
Abstract
Introduction
The Veterans Health Administration (VHA) initiated a system-wide redesign in 2011 toward a patient-centered approach called the Whole Health System (WHS) of care. Education of VHA clinical staff in WHS-informed care, Whole Health Clinical Care (WHCC), is one critical element of this redesign effort. At a minimum, WHCC education should address core competencies for clinicians and be considered satisfactory for learners. This is the first study to evaluate learner satisfaction and perceived achievement of course objectives in WHCC that incorporated active learning strategies.
Method
A large VA Healthcare System developed an in-person workshop focused on WHCC that used multiple active learning activities. These activities included case presentations, role playing, experiential learning, and group discussion.
Results
Sixty-two interprofessional staff attended the workshop in November 2019. Forty (64.50%) participants completed post-workshop surveys within 30 days. Data suggest participants were highly satisfied with the workshop and that they successfully met stated learning objectives.
Conclusions
We call on VHA and private-sector hospitals to train clinical staff in WHCC that incorporates use of active learning strategies.
Keywords
Introduction
In 2011, the Veterans Health Administration (VHA)’s Office of Patient Centered Care and Cultural Transformation (OPCC & CT) initiated a system-wide redesign effort to shift Veteran healthcare from a model focused singularly on disease management to one that also prioritizes a Veteran’s health and well
To promote this nation-wide cultural shift, it is critical to effectively train VHA staff to use WHS strategies in their work with Veterans and in their own lives. Such training must be centered on the five Whole Health Educational Core Competencies for Clinicians (WHCC Competencies) developed by OPCC & CT to ensure fidelity to the WHCC approach. These competencies focus on (1) helping Veterans explore their health and well-being and, if appropriate, co-creating a Personal Health Plan that incorporates values, (2) working effectively as a member of an interprofessional team, (3) demonstrating advanced skills in communication, empathy, and facilitation of behavior change, (4) integrating CIH therapies and use of CIH professionals as appropriate, and (5) applying a WHS approach to support staff health and well-being. To date, approximately 33 000 clinical and non-clinical VHA staff have received some form of WHS education. 4
When developing an educational offering, it is important to integrate impactful educational approaches to successfully achieve learning objectives and optimize participant satisfaction. Trainings that include active learning methods are associated with improved physician performance and patient health outcomes. 5 Specifically, case presentations increase participants’ reflection and commitment to change in their own practice. 6 Role playing connects theory and practice, allowing participants to use skills in realistic scenarios and think about complex situations from multiple perspectives. 7 According to Hewson and colleagues, use of experiential learning techniques improves physicians’ attitudes toward using CIH in their practices. 8 Group discussion has shown a broad range of positive benefits from increased tests scores to improved problem-solving.9,10 Finally, interactive follow-up activities (e.g., developing personal action plans or formal commitments to change) reinforce new skills, sustain learner engagement with the topic post-training, and support incorporation of new skills within practice over time.6,11
In sum, training VHA staff in the provision of WHCC is imperative for successful implementation of the WHS across VHA. Research suggests that incorporating active learning strategies when training health professionals is associated with satisfaction among adult learners, improved performance, and positive clinical outcomes. We are not aware of other studies that have described the use of multiple active learning strategies in the development of a WHCC course or evaluated participant response to the training (i.e., satisfaction, perceived achievement of learning objectives). The current paper seeks to address these gaps.
Method
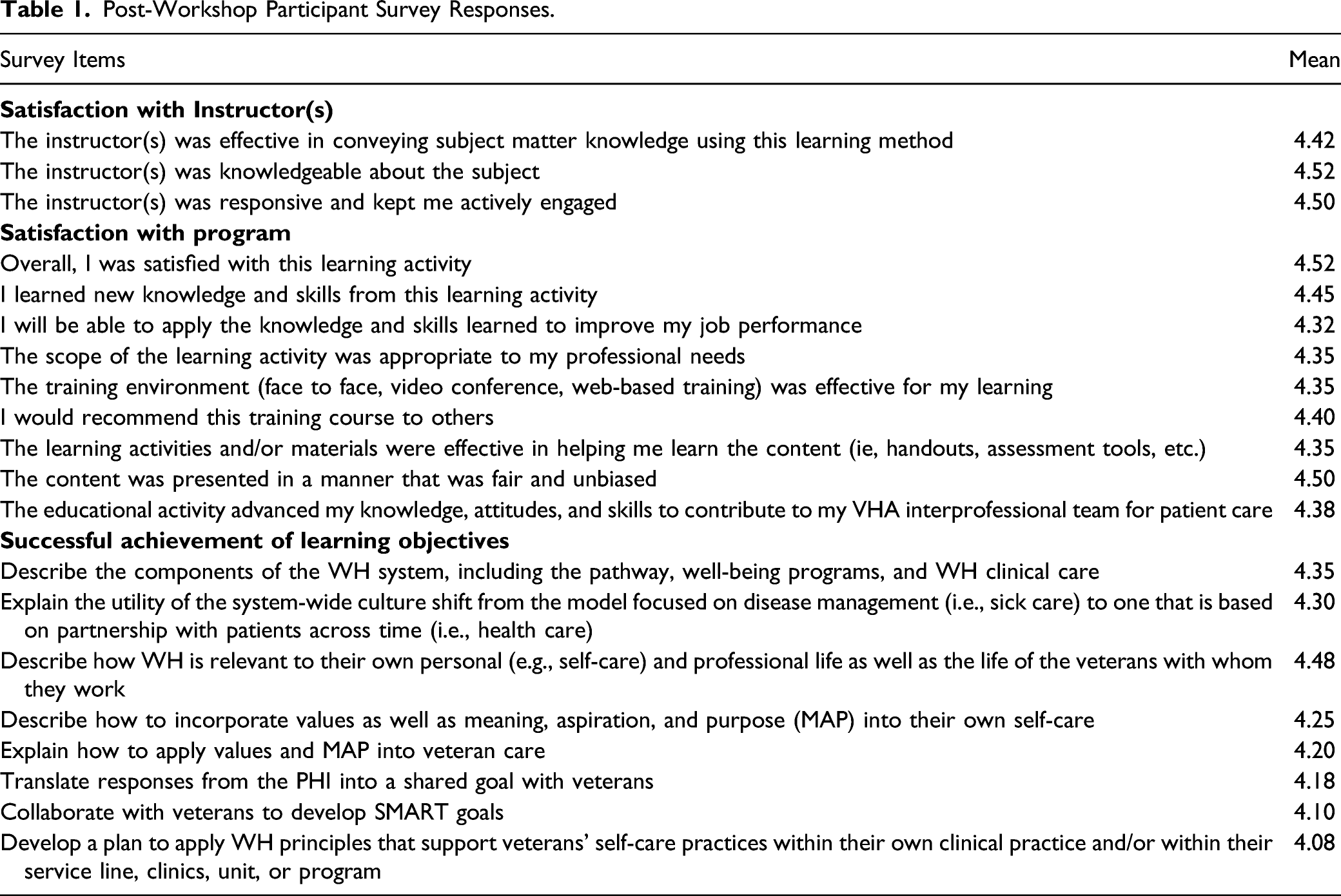
Post-Workshop Participant Survey Responses.
Case Presentations
Veteran and clinician case presentations were incorporated throughout the workshop. These case presentations illustrated the impact of WHS strategies in practice and helped workshop participants develop ideas about incorporating WHCC into their professional work. A Veteran patient provided a personal testimony highlighting the health benefits of the WHS approach. A Physical Medicine & Rehabilitation (PM&R) Service clinician shared her experience incorporating WHCC into her own individual visits. Finally, a panel of clinicians from a residential rehabilitation program discussed strategies for implementing WHS concepts within their standard operating processes across their service. There was time at the end of each case presentation for workshop participants to ask presenters questions.
Role Playing
Specific components of the PHP process were taught via a didactic presentation. A WHS team member and volunteer from the audience then role-played each component of the process to model how WHS practices can be used in the clinical setting. Role play components included: (1) self-reflection of MAP, (2) WHS assessment focused on self-care, (3) developing shared goals as a result of this exploration, and (4) creating a follow-up plan, which could include education, skill-building, resources, and support. Participants then had the opportunity to role-play these conversations with each other to develop skills in PHP. Participants in the patient role used a prepared case example or their own life experience to inform the conversation. This allowed for the opportunity to experience the WHS approach themselves.
Experiential Learning
Opportunities to experience and practice using WHS modalities were incorporated throughout the workshop. These opportunities included guided demonstrations of CIH modalities such as Yoga, Tai Chi, Meditation, and Guided Imagery, and the use of various WHS tools (e.g., the Personal Health Inventory) to support reflection of one’s own health and well-being. The Employee Whole Health Committee provided three stationary bicycles for participants to use during the workshop, which allowed participants to experience the impact of brief exercise on well-being. Some attendees also received Reiki.
Group Discussions
Following each role-play and experiential activity, participants engaged in small group discussions and then a large group debrief with the entire audience. Discussions focused on what participants learned during the workshop, what was challenging, potential opportunities for application to their professional practice and personal lives, and the overall experience of engaging with the learning activities.
Interactive Follow-Up
At the end of the workshop, participants were arranged into small groups based on discipline and clinical practice area. WHS team members joined each group to facilitate action planning for post-workshop skill application and implementation, answer content questions, and discuss opportunities to collaborate across services. Participants were given contact information for staff who could support implementation of these action plans.
Following the workshop, participants completed a survey assessing their satisfaction with the instructors (3 questions), the workshop (9 questions), and the workshop’s ability to achieve its stated goals and learning objectives (8 questions). Responses were based on a 5-point Likert scale with higher scores indicating increased agreement with the item. Specifically, 1 = “strongly disagree,” 2 = “disagree,” 3 = “neither disagree not agree,” 4 = “agree,” and 5 = “strongly agree.” Participants also indicated their profession (see Table 1).
Results
Sixty-two people participated in this workshop in November 2019. Forty participants completed post-workshop surveys within 30 days of course completion. Participants represented a range of health professions, including nurses (13; 32.50%), social workers (5; 12.50%), and psychologists (2; 5.00%). Other professions represented were occupational therapists (3), physicians (2), a dietician (1), physical therapist (1), physician assistant (1), and radiologic technologist (1). Fourteen participants did not specify their profession but did complete the survey. As displayed in Table 1, participants agreed with statements regarding effectiveness of the instructors, satisfaction with the workshop, and the workshop’s ability to meet the stated learning objectives. Further, 87.50% of participants reported they found the content of the program useful or extremely useful for their practice or professional development. In addition, 72.50% of participants reported they learned a fair amount or a great deal as a result of attending the workshop.
Discussion
To our knowledge, this is the first study to describe use of multiple active learning strategies to train clinical staff in WHCC and evaluate participant response to the training (i.e., satisfaction, perceived achievement of learning objectives). Overall, participants reported a high degree of satisfaction with the workshop content and instructors, believed the workshop was applicable to their professional work, advanced their knowledge and skills, and would recommend this training to their colleagues. Results also suggest that participants believed the structure of the workshop facilitated learning objectives and supported application of WHS strategies professionally and personally.
These findings have important implications for the broad transformation of healthcare. For example, VHA has partnered with the Whole Health Institute and the Samueli Foundation to co-sponsor the National Academies of Science, Engineering, and Medicine consensus panel called “Transforming Healthcare to Create Whole Health: Strategies to Assess, Scale, and Spread the Whole Person Approach to Health.” The goal of this panel is to examine whole-person models of care across healthcare systems to identify mechanisms for effectively building a WHS across the U.S. healthcare system, including at VHA. 4 Thus, it is likely VHA and private-sector clinicians will be trained in WHCC in the future. Our results suggest that healthcare leaders and educators may consider ways to incorporate active learning strategies into their teaching of WHS components.
Results are tempered by several study limitations, including the inherent limitations of self-report satisfaction data. In addition, the study did not directly assess the individual impact of the specific learning strategies used in the training, nor did it compare outcomes from training using more passive learning strategies. Further, causal inferences cannot be drawn between use and type of active learning strategies on satisfaction or achievement of learning objectives. Finally, while most participants agreed they would be able to apply the knowledge and skills learned to improve their job performance, post-course application of skills to professional practice was not formally evaluated, in part, due to limitations collecting data secondary to the ongoing COVID-19 pandemic.
Future research in this area can examine current WHS classroom to practice education efforts, which have been informally underway for many years throughout VHA nationally. It will be important to evaluate the impact of active learning strategies on application of WHCC skills within professional practice. This can include the impact of ongoing coaching, consultation, and sharing of best implementation practices, all of which is necessary for effective staff education and, ultimately, system-wide change. Future research should also collect both quantitative and qualitative data to understand the specific impact of each workshop component on participant satisfaction, application to clinical practice, and patient outcomes. Finally, it will be valuable to further explore how these active learning strategies can be incorporated when delivering WHS educational interventions virtually. 12
Conclusion
To meet VHA’s goal of system-wide transformation toward a WHS of care, it is essential to identify effective ways to teach WH strategies to VHA employees for use in their professional roles and in their personal self-care. Specifically, evidence-based, active learning strategies can be incorporated throughout these trainings. Future research will help identify which strategies are most effective in teaching each WHS component.
Footnotes
Acknowledgements
We would like to acknowledge the following people who contributed to the development and implementation of the Whole Health Clinical Care training discussed in this manuscript: Stephanie Adjei, Sandra Athanas-Moccia, RD/LDN, Jay Barrett, RN, BSN, MBA, Elyse Callahan, E-RYT 500, Michael Charness, MD, Kathleen Craig, RN, Teresa Czepiel, OTR/L, Mynor Diaz, BA, Lauren Durso, E-RYT 500, Mary Hanley, MA, BSN, RN, Kate Hinrichs, Ph.D., Julia Lehmann, MSW, LICSW, Sarah Leone, Ph.D., ABPP, Lindsay Lefers, PT, DPT, Kelvin McMillan, Brianne Molloy, Ph.D., Blair Morin, Michelle Nankin, MSSA, LICSW, Angel Ortiz-Bultron, Carrie Peterson, LICSW, Edward Phillips, MD, May Ramos, Elizabeth Recupero, DO, MPH, Michelle Remsen, OTR/L, LICSW, Marci Salow, PharmD, Stephanie Saunders, LICSW, ACHP-SW, Tanya Tarantino, Angela Viani, OTR/L, Stephen Wilmoth
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.