pretreatment. 20 These results may suggest that individuals who perceive their behavior to be particularly discrepant from their values may be good candidates for treatment. Alternatively, it may reflect regression to the mean, or a ceiling effect in which those with more space to improve on a scale may do so. Tests of moderation by other baseline variables controlled for pretreatment valued living to rule out a ceiling effect. Among other candidates, only depression moderated outcomes, with greater depression at baseline being associated with more improvement in valued living during treatment.
Valued living and PTSD symptoms were correlated at baseline, suggesting that these constructs are related. However, improvement in valued living during treatment was not significantly related to improvement in PTSD symptoms during treatment. This suggests that improvement in symptoms may be neither necessary nor sufficient to improve valued living. That is, individuals may not need to ameliorate symptoms before enhancing valued living, and, conversely, reducing symptoms may not necessarily enhance valued living. Future research with larger sample sizes may examine whether changes in valued living differ by symptom outcome grouping (e.g. remitted, improved, no change, deteriorated).
Strengths of the present study include its analysis of an outcome that has not been widely studied but is of keen interest to patients – the extent to which participants’ behavior is congruent with what is important to them. The study also benefits from the rigor of a randomized controlled trial design, its analysis of treatment completers, and its use of a well-validated measure of valued living. Limitations include its moderate sample size, the lack of a waitlist/placebo control condition alongside the active treatment groups which may support firmer conclusions, and the fact that the findings may not generalize to other populations and treatments.
Conclusions
These exploratory analyses suggest that CPT may improve valued living among Veterans with PTSD. Individuals scoring lower on measures of valued living and higher on measures of depression may derive more benefit in enhancing valued living. Among individuals undergoing these treatments, improvement in valued living does not appear to be dependent on improving symptoms. Further research replicating and extending these findings to new treatments and populations would further elucidate outcomes that are highly important to patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Department of Veterans Affairs RR&D Merit Review [grant number 1 I01 RX001485-01] to PJB; RJSH, DCM and TJA were supported by a Veterans Affairs Advanced Fellowship in the War Related Illness and Injury Study Center, a National Veterans Affairs Post-Deployment Health Resource.
Data Availability
Data may be obtained from the authors upon reasonable request.