
Abstract
Objectives
To determine acute effects of stress-reduction guided imagery delivered in group format on stress biomarkers salivary cortisol and salivary amylase, and on self-reported stress mood, in healthy, predominantly Latino adolescents.
Study Design
111 adolescent participants (94% Latino), a subset from a large, randomized controlled lifestyle intervention to improve obesity-related health behaviors, received either 4 weekly lifestyle education sessions (Lifestyle group; LS) or the same weekly lifestyle education sessions plus an additional weekly stress-reduction guided imagery session delivered in group format (Guided imagery group; GI). Salivary cortisol, salivary amylase, and self-reported stress moods were assessed before and after sessions on intervention weeks 3 and 4. Statistics: Linear mixed effects models examined within- and between-session and group differences in pre- to post-session changes.
Results
Both groups showed decreases in salivary cortisol, 5% decrease in LS group and 32% in GI group (within-group differences all P < .05), with between-group difference in salivary cortisol of moderate size (P = .05; Cohen’s d = .44). Within the GI group alone, salivary cortisol decrease was similar following either the lifestyle or GI sessions (P = .64). There were no statistically significant amylase changes within or between groups. All 5 individual stress moods declined by 27% to 46% in the GI group (all P < .05), while only 1 of the 5 declined in LS group.
Conclusions
Group stress-reduction guided imagery reduces the stress biomarker salivary cortisol, as well as reducing subjective stress mood states, making it a viable modality for large scale stress-reduction interventions.
Introduction
Adolescents and children living today suffer from significantly higher levels of stress and anxiety than did youth in the past.1,2 Latino adolescents may suffer from higher levels of psychosocial stress due to a combination of factors including immigration, acculturation, discrimination, or socioeconomic stressors.3–5 Latino adolescents also represent a group at high risk for both obesity 6 and obesity-related morbidities, such as type 2 diabetes 7
Chronic stress and altered hypothalamic–pituitary–adrenal axis activity have been linked to both an increase in obesogenic lifestyle behaviors (e.g., ingestion of high caloric “comfort” foods) 8 and obesity-related disease risk in adults.9–11 This evidence suggests that chronic stress may result in subtle degrees of hypercortisolism, promoting obesity-related morbidities, and risk for diabetes. Specifically with respect to children and adolescents, we previously found that in overweight and obese Latino children, ages 8–13, morning serum cortisol was higher in those with metabolic syndrome than in those without, and that serum cortisol increased in conjunction with increased number of features of metabolic syndrome. 12 Additionally, in obese Latino teens, a blunted rise in cortisol overnight was associated with increased carotid intima media thickness (a marker of preclinical peripheral vascular disease). 13 These findings suggest that disruption in the hypothalamic–pituitary–adrenal (HPA) axis may increase risk for development of obesity in non-obese individuals, as well as obesity-related co-morbidities in obese youth and adults. In addition, stress has been linked to behavioral and mental health morbidities in youth independent of obesity status, particularly in minority youth where acculturation, perceived discrimination, and cultural stress have been linked to substance use and mental health issues among Latino adolescents14,15 and perceived discrimination in adolescence has been linked to altered cortisol awakening response in African Americans. 16 Stress-reduction modalities that could modify cortisol responses might therefore be a useful integrative approach for stressed youth in general, as well as an important addition to traditional lifestyle approaches17,18 designed to prevent or treat obesity in children and adolescents.
These considerations led us to explore the effects of a stress-reduction, mind–body integrative modality, Interactive Guided ImagerySM, as a possible therapeutic modality to lower cortisol levels in obese, Latino adolescents at risk for diabetes. In this population, stress-reduction interactive guided imagery delivered to individuals acutely lowered salivary cortisol.19,20 However, the cost and labor that would be needed to deliver an in-person, individualized guided imagery stress-reduction intervention, makes it impractical for use in larger scale interventions. In addition, this work did not address the utility of guided imagery in reducing cortisol in non-obese youth. Recently we replicated the acute salivary cortisol reduction using stress-reduction guided imagery (SRGI) delivered in group format 21 in a small population of obese and non-obese youth, but without a concurrent control group, limiting the interpretability of these findings. These findings need to be replicated in a larger study population with an appropriate control group.
The generalized stress response consists of both HPA axis and autonomic nervous system responses. 22 While cortisol responses to acute stressors have been well-characterized 23 and HPA axis dysregulation has been linked to multiple health issues, 24 the autonomic nervous system response to stress, particularly in children, has been less studied. Salivary amylase is a marker of sympathetic nervous system function, 25 and is increased following acute stressors in both adults and adolescents.26,27 While some behavioral interventions in adults have shown changes in salivary amylase, few studies have assessed acute changes in amylase in response to short-term mind–body stress-reduction modalities, and none to our knowledge have done so in children.28,29
Therefore, the purpose of this report is to determine the acute effects of SRGI delivered in group format compared to an active control group (lifestyle education) on self-reported stress mood and on the stress biomarkers salivary cortisol and salivary amylase in a population of generally healthy, obese and non-obese, predominantly Latino high school students. We hypothesized that there would be significantly greater reductions in salivary cortisol and self-reported stress mood between-groups receiving SRGI compared to those receiving lifestyle education alone. We also hypothesized that among participants within the SRGI group only, reductions in salivary cortisol and stress mood would be greater following SRGI sessions compared to following lifestyle education sessions. We further sought to explore the response of salivary amylase, a marker of sympathetic autonomic nervous system activity, to the SRGI, hypothesizing that salivary amylase would be reduced following guided imagery.
Methods
Participants
Participants reported in this study represent a subset of the Imagine HEALTH parent study, a 12-week behavioral lifestyle RCT intervention utilizing guided imagery for which the full protocol and primary outcomes (physical activity and dietary intake) have been previously described in detail.30,31 Briefly, sophomore and junior high school students of any age, gender, or BMI status were recruited during in-person staff recruitment visits during required classes (e.g., History and English) from 4 public high schools in eastern Los Angeles. Exclusion criteria included serious chronic illness, eating disorder, psychiatric disorder, or physical, cognitive, or behavioral disability; use of medication known to affect body composition; lack of English fluency; or concurrent activities that would interfere with the ability to attend after-school intervention sessions. Prescreening phone calls were made by study staff, followed by group consenting and enrollment visits where written parental consent and youth assent were obtained. This study was approved by the Internal Review Board (IRB, #HS-13-00836) of the University of Southern California Health Science Campus.
Study Design
The present study presents methods and results from the subgroup of participants during the first 4 weeks of our previously reported overall 12-week lifestyle intervention.30,31 For the parent study, 232 eligible participants underwent group consenting and enrollment visits (Figure 1). The intervention was delivered during the after-school hours (starting approximately between 3–3:30 Legend * Reasons for not meeting inclusion criteria: • Inadequate time available: 750, • Other after-school activities: 214, • Incorrect age/grade: 19, • Serious illness/medications: 27, • Behavioral disorder/cognitive issue: 29, • Lack of English fluency: 8, • Other: 8.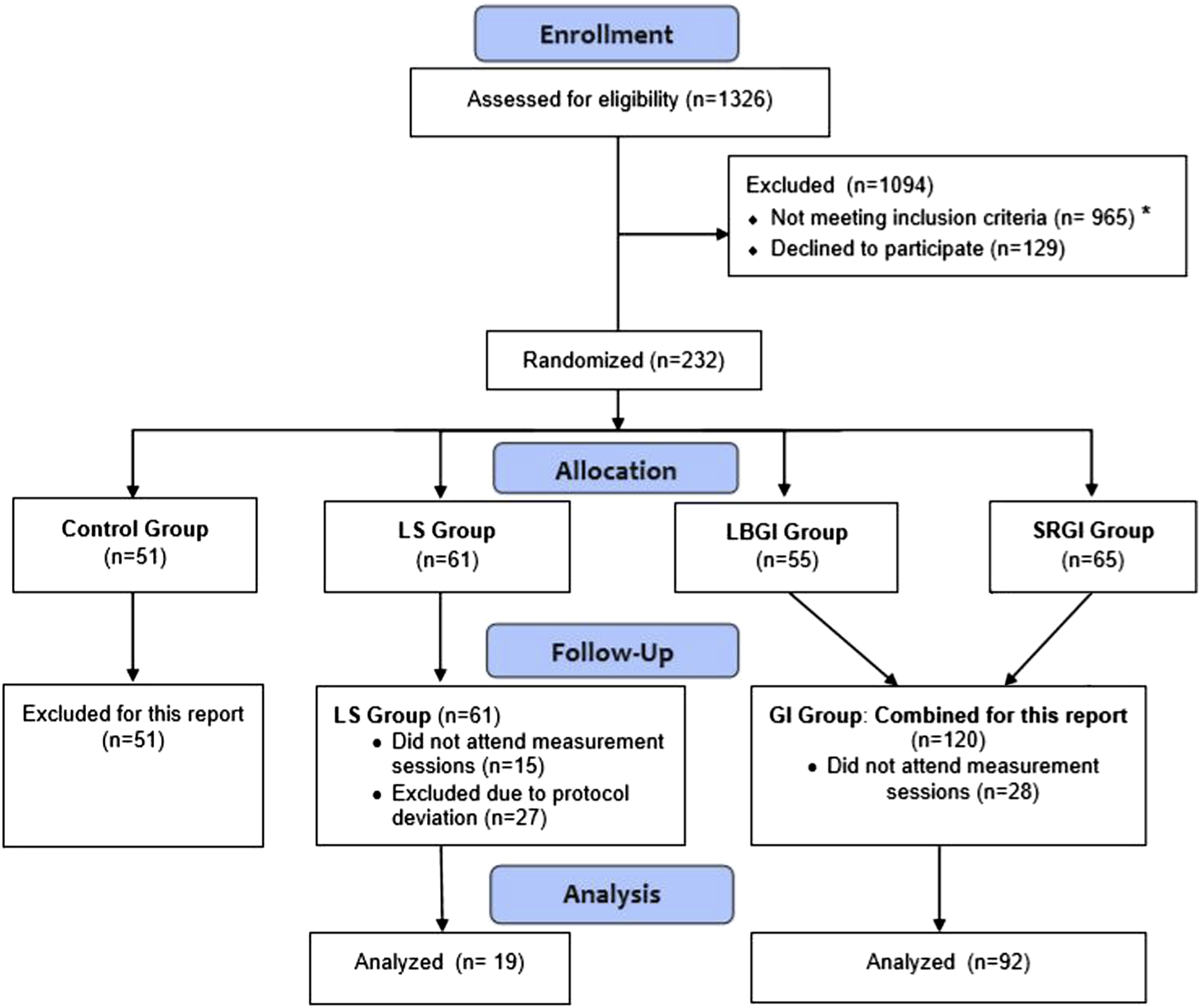
Delivery of Group Guided Imagery and Lifestyle Classes
Weekly lifestyle education classes were delivered during after-school hours (generally starting between 3–3:30
Guided imagery sessions were delivered in a classroom setting during the same after-school hours in the context of the facilitated group process known as “council.”21,30 Interventionists were highly skilled professionals with certification training in Interactive Guided ImagerySM (https://acadgi.com/certification/), including an academic social worker, an integrative physical therapist, an expressive arts therapist, and a personal coach practitioner with long-standing certification in interactive guided imagery. All were trained in the council process by the PI and an experienced council practitioner consultant from the Los Angeles public schools’ “Council in Schools” program. Fidelity of the intervention delivery was assessed weekly across the duration of the intervention by the PI, as previously described in detail. 30 Each weekly GI council session started with a personal “check in” and a brief report of their home imagery practice from the preceding week, followed by an explanation of the GI exercise about to be undertaken (∼25 minute duration). The group GI exercises were then conducted using pre-written scripts (∼25 minute duration). As previously detailed30, the specific content of the 4 weekly sessions were as follows: (1) Relaxation breathing; (2) Relaxation breathing plus progressive muscle relaxation (PMR); (3) relaxation breathing + PMR + “relaxing place” imagery (exploration of a mental image of a place that represents just comfort and relaxation); and (4) repeat of relaxing place imagery, followed by a second imaginal exploration of the relaxing place after only 3-focused breaths. Following each group SRGI session, participants debriefed their imagery experiences in the council format (duration ∼25 minutes). Each week participants were encouraged to practice the SRGI exercises at home for at least 10 minutes a day between sessions.
Outcome Procedures and Measurements
Acute Change in Salivary Cortisol and Salivary Amylase
Saliva was obtained by research study staff using Salivettes pre- and post-individual intervention sessions (∼75 minutes apart) on weeks 3 and 4 of the intervention period. For the LS group, saliva was collected immediately before and immediately after the weekly 75-minute nutrition education sessions of weeks 3 and 4. For the GI group, saliva was also collected immediately before and immediately after the nutrition education session, as well as before and after the additional weekly 75 min stress-reduction GI sessions during weeks 3 and 4. Sampling was done in weeks 3 and 4 in order to minimize the session burden in weeks 1 and 2, the first 2 sessions of a complicated 12-week intervention, and to allow the subjects to get familiar with all processes of the weekly group intervention sessions. The nutrition education session was chosen as the comparison group since the guided imagery group also took the nutrition class and this therefore was a parallel experience for both groups. No collections were made following the physical activity sessions due to the potential confounding effects of exercise on cortisol. Due to an inadvertent protocol deviation caused by human error, we estimate that 44 salivary samples from 27 participants in the LS group were not collected, resulting in a significant study group size discrepancy. Salivettes were returned on the same day as collection to our laboratory and stored at −800C until processing, at which point they were thawed and then centrifuged at 2500 RPM for 10 minutes. Saliva was then aliquoted and stored in cryovials at −800C until subsequent assay using commercially available assay kits (salivary cortisol ELISA, Salimetrics, Inc; inter-assay CV = 3.75% [high], 6.41% [low], sensitivity 2 nmol/L (.007 mcg/dl); salivary amylase kinetic enzyme assay, Salimetrics, Inc, inter-assay CV = 4.7%, intra-assay CV = 5.5%).
Acute Change in Stress Mood State
Stress mood was measured using the tension subscale of the Profile of Mood States for Adolescents (POMS-A) (168), a 24-item measure of mood that has been validated extensively in adolescent populations. 33 Study staff administered a visual analog scale containing the 4 individual mood items (“worried,” “nervous,” “panicky,” and “anxious”) plus an additional fifth item (“stressed”), at the identical timepoints of the saliva collection, pre-session and post-session during weeks 3 and 4 of the intervention. Changes in mood scores were calculated as the post-session minus pre-session difference in each of the 5 individual scale items, as well as a “total” mood score calculated as the average of the 5 individual mood scores before and after the session.
Statistical Analyses
To test the primary aim that there was a difference in decrease within session between the LS and GI groups, cortisol, amylase, and stress mood scores were examined using linear mixed effects models to examine the difference in change from pre- to post-session for LS or GI sessions. Change scores were calculated as post-session level minus pre-session level so that a negative value would indicate a decline within session. Data from both Sessions 3 and 4 were included. Since there were no differences seen between Session 3 and Session 4 values in our preliminary analyses, we included session as a repeated measurement and not a covariate in the models. Nutrition sessions include measures for both LS and GI, while guided imagery sessions include data from only GI group, as these sessions were not attended by the LS group. The model was adjusted for the starting value at each session and randomized group. Further modeling for the GI group alone was performed to determine if there was a difference in response to the type of session (Nutrition vs GI). Winsorized assay values were used so that estimates would not be unduly represented by outliers. Analyses were performed using SPSS (v.24); a priori α = .05 for examining the difference in intra-session change between GI and LS sessions. In order to understand the clinical magnitude of effect, percent change within groups and estimated marginal means for the models were used to compute estimates of effect size, Cohen 34 ’s d, which calculates the difference between groups in the unit of a SD. This allows us to determine the size of the effect as small (d = .2), moderate (d = .5), or large (d = .7).
Results
Participant Characteristics.
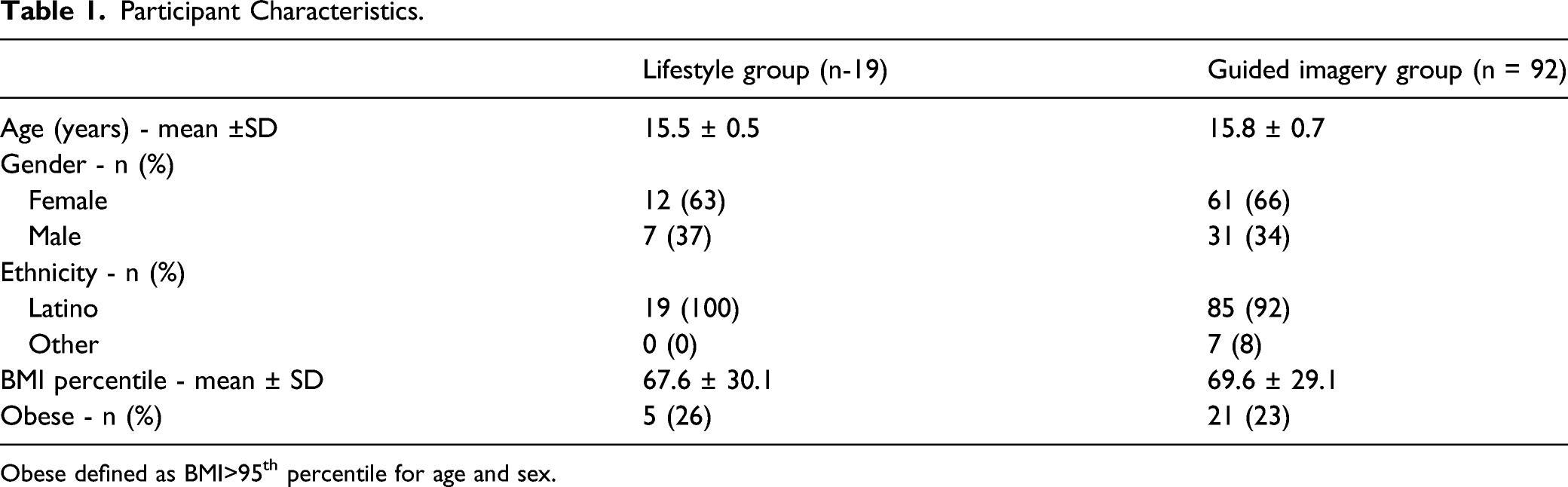
Obese defined as BMI>95th percentile for age and sex.
Salivary Cortisol, Salivary Amylase, and Self-Reported Stress Within Sessions.
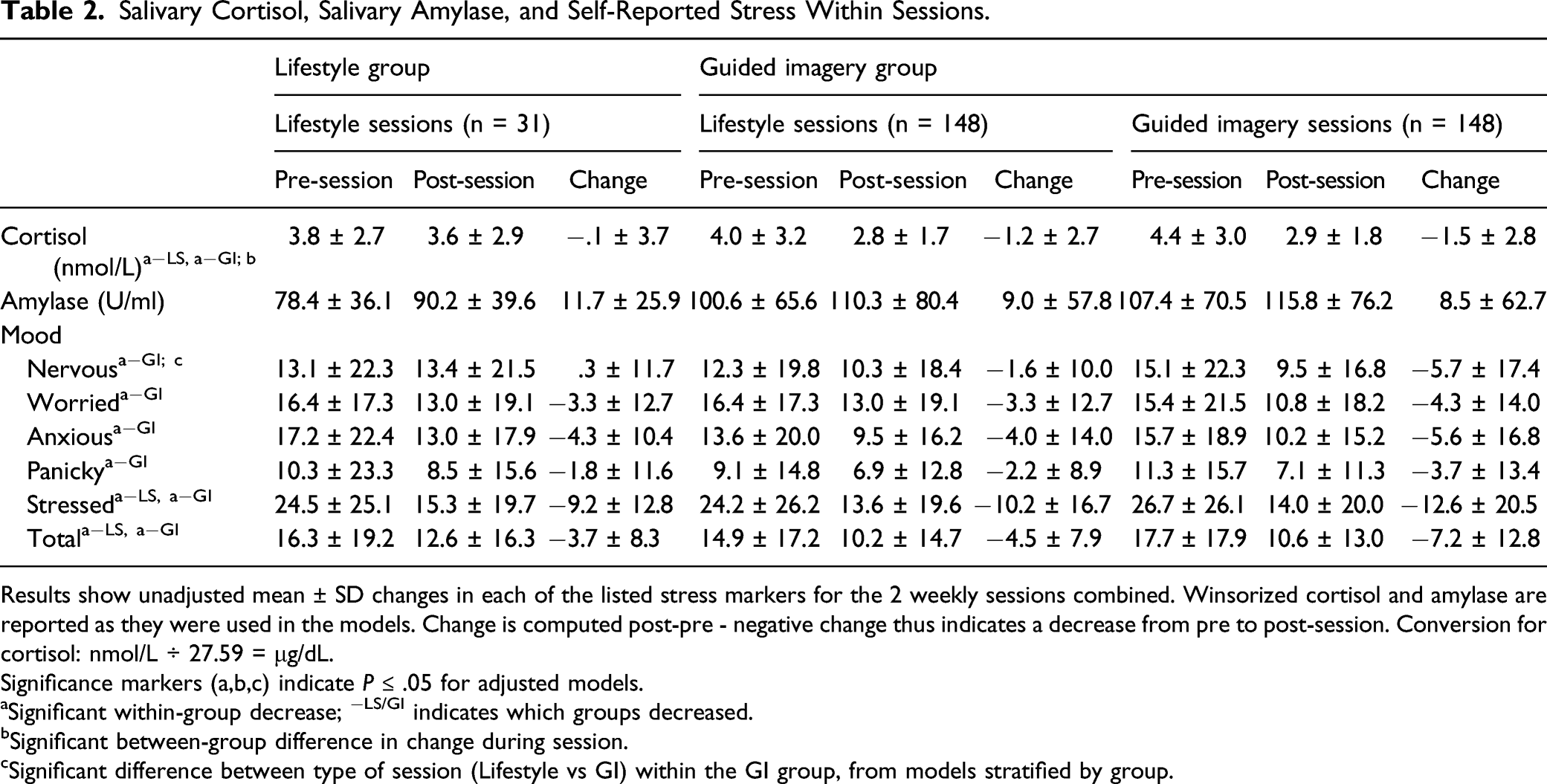
Results show unadjusted mean ± SD changes in each of the listed stress markers for the 2 weekly sessions combined. Winsorized cortisol and amylase are reported as they were used in the models. Change is computed post-pre - negative change thus indicates a decrease from pre to post-session. Conversion for cortisol: nmol/L ÷ 27.59 = μg/dL.
Significance markers (a,b,c) indicate P ≤ .05 for adjusted models.
aSignificant within-group decrease; −LS/GI indicates which groups decreased.
bSignificant between-group difference in change during session.
cSignificant difference between type of session (Lifestyle vs GI) within the GI group, from models stratified by group.

Salivary cortisol within-session change by group and type of session. Legend: Values display adjusted M +/− 95% CI for the change in salivary cortisol across Sessions 3 and 4 of the intervention (i.e., post-session minus pre-session value, adjusted for pre-session values and repeated measures). Both groups decreased in cortisol within session, as demonstrated by 95% CI for each group being <0.
For the self-reported stress mood measures, there was a significant decline in all 5 individual mood state measures, as well as in the “total” average score of the 5 mood state measures combined, within the GI group (all P < .05), with percent decreases in mean scores ranging from 27% to 46%. The LS group decreased significantly only for the feeling “stressed” item, and in the total average mood score (38% and 23% decrease, respectively). However, there were no significant between-group differences in any of the self-reported changes in mood states, as is shown in Table 2, and all between-group effect sizes were small, (Cohen’s d ranging from .04 to .25). When examining the difference in mood states relating to session type for the GI group only, there was a significant difference only for the feeling of “nervous,” with the change in “nervous” mood being greater after the GI session vs after the lifestyle session (P = .003; Cohen’s d = .31; Figure 3). Nervous mood within-session change by group and type of session. Legend: Values display adjusted M +/− 95% CI for the change in nervous mood across sessions 3 and 4 of the intervention (i.e., post-session minus pre-session value, adjusted for pre-session values and repeated measures). The GI group decreased significantly within session as demonstrated by 95% CI being <0.
Discussion
The results of this study replicate our earlier, uncontrolled pilot findings that SRGI delivered in group format leads to acute reduction in salivary cortisol levels in adolescents, adding our understanding that this effect is present whether the imagery is delivered to individuals, 20 or in groups. 21 To our knowledge, this is the first report of a randomized controlled study showing significant reductions in salivary cortisol in adolescents in response to group GI. In the present study, the decrease in salivary cortisol in the GI group compared to the LS control was of moderate effect size. It is also important to note that the 32% reduction in cortisol seen in the present study was comparable in magnitude to the 38% reduction previously seen in response to individual SRGI. 20 Other mind–body modalities have been shown to reduce either self-reported stress or cortisol values. Pawlow et al. showed reductions in salivary cortisol following progressive muscle relaxation in adults, 35 and mindfulness-based stress reduction has been shown to similarly reduce self-reported stress. 36 Thus, our findings can be placed in the increasing body of evidence that there are multiple mind–body approaches to address stress in both adults and youth, and that group guided imagery is one of several effective modalities that can be used to reduce stress in the short term in adolescents.
The finding within the GI group that salivary cortisol decreased comparably whether the subjects were experiencing either the SRGI or the lifestyle education class in the after-school period was unexpected. This may indicate that there was a non-specific effect of participating in the GI council group on the cortisol biomarker at this time of day, such that a cortisol lowering effect was seen when participants gathered at the same time with their group whether receiving SRGI or the nutrition class. A possible explanation for this occurrence is an increase in group cohesion, trust, and stress-reduction from having participated in the GI council and therefore trained in relaxation techniques for the 2 weeks prior to assessment in weeks 3 and 4. This is supported by our prior findings that council alone reduced subjective stress in young adults with type 1 diabetes. 37 As these measurements were made during the third and fourth week of the intervention, per protocol, the GI group may have experienced the after-school gathering as relaxing, no matter what specific activity they undertook. Unfortunately, we did not measure salivary cortisol and stress mood changes within Sessions 1 and 2, which might have shown that this nonspecific group effect was not present at the early sessions, but developed as the program went on and the GI group learned the relaxation techniques and grew more cohesive. Another related possibility for this finding is that the GI group participants actually used their breathing and imagery techniques during the nutrition sessions without being instructed to do so, thereby leading to comparable cortisol lowering following the after-school lifestyle sessions. If so, this would indicate an acceptability of the guided imagery modality to a level where the participants use it in aspects of their life not directly related to the study protocol. This is supported by our previous findings 21 and anecdotal experience in this study, that once adolescents are trained in GI, they spontaneously use it without instructions to do so in settings outside the formal intervention structure.
The findings that GI reduced stress mood in all 5 of the individual mood states further supports the use of GI for stress management in this population. That the reductions in stress mood states were not statistically significantly different between LS and GI groups is likely due to the very large variability in these data, particularly in the LS group which had a smaller sample size. Students discriminated among the various mood states as well, with the feeling state of nervous being particularly affected by SRGI. This may indicate actual differences in GI effects on these specific moods, or more likely indicates a different level of specificity in the participants’ ability to recognize and label the various moods. For example, feeling nervous could be a mood easily identified within the life experience of the students, whereas feeling panicked was less so. Regardless, these findings suggest the youth not only showed reduced cortisol stress biomarker, but actually felt a reduction in stress mood following GI.
Salivary amylase is generally considered to be a biomarker of sympathetic autonomic nervous system activation, 25 and therefore part of the acute systemic stress response. 38 Prior studies have demonstrated increases in salivary amylase following natural and laboratory stressors in adults as well as adolescents.26,27 These findings, and others suggesting that salivary amylase may be expected to decrease in response to therapeutic stress-reduction intervention, 39 led us to explore whether salivary amylase would acutely decrease in response to SRGI. However, we did not see such a change in salivary amylase in response to the intervention sessions, whether SRGI or lifestyle education. This null finding is consistent with prior findings in adolescents showing increases in salivary amylase only in emotional states of high arousal, but no change following emotions characterized as lower arousal, including relaxation. 40 There is also evidence that cortisol and amylase responses may be asymmetrical depending on past traumatic experiences in youth. 41 Further studies are warranted to investigate salivary amylase response to other types, durations, and depths of stress-reduction interventions, and to determine whether pre-existing characteristics of the study population may moderate amylase and other stress biomarker responses.
While acute reductions in stress and stress biomarker indicate a potent biological effect of the mind-body modality of guided imagery, it is unknown whether this translates to a benefit in stress reduction in the longer term. Whether acute changes in cortisol following brief bouts of stress reduction have any relationship to overall stress or stress biomarker patterns over time would be important to ascertain, given the past findings linking chronic life stress with obesity-related disease risk factors.10,42 Similarly, longer-term effects of stress management using GI on other health markers, whether biological or psychological, should be addressed.
Limitations of this report include the fact that this was a secondary analysis of intra-intervention outcomes related to a larger RCT intervention. As such, we combined 2 of the originally randomized groups (SRGI and LBGI) since they had to the point of analysis for this report (4 weeks into the intervention) received identical interventions of both lifestyle classes and stress-reduction guided imagery, thereby allowing for a larger GI group to compare to the lifestyle (LS) group. Combining these groups led to unequal numbers in the comparison groups (i.e., around twice as many in GI compared to LS), which was compounded by an unfortunate protocol deviation which led to the failure to assess cortisol and mood in many of the LS group participants. The resulting inequality of study group size presents a limitation in that greater standard errors due to a smaller sample size in the LS group may have limited the ability to detect the group differences. Another limitation relates to the generalizability of these findings outside of a predominantly Latino teenage population. In addition, while the absolute values we found for salivary cortisol values are in line with prior reports in children and adolescents, 43 testing for reductions in cortisol levels in the late afternoon, when levels are physiologically low, may reduce chances to detect differences in short term reductions. Future studies might address this by performing stress-reduction intervention in the late morning hours while cortisol levels are typically higher, yet beyond the potentially confounding effects of the cortisol awakening response. 43 Finally, our protocol measured cortisol responses only in weeks 3 and 4, preventing us from detecting longitudinal changes in response to the guided imagery in the GI group from weeks 1 and 2 which may have explained the unexpected similar reduction seen in cortisol within the GI group on weeks 3 and 4 whether receiving the lifestyle class or the guided imagery session.
In conclusion, we have shown that stress-reduction guided imagery delivered in group format significantly reduces salivary cortisol, and to a similar degree as that previously shown following individual guided imagery. SRGI also reduced acute stress mood, but did not have an effect on salivary amylase. Future studies will be needed to demonstrate potential longer-term effects of stress-reduction guided imagery on self-reported stress, stress biomarkers, and related health outcomes.
Footnotes
Conflicts of Interest
The authors have no conflicts of interest to report.
Financial Assistance
This work was sponsored by the NIH National Center for Complementary and Integrative Health (NCCIH), 1RO1AT008330. The study sponsors were not involved in (1) study design; (2) the collection, analysis, and interpretation of data; (3) the writing of the report; or (4) the decision to submit the paper for publication.