
Abstract
Background
The transition of young adults with type 1 diabetes (T1D) from pediatric to adult care is challenging and frequently accompanied by worsening of diabetes-related health. To date, there are no reports which prospectively assess the effects of theory-based psycho-behavioral interventions during the transition period neither on glycemic control nor on psychosocial factors that contribute to poor glycemic control. Therefore, the overall aim of this study was to develop and pilot test an integrative group intervention based on the underlying principles of self-determination theory (SDT), in young adults with T1D.
Methods
Fifty-one young adults with T1D participated in an education and case management-based transition program, of which 9 took part in the Diabetes Empowerment Council (DEC), a 12-week holistic, multimodality facilitated group intervention consisting of “council” process based on indigenous community practices, stress-reduction guided imagery, narrative medicine modalities, simple ritual, and other integrative modalities. Feasibility, acceptability, potential mechanism of effects, and bio-behavioral outcomes were determined using mixed qualitative and quantitative methods.
Results
The intervention was highly acceptable to participants, though presented significant feasibility challenges. Participants in DEC showed significant reductions in perceived stress and depression, and increases in general well-being relative to other control participants. Reduction in perceived stress, independent of intervention group, was associated with reductions in hemoglobin A1C. A theoretical model explaining the effects of the intervention included the promotion of relatedness and autonomy support, 2 important aspects of SDT.
Conclusions
The DEC is a promising group intervention for young adults with T1D going through transition to adult care. Future investigations will be necessary to resolve feasibility issues, optimize the multimodality intervention, determine full intervention effects, and fully test the role of the underlying theoretical model of action.
ClinicalTrials.gov Registration Number NCT02807155; Registration date: June 15, 2016 (retrospectively registered)
Background
The transition of young adults with type 1 diabetes (T1D) from pediatric to adult care is challenging and frequently accompanied by worsening of diabetes-related health. In particular, maintaining continuity of care and glycemic control has been shown to be difficult during the young adult years.1,2 We have recently shown that a structured transition program for young adults, Let’s Empower and Prepare (LEAP), successfully improved follow-up rates for transitioning youth and glycemic control as measured by A1C over a 1-year period. 3
It is essential to address psychosocial issues if one is to have a healthy transition from pediatric to adult care. 4 Among young adults with diabetes, psychosocial issues are known to adversely impact glycemic control. In particular, we have shown that in urban, predominantly Latino young adults, psychosocial stress clearly worsens glycemic control during this time, with the number of psychosocial stressors directly correlating with hemoglobin A1C. 5 This is in line with other, long-standing data suggesting that psychosocial stress adversely affects glycemic outcomes in T1D, likely through both direct physiological effects and effects on diabetes care behaviors.6,7
These findings suggest that there is considerable need for innovative interventions during the transition years that directly address emerging adults’ unique diabetes care needs, target reduction of chronic stress, and promote psychological well-being. To date, there are no reports which prospectively assess the effects of theory-based psycho-behavioral interventions during the transition period on glycemic control nor on psychosocial factors that contribute to poor glycemic control. Self-determination theory (SDT) is a promising theoretical approach for working with young adults with diabetes. This approach to human motivation posits that 3 innate human psychological needs form the basis for optimal self-motivation: competence, relatedness, and autonomy. 8 Support of these 3 needs predicts greater well-being in a variety of social circumstances. 9 SDT has been shown to be relevant to health behaviors involved in diabetes management. Specifically, in adults with diabetes: (1) autonomy support and autonomous motivation were associated with improved glucose control, 10 as well as greater dietary self-care and improved life satisfaction; 11 and (2) an SDT-based intervention showed that increases in autonomy support and perceived competence resulted in improved glucose control. 12
Although support groups have been shown to be somewhat effective in diabetes treatment of both adolescents and adults, 13 outcomes are still not optimal, and innovative modalities are needed to increase the effectiveness of such group interventions. Given that previous research in integrative medicine has shown that mind–body interventions such as mindfulness programs and guided imagery may be effective in reducing stress biomarkers in obese adolescents 14 and in improving outcomes in older adults with type 2 diabetes,15,16 incorporating these modalities into group interventions for young adults with T1D may enhance psychosocial, well-being, or metabolic outcomes in this population.
“Council” is a relational, facilitated group process based primarily on the decision-making and group communication processes used by indigenous and other cultures, for example, Native American, ancient Greek, and Quaker meetings. 17 In modern times, council has been used in the fields of psychology,18,19 social psychology, 20 and education, 21 including throughout the Los Angeles Unified School District which has a predominantly Hispanic/Latino student body. Council differs from a traditional support group in that there is an assumption of health and well-being rather than an assumption of pathology that requires support. Indeed, the word “empowerment” was chosen for the Diabetes Empowerment Council (DEC) specifically as a developmentally appropriate term which would appeal to young adults’ sense of seeking and striving for autonomy, rather than the word “support,” which might imply a level of victimhood with which the youth does not identify. The relational aspects of the council experience, that is, the connections between group members, are seen as critical in establishing a place of safety, trust, and comfort, from which change and healing can occur. Council is a relational practice which supports autonomous choice, acknowledges feelings, and promotes opportunities for self-direction, all important enhancers of intrinsic motivation according to SDT. 22
Therefore, the overall aim of this study was to develop and pilot test an integrative group intervention based on the underlying principles of SDT, in young adults with T1D participating in the 1-year long LEAP transition program. 3 The specific aims were to assess the feasibility and acceptability of the new intervention, to determine the potential mechanisms of action of the intervention effects through the use of qualitative methodology, and to explore the psychosocial and metabolic effects of the intervention.
Methods
This report represents a substudy of the Helmsley T1D Transition “LEAP” Program. 3 The LEAP study compared the effectiveness of a structured transition program, as compared to usual care, in improving clinical follow-up, glycemic control, and psychosocial well-being among young adults with T1D. A subgroup of participants in the structured transition program was invited to participate in the DEC and to represent the substance of this report. Written consent was signed by all participants. This study was approved by the University of Southern California Institutional Review Board.
Intervention Group Assignment
From the group of 51 participants who received the LEAP intervention, 2 separate waves of DEC were undertaken (Figure 1). The first 23 participants recruited into the LEAP program (wave 1) were randomized into DEC group versus non-DEC control group. Our intention was to similarly randomize the second wave of participants (n = 28). However, following randomization of wave 2 and inviting those selected for the DEC group to participate, it was clear that there were an insufficient number of randomized participants able to attend the DEC. We therefore abandoned the randomization and invited all wave 2 participants to attend the group, as it was more critical for the pilot study aims to carry out a nonrandomized intervention with an adequately sized group than to maintain the randomization but have an inadequate number of participants to appropriately deliver the intervention.
Intervention Group Assignments
To minimize selection bias, our analysis excludes participants initially randomized to the non-DEC condition in wave 1, as we considered that some may have elected to attend the DEC if given the option. Therefore, the control group consists of all participants who were invited to the DEC, but elected not to attend, that is, participants randomized in wave 1 to DEC who did not attend any sessions (n = 5), and all participants in the nonrandomized wave 2 who elected not to participate in the DEC (n = 23). A total of 12 participants elected to attend the DEC intervention, 7 in wave 1 and 5 in wave 2. Outcome data from 3 participants who attended only 1 or 2 DEC sessions were excluded prior to data analysis, as we considered this to be an inadequate “dose” of intervention to allow interpretation of any outcomes. Therefore, for this report, we compare the results of the participants who attended 5 or more of the 12 DEC sessions (“DEC Group,” n = 9) with participants who elected not to attend the DEC (“Control Group,” n = 28).
Diabetes Empowerment Council
The DEC met every 3 to 4 weeks for 12 sessions, with each session lasting 1.5 h. Sessions were held in the early evening from ∼6
The conduct of each council session involved the following intentions and processes
17
:
“The Circle.” The group sits in a circle, allowing all members to be easily seen and heard, and minimizing hierarchy among group members and facilitators. “Talking piece.” Only one member of the group can speak at a time. A stone, stick, or other designated personal object (the “talking piece”) is utilized to focus the communication, clearly identifying which group member holds the floor to speak. “Speak from the heart.” Members speak intentionally, with brevity and clarity, whatever is present and most important for them in the moment. “Listen from the heart.” When not speaking, all group members listen actively to each speaker. No cross talk or banter is permitted. All communications are held in utmost confidentiality.
Several integrative healing modalities were used within the context of the council circle. The modalities utilized were based on the training and experiences of the lead author (MJW), including (1) extensive personal use of council in work with youth at risk, adult men’s process groups, parent support groups, community building contexts, and formal trainings by Council in Schools leadership (coauthor JP); (2) certification in Interactive Guided ImagerySM through the Academy for Guided Imagery;
23
(3) diabetes discussion topics chosen through extensive experience as a pediatric endocrinologist; and (4) other creative modalities (storytelling, journaling, etc) used in extensive work as faculty in diabetes summer camp and other community-based work. Thus, the content of the activities within the council included the following:
Guided imagery. Group guided imagery, a complementary/integrative mind–body modality,
14
was conducted using prewritten standardized scripts following modifications of the standardized processes of individualized Interactive Guided ImagerySM.
23
Participants’ personalized mental images are used to promote health through several standardized, yet adaptable, techniques including relaxation/stress reduction, working through resistance to behavioral change, and empowerment through the activation of self-derived insight and inner resources. Following guided imagery exercises, participants shared their imagery experiences and insights within the council setting. Narrative medicine and storytelling. Some sessions were devoted to telling personal stories of life with diabetes, whereby the participants would share their own life experiences with each other, such as the time of their initial diagnosis, with the intention of learning from one another’s experience and practice. In addition, mythic storytelling was used to allow participants to relate their lives with diabetes to universal life themes covered in the mythic tale. Specifically, “Jumping Mouse,” a Native American tale of the heroic quest to full life expression,
24
was used in the council. Discussion topics, both general and diabetes-specific. LEAP curriculum topics were discussed, with focus on targeted diabetes care tasks, emphasizing the relevant life experiences of each individual. Topics could thus achieve greater relevance to group members through the depth of discussion, connection, and shared experience within the council format. While particular diabetes-related topics were brought in for discussion by the group facilitator, participants were also encouraged to bring in for discussion any topics that held importance for them in their lives as young adults with diabetes. The final content of the discussion for any given session was determined by which topics had the most salience and relevance for the participants in the moment. Poetry, drumming, interactive games, and journaling. A mixed variety of these methods were used to engage the youth in nondidactic methods of reflection, contemplation, and experiential learning. Simple ritual. Simple rituals were established to mindfully emphasize the ideas being discussed within the council. The use of the talking piece was the main ritualized action, to foster mindful, intentional communication. Other examples included the use of stones as talismans or memory pieces to emphasize or remember a particular poignant or impactful moment in circle and simple choreographed movement within the circle—for example, an individual stepping into the center of the circle to be addressed one at a time by other members, thereby receiving the recognition and acknowledgment of peers.
Qualitative Methods
Following completion of all DEC sessions, participants were invited to attend a focus group to share feedback regarding their DEC participation. Two focus groups, each lasting approximately 90 min, were conducted by a skilled facilitator (DSM) who had not participated in the DEC program. Focus groups were held on the same days and times as the DEC sessions had been offered, and participants were provided with transportation (taxi service) or travel reimbursement and a $25 gift card upon completion of the focus group session. Each focus group utilized a semistructured interview guide to elicit participants’ feedback regarding the DEC group process, organization, and logistics, as well as offering opportunities for open discussion of topics not covered in the interview guide.
Focus groups were audiotaped and transcribed by an independent contractor subject to a confidentiality agreement. Transcripts were analyzed using a qualitative descriptive approach. 25 Three researchers (MJW, EAP, and DF) independently coded each transcript, meeting biweekly over a 3-month period to discuss significant transcript passages, review codes, and identify emerging themes. This process continued iteratively until consensus was achieved among the research team. Once the team agreed upon the themes, one researcher (DF) extracted interview excerpts that supported each theme.
Quantitative Outcome Measures
The following self-report psychosocial measures were administered pre- and postintervention: the Perceived Stress Scale, 26 assessing an individual’s perception of life as stressful within the past month, adapted by increasing to 17 items and modifying wording to increase comprehension among urban Latino adolescents; 3 the Patient Health Questionnaire-9, a 9-item depressive symptom severity measure; 27 the General Well-Being Index, which has been used with participants as young as 14 years to measure psychological well-being; 28 the Arizona Integrative Outcomes Scales, 29 single-item visual analogue scales measuring a person’s global state of physical, emotional, and spiritual well-being in the preceding 24 h and 30 days; the Satisfaction with Life Scale, a 5-item global life satisfaction measure. Glycemic control was assessed by measuring hemoglobin A1C using the DCA 2000 analyzer (Bayer Inc, Tarrytown, NY).
Statistical Analyses
Baseline demographics in the DEC versus control groups were compared using t tests for continuous variables and Fisher exact tests for categorical variables. Changes in psychosocial variables from the baseline to 12 months were compared using t tests. For the purpose of this small pilot study, a P value of .1 was a priori set to indicate statistical significance. Effect sizes for the changes in the empowerment group versus the control group were expressed as Cohen’s d with 90% confidence intervals. Mixed-effects regression was performed to model A1C as a function of treatment group, time, and an interaction term of treatment group and time in order to assess the rate of change in A1C over the 12-month study period.
Results
Participant Demographics
Baseline Demographic Characteristics.
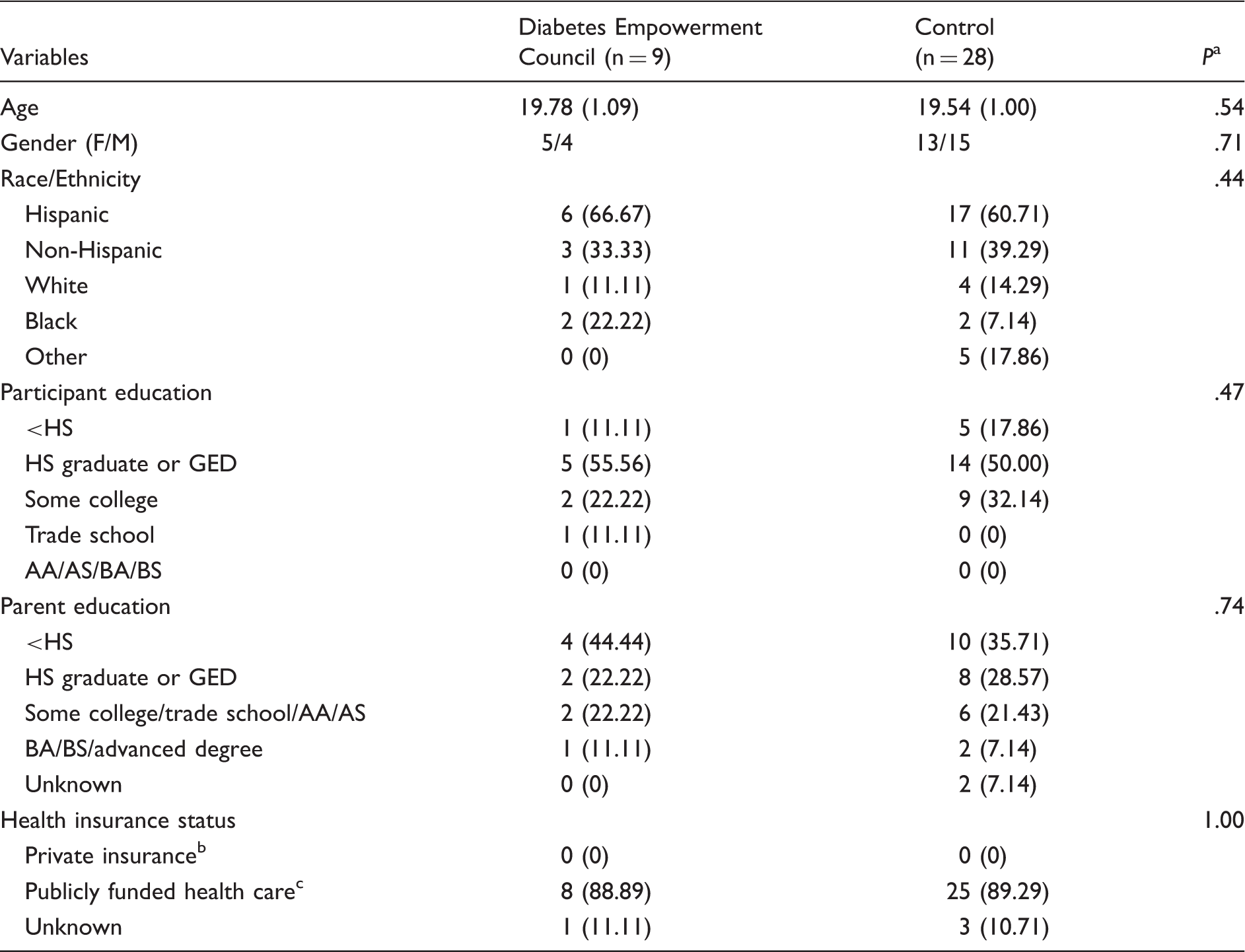
Abbreviations: AA, associate in arts; AS, associate in science; BA, bachelor of arts; BS, bachelor of science; GED, general equivalency diploma; HS, high school.
t test for age and number of sessions attended, Fisher exact test for all others.
Any private insurance, alone or in combination with public programs.
Public programs only (eg, MediCal, California Children’s Services) or uninsured.
Qualitative Results
Intervention structure
In total, 7 of the 9 DEC participants attended a focus group. Participants expressed satisfaction with the structure of the DEC sessions, including transportation, food, and scheduling. They noted that the text message reminders 2 days before the meeting and again the day of the meeting were helpful in facilitating their attendance. With respect to recruitment and reasons for participation, several participants noted that they were interested in the group because of its framing as an empowerment (vs support) group. To enhance future recruitment, they suggested including testimonials from previous participants in recruitment materials. Although participants noted that carryover of the DEC principles and concepts was strong, carryover of specific intervention activities outside the group was mixed. Passive intervention activities, such as carrying stones engraved with words that symbolized topics discussed in the group, had strong carryover, whereas activities that required ongoing active participation outside the group, such as journaling, had poor carryover, largely due to logistical barriers. Participants suggested that text message reminders may improve adherence to this aspect of the intervention.
Intervention process
Analysis of the focus groups led to a preliminary theoretical model of the DEC process and outcomes, as depicted in Figure 2. In this model, we hypothesize that the DEC structure and format strengthened participants’ motivation, self-acceptance, stress reduction, and relatedness, which in turn led participants to find new meaning and purpose in having diabetes, and incorporate new activities and behaviors into their daily lives. Relative to the 3 major SDT principles, we found support for the DEC changing relatedness and autonomy/motivation, but not competence. Our model additionally incorporates stress reduction, a construct not included in SDT, as a mediator of health behavior changes and other positive outcomes. Next we summarize findings related to each aspect of the DEC process and outcomes outlined in Figure 2. Supporting quotes from focus group participants are provided in Table 2.
Theoretical Model for DEC Process and Outcomes. Focus Group Participant Quotes. Abbreviation: DEC, Diabetes Empowerment Council.

Intervention format
Participants described 4 concepts as being central to the DEC: the use of ritual and talismans; guided imagery; poetry and storytelling; and the council principles as the overarching group process. Talismans (such as an engraved stone) served as tangible reminders of DEC principles and concepts that participants could easily integrate into everyday life, through carrying them in a pocket or backpack. Guided imagery was noted to be a valuable tool for stress management that participants used both during and outside of DEC sessions. Participants stated that the poetry and storytelling shared in the DEC helped them to explore different points of view related to living with diabetes. The council rules for group facilitation allowed everyone in the group to share their thoughts and be listened to intently, without pressure and expectations about what should be said. Relatedly, participants also valued the egalitarian structure of the DEC, an emergent finding not initially probed for in the interview guide. Health professionals and young people with diabetes participated as equals in the DEC, facilitating the autonomy of the young people, who noted that their previous interactions with health professionals were often characterized by unequal power relations.
DEC process and outcomes
The 4 major processes cited by focus group participants as leading to positive changes were increases in self-acceptance, stress reduction, relatedness, and motivation. Participants identified that these processes had led to participation in new activities and behaviors, as well as a new meaning and purpose associated with their diagnosis of diabetes. In contrast, competence in performing diabetes-related tasks was not strongly emphasized by participants as an outcome of the DEC intervention.
Self-acceptance
DEC participants expressed that the group had helped them feel more confident with respect to their diabetes care decisions. In addition, participants shared that they no longer saw diabetes as defining their identity. Finally, participants expressed an increased acceptance of diabetes management tasks as being an intrinsic part of everyday life.
Stress reduction
Several aspects of the DEC were cited as helping participants reduce stress, including guided imagery, storytelling, and sharing personal experiences. Further, several participants noted that they had been able to incorporate the stress reduction strategies learned in the DEC into their everyday lives.
Relatedness
Participants said that the DEC had both created positive relationships among the group members as well as strengthening their relationships with friends and family members. Relatedness was seen as enabling self-disclosure and social support among the DEC members. Within the DEC process, participants spontaneously requested a session where they could bring friends and family members to the DEC to talk about diabetes. Participants cited this session as being highly successful in enabling them to communicate effectively about the challenges and frustrations of living with diabetes.
Motivation
Participants expressed that the DEC had increased their motivation for diabetes self-care, as well as for dealing with other challenging life situations. Participants drew motivation from stories shared in the group, other participants’ experiences, and the knowledge that they were not alone in their struggles with diabetes and other life issues. Participants also cited the talismans as a tangible reminder of the DEC that could strengthen motivation during challenging situations.
New activities and behaviors
Although changing diabetes self-care behaviors was not an explicit goal of the DEC, some participants stated that they had become more consistent with checking blood glucose and taking insulin. Participants also reported performing self-care behaviors more consistently than before, using what they had experienced in the DEC as a resource when diabetes self-care was challenging.
New meaning and purpose
Participants stated that the DEC had helped them reframe the meaning of diabetes more positively than before. They also shared that the DEC led to their discovery of a newfound purpose to having diabetes. For example, many participants stated that participating in the DEC created a desire to help others with diabetes. Others said that the DEC had opened their eyes to work and career opportunities that were open to them because of diabetes. Overall, the DEC enabled participants to see positive ways that diabetes could contribute to their life meaning and purpose.
Quantitative outcomes
Psychosocial and Glycemic Outcomes.

Abbreviations: CI, confidence interval; DEC, Diabetes Empowerment Council; SD, standard deviation.

Relationship Between Change in A1C and Change in Perceived Stress.
Discussion
In this report, we describe the development of the DEC, a holistic, facilitated group intervention using multiple complementary/integrative modalities for young adults with T1D. We found that the intervention was highly acceptable to those who participated and led to significant reductions in stress and depression and increases in general well-being. Although the intervention did not lead to improvements in glycemic control, the overall association between reduction in perceived stress and A1C reduction supports the use of stress reduction modalities as a promising approach in youth with T1D.
The primary objective of this study was to determine the feasibility and acceptability of the intervention. It was clear that substantial feasibility issues must be overcome in order to deliver this intervention on a broader basis. The main problem with feasibility was getting the participants to attend the initial group meeting in the first place, and we found that young adult lifestyles made regular group attendance very difficult. Thus, difficulties with travel and generally extremely busy lives including college, work, and other demands, all present substantial barriers to adherence to group participation. The dropout rate of 3 participants of the original 12 who came to the DEC intervention is acceptable and comparable to other mind–body interventions in adult diabetic populations. 16 In addition, the qualitative data suggested that the DEC was highly acceptable to those who did participate in the intervention—that is, if they came, they liked it. Participants’ suggestions for strategies to overcome barriers to initial participation (eg, testimonials, more geographically desirable meeting locations, participant incentives) may improve feasibility in future trials.
Participation in the DEC markedly reduced depressive symptoms and perceived stress, with large between-group effect sizes for these key psychosocial factors. The decrease in depressive symptoms is notable, since depression was not a direct target of the intervention but has been long known to adversely affect glycemic control in diabetes.30,31 In contrast, stress was a direct target of the intervention through the use of the mind–body modality of stress-reduction guided imagery. We have previously shown that individually delivered stress-reduction guided imagery such as that used in the DEC can acutely reduce salivary cortisol levels in adolescents by more than 35%. 14 The stress reduction approach for diabetes is grounded in the long-standing literature implicating psychosocial stress as a contributor to poor glycemic and psychological outcomes in both adults and youth with T1D.32–36 Acute stress leads to neuro-hormonal changes of the coordinated stress response, including increases in cortisol and catecholamines, which promote elevation of blood glucose. 37 Reports have confirmed the role of family and psychosocial stressors on poor adherence to diabetes care behaviors, with a presumed secondary effect on glycemic control in adolescents.6,38,39 Others suggest that psychosocial stress may directly contribute to poor glycemic control in adolescents—that is, not solely through its effect on adherence to diabetes self-care. 7 Among LEAP study participants, we have documented an association between the number of stressful life events and glycemic control. 5 All these data suggest that stress reduction is a valid target for intervention in T1D to improve glycemic control, either through direct effects on stress physiology or indirectly by improving adherence to diabetes self-care behaviors such as increased home glucose monitoring or adherence to insulin therapy. 38
The importance of addressing stress and directly promoting stress reduction is further highlighted by our finding that independent of intervention group, a reduction in perceived stress was associated with a reduction in A1C. While this finding is not novel, it is to our knowledge the first time that longitudinal changes in stress and glycemic control have been shown to be related to a young adult diabetic population in transition. Although A1C was not significantly reduced in the DEC group relative to controls, there was a small effect (d = .33) seen in this direction, and this small study did not have the power to detect significant change on this outcome. However, even a statistically significant change of this magnitude, while comparable to that seen with some diabetes pharmaceuticals, would still not lead to an A1C in this population that approaches the clinical A1C target of 7% established by the American Diabetes Association. Future studies might therefore increase the dose of stress-reduction guided imagery and more strongly emphasize the home practice of stress-reduction guided imagery exercises in order to maximize the effect of stress management on glycemic control.
In addition to ameliorating the negative psychological symptoms of stress and depression, participation in the DEC improved general well-being among participants. This is important to note, given the World Health Organization’s definition of health as “a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity.” 40 The reason for discordance in our 2 separate measures of well-being is unclear, with improvement seen in general well-being, but none in the global well-being measure. Although both scales have been validated in healthy young adult populations, they have not to our knowledge been utilized in clinical samples such as in this study. Of note, we previously found that all participants who participated in the full LEAP intervention study did show improvements in the 1-month global well-being measure compared to controls, 3 and it is likely that this small study lacked the power to fully address this issue.
Our last objective was to assess the possible theoretical mechanism of action of the DEC intervention through the analysis of qualitative data. The a priori theoretical basis of the intervention was SDT as described by Ryan and Deci, 8 which suggests that competence, relatedness, 41 and support for autonomy are 3 key factors that can lead to health behavior change. Our focus group data strongly suggested that relatedness was increased in the DEC participants, while autonomy support also seemed important to the mechanism of intervention action. In contrast, competence for diabetes-related tasks was not strongly emphasized by participants. Thus, 2 of the 3 major factors leading to health behavior change, as posited by SDT, were positively impacted by DEC participation. Future studies with larger groups would be necessary to yield the power that would permit quantitative measurement of these effects in order to validate SDT as the underlying basis for the effects seen.
Of interest, participants commented that other aspects of the intervention beyond the stress-reduction guided imagery were perceived as reducing their stress, including the use of story telling, being able to trust the others in the group enough to tell their personal stories, and aspects of the council process itself. The mechanism whereby storytelling and council may lead to stress reduction is unknown, but may lie in the way that both can promote mindfulness. Mindfulness-based stress reduction has been clearly shown to have beneficial effects in multiple health conditions including reduction in stress.41,42 The nature of the council process in particular promotes deep mindfulness, as its ritualized mode of communication emphasizes mindful, purposeful speech, encourages deep listening, and promotes an attitude of nonjudgment and respect. The metaphoric use of mythic storytelling may stimulate the imagination and allow one to focus on the narrative of the story, permitting each listener to apply the metaphoric substance of the story to one’s own circumstance. 43 Finally, the narrative process of telling one’s own story and hearing others’ stories is potentially a powerful intervention strategy in diabetes, having previously been shown to facilitate acceptance and integration of diabetes into one’s identity, positive coping, and performance of self-management behaviors.44–46 Future studies of this intervention should assess mindfulness as a potential mediator of intervention effects.
The major strength of this study is that it adds to the extreme paucity of controlled studies of diabetes transition from pediatric to adult care. Our previous report of the full cohort that contained the subset addressed in this report is one of the few controlled trials reported. 3 One published study 47 failed to detect effects due to low number of participants, highlighting feasibility challenges in working with a young adult population, and a randomized clinical trial of a structured transition program is currently in progress. 48 Other strengths of this report include our use of mixed methods, which allow for a robust evaluation of both intervention processes and outcomes. The use of qualitative methods is particularly important in a small-scale pilot study, as qualitative findings may be used to generate hypotheses regarding potential intervention mechanisms and outcomes that can be further investigated in a larger trial. Finally, this is the first report of use of highly innovative, complementary-integrative healing modalities applied to a population of patients with diabetes. Complementary-integrative modalities in general are showing increasing use within the U.S. population, and an expanding evidence base suggests potential benefits for such approaches. 49 Thus, this report adds to the literature suggesting that mind–body interventions may have a role to play in the integrative treatment of patients with diabetes.
The major limitation of this study is that it is a small, nonrandomized pilot trial. We had to accept this limitation when our initial attempts to conduct this as a randomized trial failed. The small number of participants greatly limited the power to detect significant effects. Despite this, we did see significance in some of our outcomes, and the large effect sizes suggest that those persons who do seek out the group intervention may benefit over those who do not. These results clearly need to be verified in a larger randomized controlled trial. Another limitation was the holistic, multimodality nature of the intervention which makes it impossible to clearly determine which components of the intervention were leading to benefits and which were not. Clearly, future studies will need to address these limitations through the recruitment of larger study groups, overcoming the initial feasibility barriers, and optimizing the intervention components through the use of specific study designs selected to do so. 50 Finally, there may be limitations to the generalizability of the intervention. The participants in this study were primarily from racial/ethnic minority backgrounds, had low socioeconomic status, and accessed health care through publicly funded insurance and entitlement programs; the extent to which our findings are applicable to populations with differing demographic characteristics requires further investigation.
Conclusions
In conclusion, these pilot data suggest that the DEC, as a facilitative group process, was well-liked by young adults with diabetes and had the anticipated effect on group relatedness, a key construct of SDT. The DEC significantly reduced perceived stress, presumably through both direct (stress-reduction guided imagery) and indirect (feelings of safety and trust, mindfulness) mechanisms. Larger scale intervention is clearly needed to fully determine the effects of the intervention, tease out which components of the holistic intervention led to the effects and which were either neutral or counterproductive, and to fully test the role of the underlying theoretical model of program action in leading to intervention outcomes.
Footnotes
Acknowledgments
The authors would like to acknowledge the extensive assistance of Lucy Montoya, project manager for the LEAP Transition Program.
Authors’ Contributions
MJW: Study conceptualization and design, study conduct, and data analysis; EAP: Study conduct, data analysis, and manuscript revisions; CV: Statistical analyses; PS: Study design and study conduct; DSM: Focus group conduct and review, and manuscript review; DF: Focus group transcript analysis, manuscript review, and revision; MJ: Study conduct, manuscript review, and revision; JP: Consultant to study design (council process), manuscript review, and revision.
Ethics Approval and Consent
All participants signed informed consent forms to participate. This study was approved by the University of Southern California Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Helmsley T1D Transition “Let’s Empower and Prepare” (LEAP) Program (Leona M and Harry B Helmsley Charitable Trust #2010PG-T1D011; PI: AP); the funding body did not play a role in study design, analysis, or interpretation of data. At the time of this study, EAP was a KL2 Scholar awarded under the KL2 Mentored Research Career Development Award through Southern California Clinical and Translational Science Institute at USC Keck School of Medicine (NCRR/NCATS #KL2RR031991).