
Abstract
Objective
The aim of this article is to describe the consensus process used to develop an acupuncture intervention protocol for an NIH-funded pragmatic randomized controlled trial (PRCT) of acupuncture for the management of chronic low back (cLBP) in older adults (BackInAction).
Background
CLBP is among leading causes of disability worldwide: almost 33% of US adults 65 and older experience LBP. Acupuncture is effective for cLBP but there is no specific data on older adults. The National Institutes for Health (NIH) funded a PRCT of acupuncture needling for this population. An essential trial milestone was development of a consensus intervention protocol.
Methods
An Acupuncture Advisory Panel (AAP) was formed with nine members: two physician-acupuncturists, six licensed acupuncturists representing diverse work backgrounds, and an acupuncture researcher. We used a modified Delphi process that included provision of acupuncture trial data, survey data describing how each expert treats cLBP, three conference calls, and between-call email discussion.
Results
Lively and professional discussions led to a consensus intervention protocol for the BackInAction trial that included steps/staging of care, recommendations for parameters of care session length, number of needle insertion sites, insertion depths, needle retention times, recommended types of needles, both local and distal areas of the body to be treated, acupuncture point options, auricular point options, self-care options, and minimum number of sessions considered ideal.
Conclusion
Using a modified Delphi process, an expert AAP created a consensus intervention protocol for the PRCT of acupuncture needling for cLBP in patients 65 and older.
Background
Low back pain is among leading causes of disability worldwide, with both prevalence and burden increasing with age:1,2 almost 33% of U.S. adults 65 and older experience lower back pain (LBP). 3 Despite large investments in care for LBP, the health and functional status of Americans with LBP has deteriorated. Older adults with new primary care visits for LBP often have persistent symptoms, disability, and interference over 12 months of follow-up. 4 Those who filled 2 or more opioid prescriptions within 90 days had similar patient-reported outcomes as those who did not fill early opioid prescriptions. 5 Opioid related deaths in people 65 years and older increased 635% in the 15 years from 2001 to 2016. 6 Opioids are associated with increased disability, medical costs, subsequent surgery and continued opioid use. 7
A critical gap exists in the evidence on the safety and effectiveness of treatments for older adults with cLBP. 8 Burgeoning imaging rates revealing incidental pathology may place older adults at risk for inappropriate invasive treatments,9–11 persistent pain, and increased health care utilization. 11 Treatments that might be considered appropriate for younger adults may not be appropriate for older adults, given their greater prevalence of comorbidities with attendant polypharmacy. 12 Normal physiological changes of aging reduce tolerance of medications; older adults have substantially increased risk of adverse effects of commonly used LBP treatments and medications such as non-steroidal anti-inflammatory drugs (NSAIDs), 13 muscle relaxants, and opioids.4,9,13,14 Older populations have increased susceptibility to adverse events linked to opioids such as delirium, sedation, dizziness, confusion, pneumonia, constipation, nausea, falls and mortality. 5 In their guidelines on noninvasive treatments for LBP, the American College of Physicians (ACP) recommends acupuncture as one first line option for acute, subacute and cLBP, but there is no specific data on older adults.15,16 Given the interest of the U.S. Centers for Medicare & Medicaid Services (CMS) in knowing the value of acupuncture for cLBP in the Medicare population, they partnered with the National Institutes of Health (NIH) to issue a ‘Funding Opportunity Announcement’ (RFA-AT-19-005) to conduct a pragmatic randomized controlled trial (PRCT) of acupuncture needling for cLBP in older adults. We were funded to conduct the PRCT which included a planning year funding to prepare for conducting the study. An essential planning year milestone was development of an acupuncture intervention protocol. This manuscript describes both the protocol and its process of development.
Acupuncture for cLBP and Medicare Population
Acupuncture has been found effective for chronic pain in adults, including for cLBP wherein the benefits persist over time.17,18 A large individual patient data meta-analysis found 85% of acupuncture benefit was maintained in 12 months of follow-up.17,18 While not able to compare effectiveness between specific styles of acupuncture, most reviewed studies applied traditional East Asian medicine (TEAM) principles based in the recognition of acupuncture channels and points.18,19 Yet no trials to date have focused solely on cLBP in the Medicare population. While acupuncture is recommended by the ACP and recognized by the NIH for cLBP, it has not been routinely covered by Medicare and has been unavailable to most adults 65 and older. On January 21, 2020 the Centers for Medicare & Medicaid Services (CMS) announced a decision to cover acupuncture for cLBP in Medicare recipients with limits on number of visits per year and stipulations on who may provide and directly bill for acupuncture care, effective January 2021. 20
Methods
We identified subject matter experts with input from each trial site’s investigators. Suggested experts were contacted by email or telephone. The resulting Acupuncture Advisory Panel (AAP) included nine expert members: two physicians and six licensed acupuncturists representing diverse practice backgrounds and experience including work with underserved populations at Federally Qualified Health Centers (FQHCs), practice in university clinics, in integrative health systems and in leadership roles. One member is medical director of a holistic medicine network, another is dean at an acupuncture college, and another is an acupuncture researcher with multiple acupuncture trials and publications on acupuncture treatment for cLBP. We used a modified Delphi process to develop the acupuncture intervention protocol to be used in the IRB-approved study design.
Modified Delphi Process
Researchers have adapted the Medical Research Council’s guidance of 2000 21 and 2008 22 in developing and evaluating complex interventions that have interacting components. 23 The process of forming a consensus-based intervention protocol, sometimes called manualization23–25 describes one such adaptation that seeks to strike a balance between standardization and flexibility in acupuncture research 24 for trials on depression, 26 stroke,27,28 and chronic pain.23,25,29 The Delphi process, developed by the Rand Corporation, is widely used for convergence of expert opinion within certain topic areas. 30 It is part of the development of research protocols and manuals 31 and typically involves a formal process of using questionnaires to gather information from experts, summarizing areas of consensus and reviewing with experts one or more times until consensus is obtained. Consensus is defined as general agreement from group discussion resulting in clear support for each item. Ours is described as a ‘modified’ Delphi process wherein acupuncture had already been studied in trials and established in guideline recommendations for cLBP. Collating that knowledge from the literature with our experts’ experience was the particular task of our panel to specify acupuncture for cLBP in people 65 and older.
Preliminary Information From Trials of Acupuncture for cLBP
To contextualize our acupuncture intervention in the existing trial literature, and to prepare the AAP members for discussion, we created a table of parameters from published acupuncture trials for cLBP that included: number of sessions, number of needles, needle retention time, description of the needles, local and/or distal acupoints required, optional points if permitted, and whether ‘de qi’ was sought.32–45 Additionally we added the same data published by experienced Chinese acupuncturists practicing in the US detailing their treatment approach for cLBP in patients 65 and older. 46 This background gave us information on key acupuncture intervention parameters, frequency and intensity of treatment interventions reported in the literature. Panel members were invited to complete a survey for the intervention parameters and details that reflected their approach to treatment of cLBP in people 65 and older.
Initial Questions for the AAP
Prior to our first conference call (October 29, 2019), we emailed our AAP members (Oct 10, 2019) and asked them how they treated cLBP in general and with older adults (see Table 1).
AAP Survey Questions and Consensus on First Call.

*Question raised at first call, but not on survey.
All AAP members responded prior to the first conference call and their responses were collated in a separate table and disseminated to facilitate comparisons between experts.
Consensus Topics
The first AAP conference call consisted of introductions, an overview of the trial, a brief summary of the role and responsibility of the AAP, an explanation of the consensus intervention process, orientation to STRICTA guidelines (Standards for Reporting Interventions in Clinical Trials of Acupuncture), 47 a review of the AAP members’ responses, and a discussion of essential consensus topics. Those are listed in Table 1.
Our first meeting found consensus on most topics (steps/staging of care, recommendations for parameters of care including palpation, session length, number of needle insertion sites, insertion depths, needle retention times, recommended types of needles, that both local and distal areas of the body be treated, obtaining ‘de qi’, inclusion of ‘ah shi’ points (tender points sensitive to palpation), and self-care options (to be named) considered ideal. We clarified topics that would require ongoing discussion: acupuncture point options, auricular point options and ideal minimum number of sessions recommended to achieve clinical benefit (Table 2). Topics agreed on would be reconfirmed in the next call where we would then focus primarily on acupuncture point options.
AAP Second Call and Consensus.

In preparation for the 2nd conference call, the AAP members were asked to review the point list created from the acupuncture trials for cLBP, as well as the AAP members’ survey responses. Survey topics included: would you omit any of the points listed and were there any omissions of useful points that should be included?
The second AAP conference call occurred on November 5, 2019 with discussion and confirmation of consensus topics from the first meeting. Discussion turned to creating and confirming a list of acupuncture point options. A list was built and circulated after the call for further consideration over email.
Email Communication Between Second and Third Conference Call
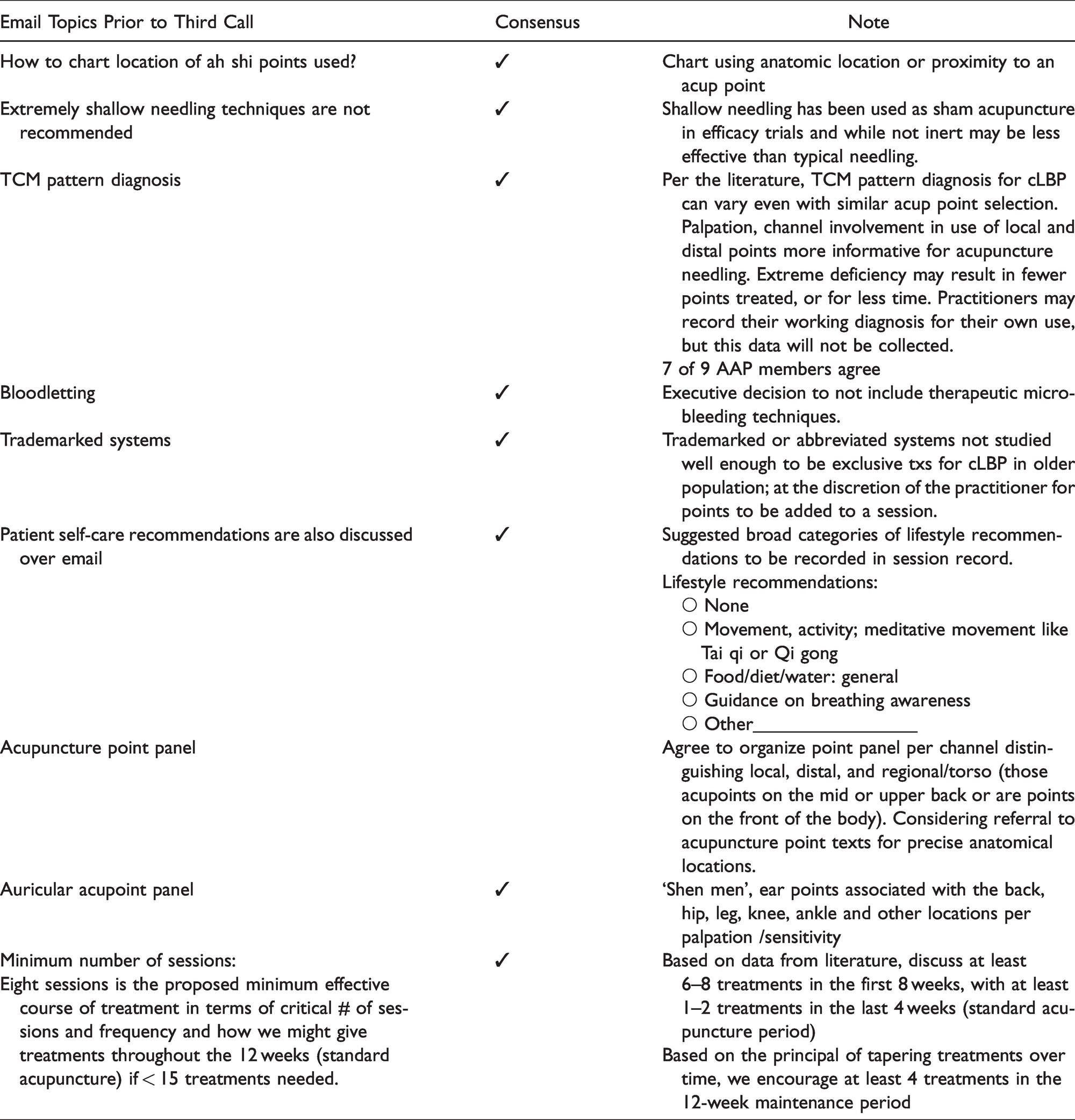
Acupoints to include continued to be discussed over email. Consensus intention was to include primary points from trials but also points that have been utilized in textbooks and by panel experts. Because patient presentations vary and treatments are expected to vary over time as a patient’s conditions improves, a panel of point options is ideal to support a practitioners versatility in individualizing care. Table 3 lists the topics in email discussion between the 2nd and 3rd conference call.
Email Topics Between Second and Third Call Informed Third Call Topics 11/26/2020.
Acupuncture Point Options
As described above, the AAP discussion of acupoint options was informed by multiple considerations: a table of information about treatments from acupuncture trials for cLBP that included local and/or distal acupoints used and optional points if permitted; acupoints from an article by seven experienced Chinese acupuncturists practicing in the US, treating cLBP in patients 65 and older, and results from our survey of each AAP member that included acupoints they use for cLBP (see Table 1). The discussion acknowledged the large number of suitable acupoints for treating cLBP, creating a range of relevant options. The decision was made to include all acupoints on the low back, including the Bladder and ‘Du’ channel acupoints, ‘Hua tuo jia ji’ and ‘extra’ points as well as indicated points on the back of the leg and selected points on the upper back and the ears.
The acupoint options are listed in the grid in the draft session form Appendix 2. The AAP agreed that point selection is at the discretion of the practitioner, with 6–20 insertion sites per session and expectation of both local and distal point needling. As a pragmatic trial, acupuncturists are expected to individualize a treatment as they would in real world clinical settings from within the protocol options. ‘Ah shi’ points and points not in the protocol list can be used with provision of rationale. Fidelity to the intervention protocol will be assessed using data from the session form, draft attached as Appendix 2. Acupuncturists may indicate if other aspects of acupuncture therapy not included in the trial (for example, moxibustion/application of heat, Ba guan (cupping), Tui na, Gua sha, electrical stimulation, herbal medicine) would have helped a particular participant, in their opinion.
Our intervention protocol proscribes microsystem or exclusively using trademarked treatments. It is acceptable to incorporate a point or two from any system into the consensus intervention, with rationale. While some texts recommend intentional micro-bloodletting of certain points for cLBP as a feature of acupuncture needling, this method is proscribed in this trial.
Self-Care Recommendations
In addition to the panel of acupuncture points, self-care recommendations elicited the most discussion for the AAP. Such recommendations are an essential aspect of acupuncture therapy and are engaged as a means of sustaining benefits from a session. These typically include recommendations on breathing, movement, temperature and other aspect of food, sleep, work and so on, as well as attitude and regard for oneself and others. The following were suggested for discussion.
Avoid excessive cold and sour food and drink. Avoid extreme exercise or work, lifting or twisting. If there is a sense one can increase exercise already engaged in, increase in small intervals. Or suggestion of meditative movement like Qi gong or Tai qi. Eat regular warm cooked meals. Drink enough water. Guidance on breathing awareness. Recommendations re: meditation or quiet reflective time in the day.
AAP agreed on need for inclusion of basic recommendations within the paradigm of classical Chinese medicine, or Traditional East Asian medicine as they would be given in real word setting. However, AAP members would have preferred more detail in the post-session recommendations. With an understanding of this as a PRCT, allowing acupuncturists to respond to patient questions and provide self-care information on breathing, increasing kinds of exercise, temperature of foods, sleep hygiene, work and activity as well as mental outlook was considered important. However, collecting data on self-care would best be done in general categories. We decided to use lifestyle recommendations categories collected in a previous trial (see Table 3).
Traditional Chinese Medicine Pattern Diagnosis
‘Diagnosing’ in traditional East Asian medicine (TEAM) acupuncture can blend paradigms from a description of locations (channels, areas of body, levels or depths, organs) to the status of substances (Qi, Blood, Fluids, Food) to Ba gang bian zheng (eight parameters: outside/inside; hot/cold; excess/deficiency; yang/yin), to TCM differentiating patterns of disharmony.49,50 These provide a context for clinical decision making where ‘patterns’ are secondary to the practical interactions of acupuncture practice. 51
Acupuncturists simultaneously treat and evaluate patients during a treatment visit by assessing how a patient responds to various stages of treatment from palpation to needling to other manual interventions that in turn inform the depth and direction of a disorder. Here evaluation is treatment and treatment is evaluation. 52 Signs and symptoms including tongue and pulse may change within a session, informing a responsive acupuncture approach. With an herbal medicine approach, one might look to patterns of disharmony and changes in symptoms, tongue etc. over time. With acupuncture therapies such changes can happen within a session and over time.
Responses within a session provide immediate and relevant information on the morphology of a presenting problem including location, type, quality, inherent waxing and waning of symptoms particularly with musculoskeletal problems like cLBP. While aspects of ‘patterns’ provide an essential context, they are not the primary determinant in choosing acupuncture points or combinations of points. It is also important to note that a TCM diagnosis, if made, is not typically written in the medical record in China. 51 Rather, signs and symptoms, acupoints treated, therapies applied, tests ordered and herbal prescriptions, if given, are recorded. A pattern ‘diagnosis’ can vary among practitioners for the same patient, while the acupoints chosen might be similar whatever the diagnosis.
This does not mean that TCM patterns are irrelevant, rather, TCM diagnosing should not be confused with the reductionist operation of Western medical diagnosing but is a flexible working assessment in a medical paradigm that assumes the only constant is change. 51 No consensus exists regarding TCM pattern diagnosis for cLBP when using acupuncture.34,53 Where acupuncturists may agree on diagnosis they can vary substantially in treatment recommendations. 54 Our trial acupuncturists are encouraged to engage and record the process they use in practice but the AAP agreed to not focus on or capture TCM diagnoses in this trial. 34
Additional Questions
The trial Steering Committee developed the inclusion/exclusion criteria; the AAP was consulted regarding the need for any acupuncture-specific inclusion/exclusion criteria. The AAP recommended a minimum effective course of treatment would include at least 8 visits. This is consistent with other sources, 17 that emphasize specific dosage in treatment including for a population likely managing multi-morbidity. 45 The AAP also concurred on the qualifications of the acupuncturists in our trial (as detailed in the next section).
Trial Acupuncturists
Trial acupuncturists will be state licensed and qualified to practice acupuncture in the state where care will be provided. At least 5 years clinical experience post-licensing is preferred with experience in treating older adults with cLBP having multi-morbidities. Exceptions for three years’ experience per individual applicant may be permitted. Trial acupuncturists will have an orientation to the trial and safety review.
Orientation for Trial Acupuncturists
All study acupuncturists will be required to complete provider training, which will include an orientation to the trial, pertinent trial logistics, the consensus intervention protocol and a review of safety for acupuncture needling in patients 65 and older.
Discussion
Establishing expert consensus protocols for complex interventions with interacting components, such as acupuncture therapy, especially for PRCTs, has replaced simple formulaic protocols used in earlier acupuncture efficacy RCTs. The Delphi process, developed by the Rand Corporation, is widely used for convergence of expert opinion 30 that seeks to strike a balance between standardization and flexibility in acupuncture research 24 for trials on depression, 26 stroke,27,28 and chronic pain.23,25,29
Delphi processes for acupuncture trials have varied. A trial for acupuncture as a complex intervention for depression preselected 52 characteristic components of treatment used in trials and then asked 15 expert practitioners to rate them in a survey. 26 A trial of acupuncture for assisted fertility used 3 rounds of survey questionnaires. 31 A trial of acupuncture for stroke rehabilitation blended structured planning meetings with experts and protocol questionnaires. 27 A large trial of acupuncture for chronic pain in an underserved population used multiple expert panel discussions without the use of surveys. 23
Our process is unique in several ways. First, our intervention protocol is for a PRCT, albeit limited to acupuncture needling compared to usual care. Also unique is that we provided our panel with treatment intervention information from prior trials of acupuncture for cLBP. We then used both survey information from our expert panel as well as conference call discussions to find consensus on topics and reconfirm them in subsequent calls. This process mixed the best features of ‘time needed to think’ in responding to survey topic questions, and the lively and professional discussions with the AAP members that built not only a consensus protocol, but a sense of team commitment to the project. Tables 1 to 3 illustrate consensus building as an iterative process representing compromise from individual opinions toward collective agreement. The intervention protocol is attached as Appendix 1.
Pilot Study of Processes
The consensus intervention was then used in a pilot trial at 2 of our 4 health system sites. This process provided direct feedback from pilot acupuncturists on possible tweaks to the protocol, which were then taken back to the AAP for discussion and confirmation. The final consensus intervention was used to refine our training orientation for acupuncturists employed in the trial, along with a review of safety in terms of potential issues with an older population, multi-morbidities and infection control. The draft acupuncture visit form is included as Appendix 2.
While use of modified Delphi processes are established as a feasible means for obtaining consensus on an intervention protocol for acupuncture RCTs and PRCTs, future Delphi processes might benefit using previous trial information, expert surveys as well as well as either in person or conference call meetings for a certain team building in the process of arriving at consensus.
Conclusion
Using a modified Delphi process, an expert AAP created a consensus acupuncture intervention protocol for a pragmatic randomized controlled trial of acupuncture needling for cLBP in patients 65 and older. The consensus protocol options provide a balance between standardization and flexibility in allowing acupuncturists to customize a session to a participant’s specific presentation of cLBP and as it evolves over time.
Supplemental Material
sj-pdf-1-gam-10.1177_21649561211007091 - Supplemental material for Acupuncture Intervention Protocol: Consensus Process for a Pragmatic Randomized Controlled Trial of Acupuncture for Management of Chronic Low Back Pain in Older Adults: An NIH HEAL Initiative Funded Project
Supplemental material, sj-pdf-1-gam-10.1177_21649561211007091 for Acupuncture Intervention Protocol: Consensus Process for a Pragmatic Randomized Controlled Trial of Acupuncture for Management of Chronic Low Back Pain in Older Adults: An NIH HEAL Initiative Funded Project by Arya Nielsen PhD Laura Ocker LAc, MAcOM Iman Majd MD, MS, LAc Jeff A Draisin MD Katherine Taromina CACM, LAc in Global Advances in Health and Medicine
Supplemental Material
sj-pdf-2-gam-10.1177_21649561211007091 - Supplemental material for Acupuncture Intervention Protocol: Consensus Process for a Pragmatic Randomized Controlled Trial of Acupuncture for Management of Chronic Low Back Pain in Older Adults: An NIH HEAL Initiative Funded Project
Supplemental material, sj-pdf-2-gam-10.1177_21649561211007091 for Acupuncture Intervention Protocol: Consensus Process for a Pragmatic Randomized Controlled Trial of Acupuncture for Management of Chronic Low Back Pain in Older Adults: An NIH HEAL Initiative Funded Project by Arya Nielsen PhD Laura Ocker LAc, MAcOM Iman Majd MD, MS, LAc Jeff A Draisin MD Katherine Taromina CACM, LAc in Global Advances in Health and Medicine
Footnotes
Acknowledgment
We thank Lynn DeBar, PhD for attending several meetings and Danielle Katsman for administrative assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (NIH) through the NIH HEAL Initiative under award number UG3/UH3 AT010739 from the National Center for Complementary and Integrative Medicine. This work also received logistical and technical support from the PRISM Resource Coordinating Center under award number U24AT010961 from the NIH through the NIH HEAL Initiative. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or its HEAL Initiative.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.