
Abstract
Background and Objective
Mind-body interventions (MBIs) have been shown to be effective individual-level interventions for mitigating physician burnout, but there are no controlled studies of yoga-based MBIs in resident physicians. We assessed the feasibility of a yoga-based MBI called RISE (resilience, integration, self-awareness, engagement) for residents among multiple specialties and academic medical centers.
Methods
We conducted a waitlist controlled randomized clinical trial of the RISE program with residents from multiple specialty departments at three academic medical centers. The RISE program consisted of six weekly sessions with suggested home practice. Feasibility was assessed across six domains: demand, implementation, practicality, acceptability, adaptation, and integration. Self-reported measures of psychological health were collected at baseline, post-program, and two-month follow-up.
Results
Among 2,000 residents contacted, 75 were assessed for eligibility and 56 were enrolled. Forty-four participants completed the study and were included in analysis. On average, participants attended two of six sessions. Feasibility of in-person attendance was rated as 28.9 (SD 25.6) on a 100-point visual analogue scale. Participants rated feasibility as 69.2 (SD 26.0) if the program was offered virtually. Those who received RISE reported improvements in mindfulness, stress, burnout, and physician well-being from baseline to post-program, which were sustained at two-month follow-up.
Conclusion
This is the first controlled study of a yoga-based MBI in residents. While the program was not feasible as delivered in this pilot study, initial analyses showed improvement in multiple measures of psychological health. Residents reported that virtual delivery would increase feasibility.
Introduction
Physicians experience high rates of stress, depression, and burnout, a work-related syndrome characterized by increased emotional exhaustion, increased depersonalization, and reduced personal accomplishment. 1 Burnout is associated with medical errors, professionalism issues, career attrition, substance use, and suicidal ideation.2–6 For many physicians, these symptoms rise during medical school and peak during residency, with a prevalence of approximately 51% among medical residents 7 and 69% among surgical residents. 8
Importantly, because of impact on clinicians and the health care system, the Quadruple Aim, developed by the Institute for Health Care Improvement to optimize health system improvement, emphasizes that physician well-being is an essential part of any health care reform. 9 Both individual- and organization-focused interventions offer clinically meaningful benefit in reducing physician burnout. 10 Successful individual interventions include stress management and mind-body interventions (MBIs).10–13 MBIs often incorporate mindfulness, or the ability to dispassionately observe the experience of the present moment with non-judgmental openness; an example of a standardized intervention is mindfulness-based stress reduction (MBSR).14–17 Yoga is a mind-body practice that not only incorporates the quality of mindfulness and formal meditation practice, but also physical postures, breath regulation, and relaxation. Evidence suggests the yoga component of MBSR may be the most crucial element for improving psychological well-being.18,19
The Kripalu Center for Yoga & Health developed the yoga-based program, RISE (resilience, integration, self-awareness, engagement), for professional populations. RISE has been studied in frontline professionals in single-arm and controlled designs.20–24 In a study with attending physicians, improvements in burnout, professional fulfillment, interpersonal disengagement, stress, resilience, anxiety, and depression were observed at post-program, and interpersonal disengagement, resilience, and mindfulness at two-month follow-up. 24
Given the demanding nature of training, there is great interest in evaluating the feasibility and efficacy of MBIs for the resident physician population. The primary aim of the present study was to assess the feasibility of providing a yoga-based MBI, RISE, for residents among multiple specialties in the academic medical center setting. As a secondary aim, the efficacy of RISE on measures of psychological health was explored.
Institutional Review Board
This study was approved by the Partners HealthCare Institutional Review Board.
Methods
Settings, Participants, and Study Design
During 2018 and 2019, residents were recruited from programs based at Brigham and Women’s Hospital, Beth Israel Deaconess Medical Center, Boston Children’s Hospital, and Harvard combined residency programs. Two cohorts of the study were conducted at the same time each year; fall of the academic year (September through November) was selected to allow new residents to settle in after starting in July and avoid holiday vacations. Residents were contacted by e-mail distribution lists and via residency program directors and graduate medical education (GME) offices. Paper fliers were placed in workrooms and common areas. Fellows were excluded from the study; residents were excluded if they had practiced a mind-body technique for more than 25 hours in the past six months. All participants, in both the intervention and control groups, provided informed consent and received a $25 gift card. This study was registered on ClinicalTrials.gov as NCT03687450.
Intervention
Developed by Kripalu Center for Yoga & Health, RISE is a program of yoga-based practices (Supplementary File S1). The program was delivered at the academic medical center as 60-minute weekly sessions over a six-week time period. 24 The instructor was a psychologist and certified yoga instructor (E-RYT 500). Sessions contained a combination of didactic and experiential material. Participants had access to online resources that reinforced content and were asked to maintain a daily home practice. The waitlist control group received one session at the end of the study period, which included an overview of didactic material and practices.
Data Collection
Surveys were administered using REDCap software. Feasibility was assessed post-program (at six weeks). Psychological measures were assessed at baseline, post-program, and two-month follow-up. Attendance was kept by the instructor at each session. Participants kept daily home practice logs.
Outcome Measures
At baseline, all participants completed a questionnaire about demographics and current mind-body practices (Supplementary File S2).
Feasibility was assessed according to six dimensions as described in recommendations for the design of feasibility studies from the National Cancer Institute, 25 utilized in other studies of mind-body interventions:26–28 1) demand, 2) implementation, 3) practicality, 4) acceptability, 5) adaptation, and 6) integration. Demand was qualitatively assessed informally in the local environment. Implementation was operationalized as the extent to which the program could be delivered and included weekly class observation. Practicality was determined by monetary costs, attendance, and extent of home practice. Acceptability was assessed through participant evaluation of RISE based on a visual analogue scale from 0 (not at all feasible) to 100 (very feasible). Adaptation was operationalized as modifications made to RISE to accommodate residents’ unique needs, such as long, irregular work hours and limited transportation options. Integration was operationalized as participant use of skills outside of sessions and during follow-up. Additional evaluation of feasibility by participants was obtained by questionnaire at post-program follow-up (Supplementary File S3).
Preliminary efficacy was assessed via self-report measures of psychological health at baseline, post-program, and two-month follow-up. Surveys included the Five Facet Mindfulness Questionnaire (FFMQ; short form, 15 items),29,30 Resilience Scale (RS-14; 14 items), 31 Perceived Stress Scale (PSS; 10 items), 32 Maslach Burnout Inventory (short form, 2 items),33,34 Professional Fulfillment Index (PFI; 16 items), 35 Patient Reported Outcomes Measurement Information System (PROMIS) Depression and Anxiety (short form: depression-4, anxiety-4),36–38 PROMIS Sleep Disturbance (short form, 4 items),39,40 and Resident Well-Being Index (7 items). 41
Analysis
Feasibility was reported utilizing the multidimensional approach described above; participant comments were grouped and reported according to the relevant domain of feasibility, determined by authors J.L. and N.D. For quantitative measures, within group changes were analyzed via paired samples t-tests and between group changes were analyzed via one-way ANOVAs. For questionnaires administered at one timepoint, descriptive data were calculated and presented. SPSS 24.0 was used for data analysis (IBM Corp, Armonk, NY).
Results
Participants
Approximately 2,000 residents were contacted by recruitment methods described above. Seventy-five residents and fellows responded to advertisements and were assessed for eligibility. Fifty-six residents met eligibility criteria and were enrolled; participants were randomized 2:1 using a random number generator to intervention (n = 38) vs. control (n = 18) (Figure 1). Of the 56 residents who enrolled and completed baseline measures, 43 completed post-program measures and 42 completed two-month follow-up. Participants who completed baseline and at least one follow-up assessment were included in analysis (Figure 1).
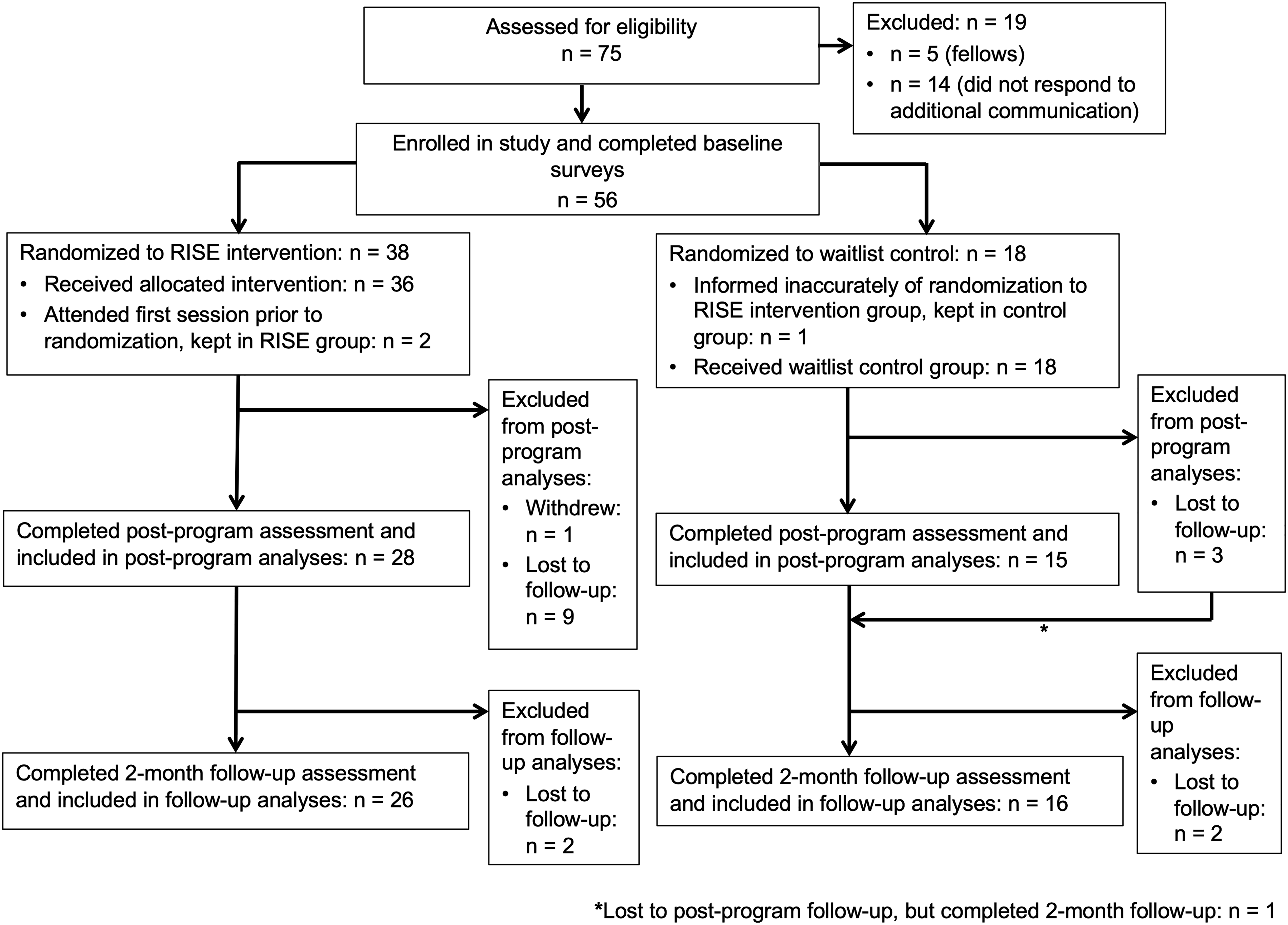
CONSORT Flow Diagram.
Both the intervention and control groups had a mean age of approximately 29 years; the majority of participants were female (Table 1). Almost half of participants self-identified their racial background as white. Internal Medicine residents comprised approximately half of the study sample. There was a fairly even distribution across training years. Baseline practice of mind-body techniques is described in Table 1. There were no statistically significant differences in demographic variables between groups (all p values > .05).
Characteristics of study sample (participants who completed baseline and any follow-up surveys).
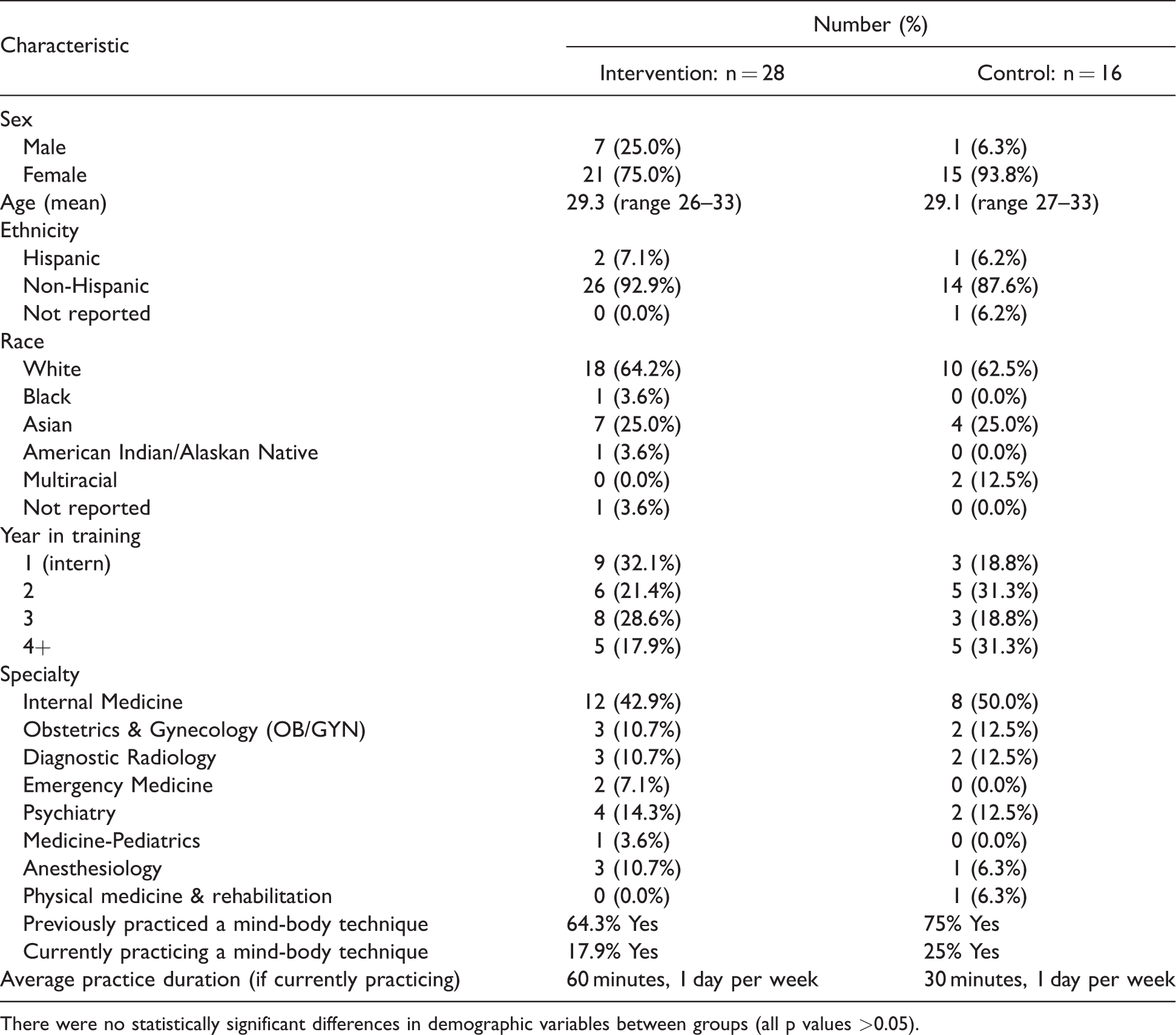
There were no statistically significant differences in demographic variables between groups (all p values >0.05).
Feasibility
Demand
Most residency program directors who were contacted responded positively and communicated their support of the study; there were no program directors who negatively responded to inquiries. One program protected their residents’ time to attend sessions.
Implementation
Sessions were held in hospital conference rooms at no cost with chairs that could be moved to place yoga mats (stored on-site). None of the sessions were cancelled or truncated. Authors J.L. and M.L.S. observed weekly classes to ensure quality.
Adaptation
RISE was delivered as six 60-minute weekly sessions. 24 Sessions were held on hospital premises to improve access for residents working different types of shifts and occurred Thursdays 6:00-7:00 PM, chosen based on a prior informal survey of residents.
Practicality
On average, participants attended a mean of 1.93 in-person sessions (SD = 1.52). Six (25%) attended no sessions, 21.4% attended one session, 17.9% attended two sessions, 17.9% attended three sessions, 14.3% attended four sessions, and 3.6% attended five sessions. No participant attended all six sessions. Participant reasons for missing RISE sessions were attributed to work schedule (89%), vacation (10%), or illness (1%).
At post-program follow-up, 74.1% of RISE participants reported they were using online RISE resources for home practice, with 75% using resources some days of the week and 25% more than half of the days of the week.
Acceptability
Participants rated the feasibility and acceptability of attending RISE as low, mean (M) = 28.9, standard deviation (SD) = 25.6, but rated it higher if offered multiple times per week, M = 63.2 (SD = 20.9), or online, M = 69.2 (SD = 26.0). If RISE was delivered by residency program, 48.1% of participants said it would have improved attendance; acceptability is summarized in Table 2.
Participant comments: acceptability, integration, and adaptation.

Integration
At two-month follow-up, 44% of the intervention group reported they had practiced RISE techniques 1.9 days per week (range 0–6 days; SD = 1.93) for 13.0 minutes (range 0-60 min; SD = 15.78) per occurrence. Participants used online resources and incorporated techniques into daily life (Table 2).
Preliminary Efficacy
Means and standard errors of psychological health measures for RISE and control groups at baseline, post-program, and two-month follow-up are displayed in Figure 2(A) and (B). Within-group analysis revealed that the RISE group improved in resilience, [t(27) = 2.66, p = . 013, d = 0.50], mindfulness (t(25) = 6.15, p = .0001, d = 1.21], stress [t(26) = −2.68, p = .013, d = .52), sleep disturbance [t(25) = −2.64, p = .014, d = .52], work exhaustion subscale of the PFI [t(19) = −4.66, p = .001, d = 1.04], interpersonal disengagement [t(25) = −2.01, p = .050, d = .39], total burnout [t(24) = −3.08, p = .021, d = .48], and physician well-being [t(25) = −2.56, p = .017, d = .50] from baseline to post-program. There was no improvement (p < 0.08) in depression [t(24) = −2.04, p = .073, d = .37]. There were no improvements in psychological health measures from baseline to post-program within the control group.
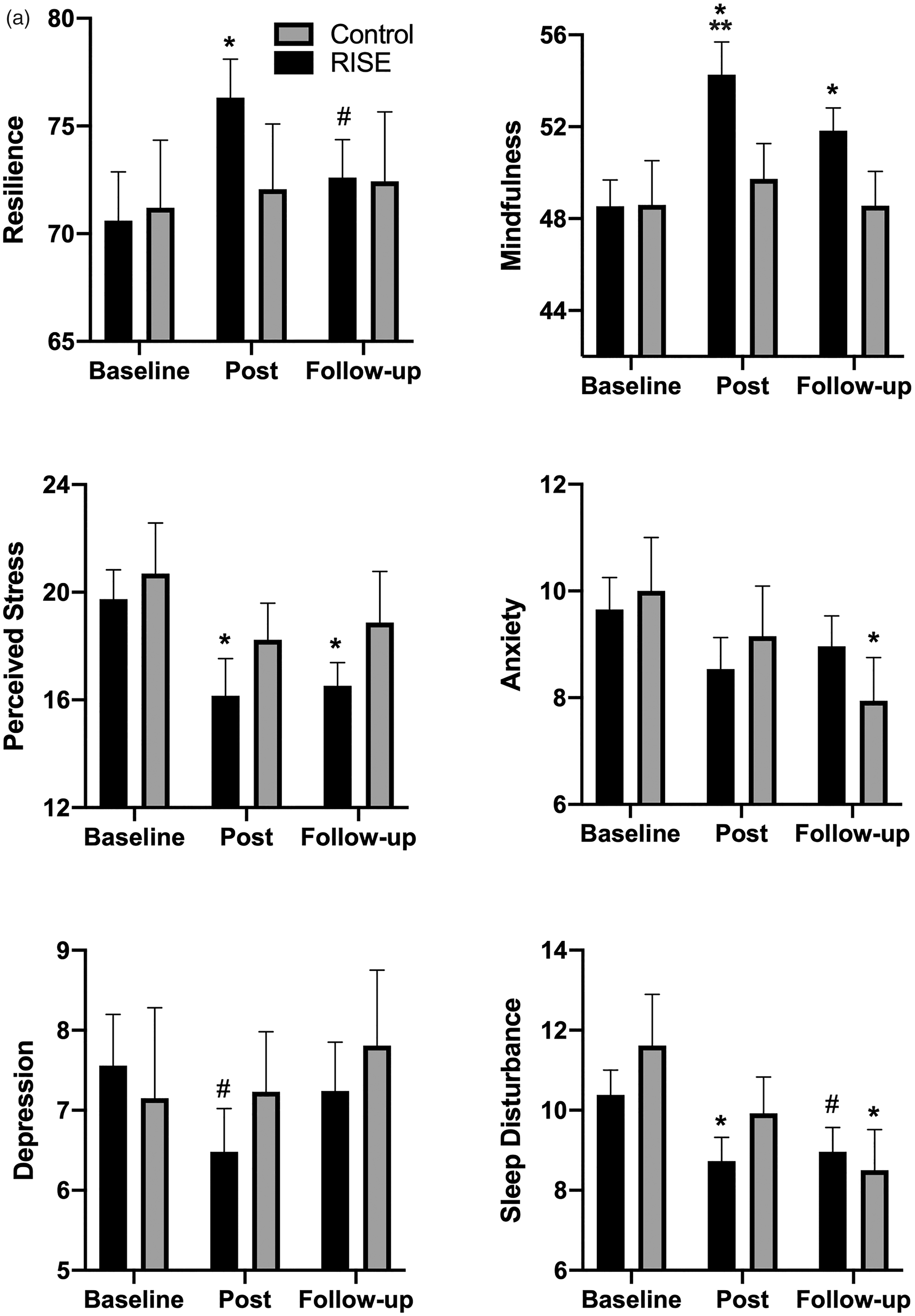
a and b, The means and standard errors of the psychological health measures for the RISE group and control group at baseline, post-program “Post”, and two-month follow-up “Follow-up” time points. *p < 0.05 compared to baseline (within groups analysis), #p < 0.08 compared to baseline, **p < 0.05 compared to control (between groups analysis).
From baseline to two-month follow-up, the RISE group reported significant improvements in mindfulness [t(23) = 3.03, p = .006, d = .62], stress [t(24) = −3.24, p = .003, d = .65], work exhaustion [t(24) = −3.78, p = .001, d = .75], interpersonal disengagement [t(24) = −2.07, p = .049, d = .37], total burnout [t(24) = −3.08, p = .005, d = .62], and physician well-being [t(24) = −2.38, p = .026, d = 0.48]. There were marginal improvements in resilience [t(25) = 1.86, p = .075, d = .36] and sleep disturbance [t(24) = −2.04, p = .053, d = .41]. The control group improved in anxiety [t(15) = 1.36, p = . 036, d = .58] and sleep disturbance [t(15) = 2.38, p = .031, d = .59] from baseline to two-month follow-up.
An exploratory between-group analysis revealed a statistically significant between-group difference in mindfulness [F(1, 40) = 9.58, p = .004, η2 = 0.20] from baseline to post-program, whereby the RISE group improved compared to the control group, but no improvement in work exhaustion [F(1, 40) = 4.01, p = .052, η2 = 0.09] from baseline to two-month follow-up compared to control (Figure 2(A) and (B)).
Discussion
To our knowledge, this is the first controlled study of a yoga-based MBI in residents and was unique in including residents from multiple academic medical centers and specialty departments. As delivered in this study, RISE was not rated as highly feasible by residents. Most importantly, residents reported that their work schedule conflicted with the delivery of the program. In an efficacy analysis, those receiving RISE reported improvements in multiple measures of psychological health from baseline to post-program, which were sustained at two-month follow-up.
MBIs have previously been evaluated in residents with mixed outcomes. Most studies evaluated mindfulness-based interventions; to our knowledge, there is only one single-arm pilot of a yoga-based MBI in residents. 42 MBSR administered to surgical interns was found to improve mindfulness, reduce stress, and improve well-being. 43 Several studies demonstrated reduced stress and/or burnout after meditation-based MBIs,44–48 whereas others did not observe an effect.49,50 In a feasibility study of a mindfulness intervention for German residents, the program was rated as highly feasible with no attrition, but included only nine participants and no comparison group. 44 While our study experienced high levels of nonattendance, this could be attributed to differences in work hours— U.S. residents are limited to a maximum of 80 hours per week while European residents are limited to 48 hours. 51 Several studies included interventions that were structured by residency program with protected didactic time, which improved feasibility.26,47,48 One program 26 used moonlighters to cover trainee time, which is costly and requires institutional commitment. In all, there is heterogeneity in the design and implementation of MBIs for residents.
The participants in our study reported that feasibility would improve if RISE was offered separately by residency program, potentially addressing work schedule conflicts. Participants also thought feasibility would improve if RISE was delivered virtually (e.g., videoconferencing or smartphone app). Virtual delivery of MBIs have been studied in a limited manner: a trial of smartphone-delivered vs. in-person mindfulness intervention in health care workers demonstrated increased well-being in both groups, but the in-person group had additional improvements in stress and burnout. 52 In our study, most participants utilized online RISE resources even if they did not attend in-person sessions, suggesting virtual delivery as a potential adaptation (Table 2). In a previous RISE study, livestream and recordings of in-person sessions increased participation. 24 On a practical note, brief interventions may improve feasibility for busy resident physicians.47,53 In the MBSR literature, the standard 26-hour form has the most empirical support, but there is no correlation between reduction in psychological distress and the number of in-class hours. 54 In all, a flexible format with a variety of delivery options may better suit resident physician needs.
A larger question inevitably arises: what is the utility of programs such as MBIs when systems-level issues contribute to burnout? While it is crucial organizational changes occur, individual interventions are also effective. 10 Given the time and resources required for organizational changes, MBIs may be a time-sensitive and cost-effective way to address clinician distress in the short term and complement large-scale changes. In addition, there is evidence that individual and workplace factors play similarly large roles in determining burnout and depressive symptoms, 55 arguing for a fine-tuned approach to problem assessment and solution development. MBIs have been successfully implemented at scale, demonstrated by the Mindful Medical Center. 56 Finally, medicine is an inherently stressful profession, so providing an MBI could be considered essential resiliency skills training, similar to other high-performing professions. 57
Limitations
Our study had multiple limitations. It was conducted in a self-selected, single geographic area, limiting generalizability. While between-group analysis is the most rigorous statistical approach, given the exploratory purpose of this feasibility study, we report both between- and within-groups analyses. We also had lower participation of residents in surgical subspecialties, suggesting the need for an individualized approach by specialty. Study participation and attendance may have been improved by making sessions mandatory, but there is some evidence that MBIs are more effective when individuals volunteer. 58 RISE is relatively brief compared to other MBIs, offering only 6 hours of in-person intervention compared to 16 hours reported by Lebares et al. 26 However, based on our results, we felt a shorter program was more feasible. By chance, the RISE group reported higher baseline mind-body practice compared to control, which may have diminished effect sizes of psychological outcome measures. There was likely heterogeneity introduced given implementation over two years, though this was minimized by administering the study during the fall each year. Finally, though we did not follow participants past the two-month timepoint, most other studies of MBIs in residents used a single-arm study design with minimal follow-up.24,44
Conclusions
This is the first controlled study of a yoga-based MBI in residents. As delivered in the present study, a yoga-based MBI, RISE, was not highly feasible for residents; however, given observed improvements in psychological outcomes, virtual delivery should be studied. In addition, given variability in resident MBIs and time constraints, a minimum effective dose for MBIs in this population should be determined. Finally, RISE may be more feasible if structured into the residency program. Innovation is urgently needed to support physician well-being (Table 3). Future studies will investigate virtual delivery and integration into residency program structures.
Resident well-being innovation: supports and barriers.

Supplemental Material
sj-pdf-1-gam-10.1177_21649561211001038 - Supplemental material for Evaluation of a Yoga-Based Mind-Body Intervention for Resident Physicians: A Randomized Clinical Trial
Supplemental material, sj-pdf-1-gam-10.1177_21649561211001038 for Evaluation of a Yoga-Based Mind-Body Intervention for Resident Physicians: A Randomized Clinical Trial by Julia Loewenthal MD, Natalie L Dyer PhD, Marla Lipsyc-Sharf MD, Sara Borden MBA, Darshan H Mehta MD, MPH, Jeffery A Dusek PhD, Sat Bir S Khalsa PhD in Global Advances in Health and Medicine
Supplemental Material
sj-pdf-2-gam-10.1177_21649561211001038 - Supplemental material for Evaluation of a Yoga-Based Mind-Body Intervention for Resident Physicians: A Randomized Clinical Trial
Supplemental material, sj-pdf-2-gam-10.1177_21649561211001038 for Evaluation of a Yoga-Based Mind-Body Intervention for Resident Physicians: A Randomized Clinical Trial by Julia Loewenthal MD, Natalie L Dyer PhD, Marla Lipsyc-Sharf MD, Sara Borden MBA, Darshan H Mehta MD, MPH, Jeffery A Dusek PhD, Sat Bir S Khalsa PhD in Global Advances in Health and Medicine
Supplemental Material
sj-pdf-3-gam-10.1177_21649561211001038 - Supplemental material for Evaluation of a Yoga-Based Mind-Body Intervention for Resident Physicians: A Randomized Clinical Trial
Supplemental material, sj-pdf-3-gam-10.1177_21649561211001038 for Evaluation of a Yoga-Based Mind-Body Intervention for Resident Physicians: A Randomized Clinical Trial by Julia Loewenthal MD, Natalie L Dyer PhD, Marla Lipsyc-Sharf MD, Sara Borden MBA, Darshan H Mehta MD, MPH, Jeffery A Dusek PhD, Sat Bir S Khalsa PhD in Global Advances in Health and Medicine
Footnotes
Acknowledgments
The authors would like to thank the Kripalu RISE staff, especially yoga instructor Jennifer Johnston and coordinator Jamyal Newton.
Author Contributions
JL, JAD, and SBSK were responsible for study conception and design. JL, MLS, SB, and NLD were responsible for data collection. NLD analyzed and interpreted data. JL drafted the article. SBSK, JAD, NLD, MLS, and DHM provided critical revision of the article. All coauthors gave final approval for submission of this version of the article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors JL, NLD, MLS, SB, DHM, JAD, and SBSK report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Osher Pilot Research Award (SBSK) from the Osher Center for Integrative Medicine, Brigham and Women’s Hospital, Harvard Medical School; Partners Centers of Expertise in Medical Education grant, Partners HealthCare Graduate Medical Education (JL).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.