
Abstract
This paper provides a framework for understanding why, when and how to adapt mindfulness-based programs (MBPs) to specific populations and contexts, based on research that developed and adapted multiple MBPs. In doing so, we hope to support teachers, researchers and innovators who are considering adapting an MBP to ensure that changes made are necessary, acceptable, effective, cost-effective, and implementable. Specific questions for reflection are provided such as (1) Why is an adaptation needed? (2) Does the theoretical premise underpinning mainstream MBPs extend to the population you are considering? (3) Do the benefits of the proposed adaptation outweigh the time and costs involved to all in research and implementation? (4) Is there already an evidenced-based approach to address this issue in the population or context? Fundamental knowledge that is important for the adaptation team to have includes the following: (1) essential ingredients of MBPs, (2) etiology of the target health outcome, (3) existing interventions that work for the health outcome, population, and context, (4) delivery systems and settings, and (5) culture, values, and communication patterns of the target population. A series of steps to follow for adaptations is provided, as are case examples. Adapting MBPs happens not only by researchers, but also by MBP teachers and developers, who endeavor to best serve the populations and contexts they work within. We hope that these recommendations for best practice provide a practical framework for skilfully understanding why, when, and how to adapt MBPs; and that this careful approach to adaptation maximizes MBP safety and efficacy.
Introduction
Case Example 1: Alejandro Zima is a bilingual Spanish/English Licensed Mental Health Counselor and Mindfulness-Based Stress Reduction (MBSR) teacher. He specializes in grief counseling. Alejandro was considering whether to offer MBSR in a hospice setting to family members of hospice patients, particularly in their second year of grief or later as a “step beyond” program. His hospice setting already offered effective psychoeducational and counseling programs for the first year of grief (some that included basic mindfulness training) but there was a gap in effective programs beyond that time. In fact, most participants in his MBSR programs had participated in prior grief support programs and/or were currently receiving ongoing counseling supports. Informed by his training in MBSR, counseling theory, grief support methodologies, trauma-sensitive mindfulness, and post-traumatic growth, Alejandro felt that MBSR would likely be effective, but with a few tailored considerations in the participant screening process and curricular modifications, to help it better support people who are healing following the passing of a loved one.
Case Example 2: Eric Loucks, a cardiovascular epidemiologist and MBSR teacher, was interested in whether MBSR might reduce risk for cardiovascular disease. Turning to the scientific literature, the effects of MBSR in a systematic review and meta-analysis showed reductions of systolic blood pressure of 6.6 (95% CI: −11.7, −1.5) mmHg at immediate post-intervention follow-up.
1
Long-term effects are not yet clear.
1
He already knew research showed that major drivers of blood pressure are diet, physical activity, obesity, excessive alcohol consumption, and antihypertensive medication adherence, which MBSR does not explicitly address other than through yoga training.
2
He wondered if MBSR’s effects could be boosted, and MBSR be more accepted by people with hypertension, if its curriculum more explicitly directed mindfulness skill development to participants’ health behaviors that affect blood pressure (detailed elsewhere).
3
Case example 3. Mark Williams, a clinical psychologist was interviewed about Mindfulness-Based Cognitive Therapy (MBCT) for depression by a journalist, Danny Penman, for an article in a UK national newspaper. They got to talking about whether MBCT might go beyond depression to help all of us who are struggling with the everyday demands and challenges of life, including whether it could support well-being in the wider population. They collaborated on answering these questions and wrote a book, Mindfulness – A Practical Guide to Finding Peace in a Frantic World, that has been read by more than 1.5 million people and translated into more than 30 languages.
4
The work has been developed, implemented and researched as an in-person course.5,6
There has been an explosion of interest in mindfulness-based programs (MBPs).7-9 MBSR, which teaches mindfulness practices in group settings over an 8-week period using an established curriculum, has undergone hundreds of randomized control trials from which systematic reviews and meta-analyses show effects on outcomes such as stress, anxiety symptoms, depressive symptoms and chronic pain management.7-11 MBCT integrates MBSR with cognitive behavioral therapy (CBT) in ways that target the vulnerability factors for people at risk of recurrent depression. MBCT and MBSR have increasingly demonstrated effectiveness and cost-effectiveness, providing millions of people with choices about how best to recover and stay well in the longer term.8,12
Partially because of this careful work to develop and research MBSR and MBCT, there is growing awareness of, and demand for, MBPs in new populations and contexts. This has led to a proliferation of MBP innovations with potential to improve outcomes in target populations. However, there are also costs and downsides to adaptations. Careful adaptation is time and resource intensive. It requires research to investigate the acceptability, effectiveness and cost-effectiveness, and whether the adaptations work through hypothesized mechanisms. A key question is whether adaptations add value to other already available evidence-based programs. Finally, even if the adaptation proves to be acceptable and cost-effective, real-world implementation is complex and time consuming (such as training teachers, developing digital platforms and persuading policy groups to recommend it). Theory and research point to the facilitators and barriers involved in navigating an evidence-based MBP to targeted populations and new contexts.13-16
Nonetheless, there are several excellent examples of MBPs adapted to specific populations and contexts, such as depression (MBCT), 8 binge eating disorder (Mindfulness-Based Eating Awareness Training), 17 relapse prevention (Mindfulness-Based Relapse Prevention), 18 cancer (Mindfulness-Based Cancer Recovery), 19 and blood pressure (Mindfulness-Based Blood Pressure Reduction). 20 There are increasing adaptations to specific demographic groups, such as young adults (Mindfulness-Based College), 21 military personnel (Mindfulness-Based Mind Fitness Training, Mindfulness-Based Attention Training), 22 those with trauma history, 23 expectant parents (Mindfulness-Based Childbirth and Parenting Program), 24 and Native American communities (NativeMIND). 25 There are many more, and the evidence base and penetration of these MBPs varies greatly, from early preliminary studies (e.g., NativeMIND), through to extensive evidence and implementation around the world (MBCT). In some cases, implementation far outstrips the evidence, for example, with some mainstream mindfulness apps that are used by millions internationally. There are early promising findings for adaptations to online delivery formats: for example, randomized controlled trial showed online MBCT effectively prevents depression relapse 26 ; a pilot single-arm trial show the Eat Right Now app improved emotional eating 27 ; a systematic review of face-to-face MBPs delivered through videoconferencing online suggests beneficial effects. 28
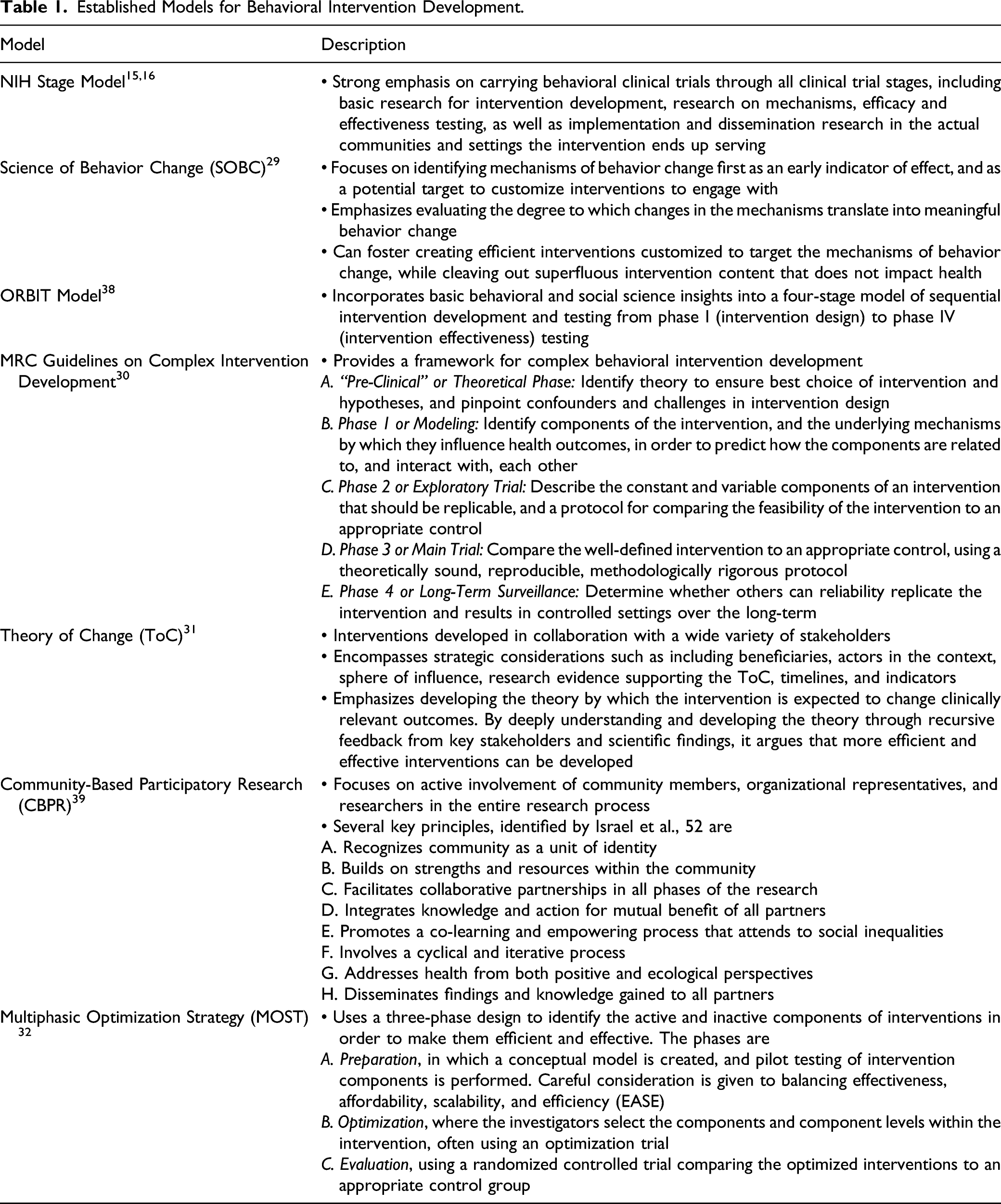
Established Models for Behavioral Intervention Development.
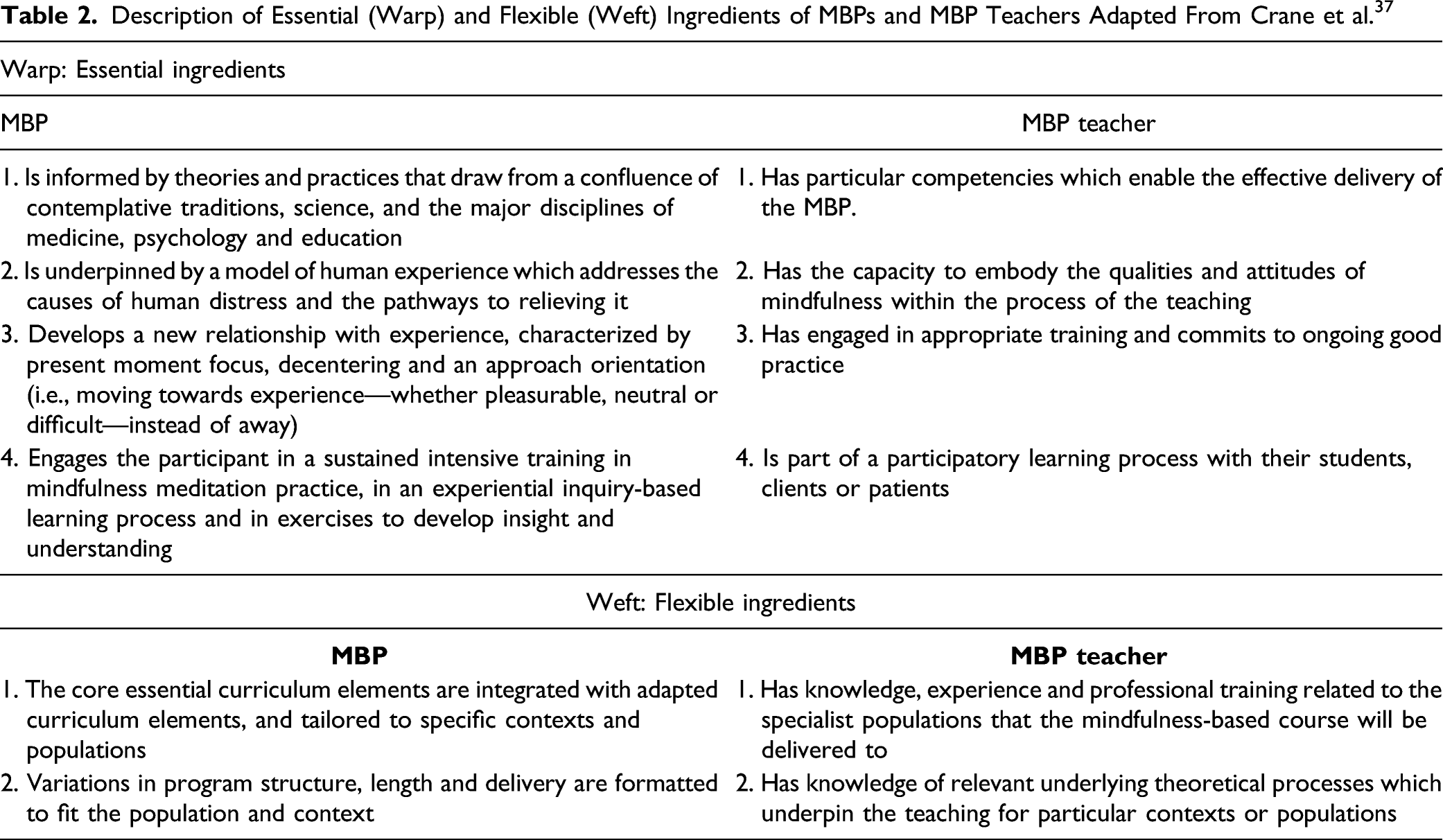
Description of Essential (Warp) and Flexible (Weft) Ingredients of MBPs and MBP Teachers Adapted From Crane et al. 37
This paper is a sequel to the warp and weft paper, providing a detailed framework on why, when and how to adapt MBPs to specific populations and contexts. Currently, such a framework for MBP adaptation is absent in the literature. We start by addressing the obvious first questions: “Why is an adaptation necessary?” “When should I adapt, and when shouldn’t I?” We then go on to address the question, “How should I adapt for this population or context?” Our intention is to support MBP teachers (case example 1), researchers (case example 2) and innovators (case example 3) in considering whether and how to adapt MBPs. In doing so, we hope to support participants and the wider field by ensuring MBP teaching is acceptable, effective, cost-effective, implementable, and underpinned by best professional ethical codes and practices. While considering adapting MBPs, we encourage qualities such as humility, curiosity, open-mindedness, clarity about aims, embracing diverse and challenging voices, listening, testing, iterating, improving, and continued engagement with personal mindfulness practice. In these ways, we anticipate that adaptations will have the greatest likelihood of being safe and helpful.
Why and When to Adapt an MBP?
Five Questions for Reflection in Considering Whether or Not to Adapt an MBP.

How to Adapt an MBP?
In order to develop an effective adapted MBP, there are fundamental knowledge domains required in the developmental team (see Figure 1). Fundamental knowledge domains required in the developmental team in order to develop an effective MBP adapted to specific populations or contexts.
Fundamental Knowledge Domains Needed to Skilfully Adapt an MBP
(1)Essential ingredients (i.e., warp) of MBPs: It is important to either be, or work with, a highly experienced MBP teacher who has deep knowledge of what MBPs are and aren’t.
37
MBPs’ warp includes a core theoretical basis that underlines the universal importance of foundational psychological skills such as attention, decentering and self-regulation (see Table 2).
42
This is an aspect of the essential theoretical ‘DNA’ and does not need adaptation if it is to be considered an MBP. The same applies to some of the vehicles of change within MBPs, namely, experiential learning through core mindfulness practices. These are defining premises of how MBPs are expected to effect change, even if the way they are offered is adapted. (2)Etiology of target outcome: For many conditions and diseases, we know a great deal about what causes, maintains and exacerbates them. For example, blood pressure is sizably affected by obesity, diet, physical activity, alcohol consumption, and antihypertensive medication adherence.
2
Once we know the modifiable determinants of the health outcome, we can design MBPs to engage participants’ relationships with these, such as through mindful eating or physical activity practices. In Case Example 2, a theoretical framework was developed using a Theory of Change approach (Table 1) for how mindfulness training could influence blood pressure.
20
It built upon prior theoretical work by Tang et al.
43
suggesting that mindfulness impacts 3 domains of self-regulation, specifically attention control, self-awareness, and emotion regulation. The theoretical framework extended to applying these 3 mindfulness skills to people’s relationships with their modifiable determinants of elevated blood pressure, such as diet, physical activity, and antihypertensive medication adherence. Example approaches used in MB-BP were directing participants’ improved self-awareness to how they felt before, during and after certain kinds of foods and physical activities, and then being with what insights arose from that awareness. In these scenarios, participants also used their improved attention control skills to redirect their attention to healthier choices (e.g., less reactive response to a stressor and healthier food selection).20,44 The detailed conceptual framework is described elsewhere.3,20 (3)Existing interventions that work for the health outcome, population, and context: At times, it may serve the MBP to weave evidence-based elements into extant approaches, in order to maximize efficacy. MBSR itself contains a variety of evidence-based intervention characteristics, such as participatory medicine practices and elements of motivational interviewing, such as during the last class where participants write a letter to themselves setting goals, considering what might get in the way of meeting those goals, and what they will do if that happens.
11
MBCT integrates MBSR and CBT. A challenge to this approach, particularly from a scientific and mechanistic perspective, is that, as most MBPs are complex behavioral interventions, this affects our ability to understand what the most active ingredients are. Hence, we must balance 2 considerations: Firstly, the encouragement for more dismantling studies using techniques in Table 1 such as the MOST framework to understand the maximally active elements, and cleave out unnecessary elements so that interventions are more cost-effective and efficient. Secondly, as MBP instructors often see during the end of the program when asking participants which practices they will continue with longer term, providing a panel of active elements within the program appears to meet different people in different ways, shown by the diversity of practices that participants plan to practice longer term to support their well-being (e.g., body scan, attentional focus meditation, yoga, and loving-kindness meditation). A sizable range of meditation practices was recently demonstrated in a sample of diverse meditation practitioners,
45
recognizing different practices support well-being of individuals in unique ways. It is a challenge for mindfulness intervention developers to create interventions that are likely to be accepted by a large segment of society while keeping them efficient and understanding the mechanisms by which they operate. (4)Delivery systems and settings: The variety of settings and methods by which MBPs can be delivered is wide. Delivery can occur in distinct physical settings, such as grade school classrooms, military barracks, corporate workplaces, prisons, or local health centers. MBPs are increasingly being delivered digitally.26-28 A frontier of digital mindfulness research is determining the value of these universal elements of MBPs, asking, “What is essential?” For example, Table 2 suggests that 2 essential elements of an MBP are: “Engages the participant in a sustained intensive training in mindfulness meditation practice, in an experiential inquiry-based learning process and in exercises to develop insight and understanding” and the teacher “Is part of a participatory learning process with their students, clients or patients.” Some MBP apps have synchronous (i.e., live) elements with teacher feedback, like Unwinding Anxiety and Eat Right Now.27,41 Is the synchronous element needed, and does it maximize positive effects and minimize adverse effects? Alternatively, is purely asynchronous (i.e., static) content, such as that delivered by popular apps like Headspace and Calm, or by books, enough? As technological developments in machine learning, artificial intelligence, social interaction, and mobile sensing continue, there will be increasing opportunities to adapt digitally delivered MBPs in accessible, scalable ways.
46
Other explorations include stepped care models that would encourage the use of apps, books, self-taught, or lightly supported interventions in mild to moderate conditions—and more intensive teacher/therapist led interventions for people with more challenging issues. There can even be bidirectionality where people may find themselves drawn to different delivery systems at different times in their lives. These are important domains to explore and systematically research as there are sizable accessibility and cost-effectiveness implications. (5)Culture, values, and communication patterns of target population: The importance of culture, race, gender, sexual orientation, and age are increasingly recognized in mindfulness research.47,48 In terms of race and culture, a qualitative study by Tenfelde et al, in predominantly low income African American women, found the participants recognized that yoga and mindfulness could be beneficial, and found several recommendations for culturally adapting it to them, including (1) Focusing on stress relief and health benefits; (2) Changing the image of yoga to include the Black community; (3) Peer to peer teaching; and (4) Afro-centric history and connection to yoga.
49
Bringing forward the culture, values and communication patterns of target groups, whether it is by race, ethnicity, age, gender, or disability status, to name a few, and preferably taught by a member of that group, are important ways to ensure that MBPs are accessible to the broad diversity of people throughout the world, as well as to diverse communities within countries.
47
For example, in the community-based participatory research being done for the NativeMIND study, 25 participants are explicitly naming how they are “indigenizing and decolonizing MBSR” as they adapt it to Native American cultures and traditions. This, for example, in one tribal nation, includes using a drum instead of bells to begin and end meditations, and in other tribal nations doing slow ceremonial dances instead of walking meditation. Clear feelings have been expressed in focus groups that NativeMIND is now an authentic expression of their culture and values. When participants feel ‘met’ by the teaching process, the potential for deeper engagement and transformation is significant. 50 In adapting MBPs, it is fundamental to adapt with rather than for the communities and contexts.
Develop and Test Your Adaptation: 8 Steps to Adaptation
Based on experience developing and adapting MBPs, we offer recommendations on steps to adaptation. We recommend researchers follow all steps, while mindfulness teachers may consider following steps 1 through 5. Partnering with researchers is encouraged so that the safety and efficacy of the adaption can be understood, enhancing the chances that the adaptation is evaluated and sustainably implemented. We recommend adhering to best practices for behavioral intervention development, outlined in Table 1. This includes engaging stakeholders in every step of the path (e.g., patients, clinicians, and health insurers) so that an intervention that meets the needs of the population is developed. It is beyond the scope of this paper to outline these steps in detail; a well assembled collaborative team would cover the requisite knowledge and skills to conduct these steps. Refer to the reflective questions in Table 3 while considering these 8 recommended steps for adaption: (1)Determine if this work is needed. Perform a thorough review of the literature, and engage with diverse stakeholders, to establish what is already known about MBPs in the target population and context, and determine if there are already adaptations or alternative non-mindfulness-based approaches being used. (2)Articulate the aim and intention of the adaptation, and the theoretical basis of why an MBP would be helpful for this population or context. Include a theoretical account of the issue of concern in the target population, and how an MBP would address the specific mechanisms (e.g., using the Theory of Change approach in Table 1). (3)Generate and develop ideas for the necessary adaptations. Work creatively with a group of MBP teachers and representative key stakeholders, including those with lived experiences of the issues of concern and the delivery context, and those with expertise in the target population and context. (4)Evaluate feasibility: This can include qualitative interviews with people from the target population/context, single-arm pilot trials of the adapted program monitoring acceptability and feasibility, along with exploratory work about the impact on proposed mechanisms and outcomes. (5)Steps 3 and 4 continue iteratively until a theoretically plausible, acceptable, feasible, and potentially safe and potent adaptation, is ready to pilot. (6)Pilot clinical trial, with meaningful measures of acceptability, feasibility, harms, adverse events, mechanisms and effectiveness, using a meaningful comparison group. (7)Perform an adequately powered preregistered randomized controlled trial, adhering to CONSORT guidelines,
51
to evaluate impacts on the primary outcome of interest, and relevant mechanisms. (8)If efficacy in step 7 is sizable, carefully proceed with replication, scalability, dissemination, and implementation studies, using stepped implementation science-informed approaches such as those outlined in the NIH Stage Model,15,16 Science of Behavior Change,
29
Obesity-Related Behavioral Intervention Trials (ORBIT) model,
38
Multiphasic Optimization Strategy (MOST),
52
and MRC Guidelines on Complex Intervention Development.
30
as summarized in Table 1. Our three case examples have progressed through these steps to differing degrees. Case example 1 moved through steps 1–4 to see that a full adaptation of MBSR was not needed, but instead MBSR was used with more minor modifications and screening considerations such as those described in Table 3. To establish if MBCT could be accessible to the general population, the new Finding Peace in a Frantic World (case example 3) passed through steps 1 through 7. It is also emerging in step 8 through book distribution and reader feedback). MB-BP (case example 2) has advanced through steps 1 through 6, with step 7 recently completed and analyses underway.
Strengths and Limitations of This Framework
Strengths of the MBP adaptation system provided in this paper include grounding it in the established theoretical framework of the essential (warp) and flexible (weft) ingredients of MBPs. The recommendations on how to adapt MBPs are linked to established behavioral intervention development methods such as the NIH Stage Model,15,16 Community-Based Participatory Research, 39 MRC Guidelines on Complex Intervention Development, 30 and others described in Table 1. Limitations include that, while the warp and weft are informed by theory and practice, the proposed essential and flexible elements have not yet been empirically tested to identify which are more active. These elements were offered by a team of researchers that included some of the first- and second-generation designers of MBSR and MBCT, so reflect their best understanding of active and unique components. Empirically validating the warp and weft elements remains an opportunity for future research.
Summary and Conclusion
Adapting MBPs is currently happening not only in research, but also by MBP teachers and developers who endeavor to best serve the populations and contexts they work within. This paper provides a set of principles and criteria for when, why and how to adapt MBPs. We suggest ways to ensure adaptations to MBPs are acceptable to populations and contexts, and become potentially scalable, thereby creating efficient and effective programs to maximize public health. Our hope is that this provides a useful framework for ensuring that further developments in the field of MBPs systematically consider safety, acceptability, effectiveness, cost-effectiveness and scalability so their potential to enhance public health and well-being is maximized.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Loucks is the director of the Mindfulness Center at Brown University. The Mindfulness Center, a non-profit entity, has an Education Unit that provides mindfulness-based program delivery to the general public for fees. Dr. Loucks’s salary is not tied to quantity or content of programs offered through the Mindfulness Center.
Rebecca Crane receives royalties from books on mindfulness
Judson Brewer owns stock in, and serves as a paid consultant for Sharecare Inc. the company that owns the Eat Right Now and Unwinding Anxiety apps mentioned in this manuscript. This financial interest has been disclosed to and is being managed by Brown University, in accordance with its Conflict of Interest and Conflict of Commitment policies.
Willem Kuyken is the director of the Oxford Mindfulness Centre. Since arriving in Oxford (2014) he has received no payments for training workshops, presentations or consultation work related to his MBCT work and donates any such payments to the Oxford Mindfulness Foundation, a charitable trust that supports the work of the Oxford Mindfulness Centre. He was until 2015 an unpaid Director of the Mindfulness Network Community Interest Company. He receives royalties for several books on mindfulness published by Guilford Press. He has advised and consulted various groups (e.g., evidence to UK NHS committees, the UK Mindfulness All Party Parliamentary Group).
Other authors report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Aging and Mount Sinai Health System.