
Abstract
Objective
Assess therapeutic value of specific yoga poses for thoracic and lumbar adolescent idiopathic scoliosis (AIS) taught in office or Internet.
Study Design
Nonrandomized control trial: Fifty-six adolescents (mean age 14.0 years; mean Risser 3.0) were recruited from our clinic; 41 did the side-plank, the half-moon and elevated side plank poses as appropriate (treatment group) and 15 did not (controls). Thirty curves were treated in office, 30 via Internet. Curve change was evaluated by blinded serial Cobb angles, and analyzed using Mann-Whitney U, paired t-tests and χ2.
Results
Mean lumbar and thoracolumbar Cobb angle change was −9.2 (95% CI = −11.8, −6.6) in the treatment group and 5.4 (95% CI = 1.7, 9.0) in controls. Both treatment group improvement and deterioration in controls were significant (treatment group: paired t-test t = −7.1, df = 40, p = .000; controls: t = 3.2, df = 12, p = .008). Mean thoracic Cobb angle change was −7.1 (95% CI = −13.1, −1.2) in the treatment group and 9.3 (95% CI = 4.5, 14.6) in controls. Both changes were significant (paired t-test t = −3.3, df = 21, p = .022 for treatment group; t = 4.5, df = 5, p = .006 for controls). Nine Internet patients were non-compliant vs. 6 office patients. Office patients improved 1.6 degrees/month or 5.5%/month; Internet patients improved .72 degrees/month or 3.3%/month.
Conclusion
These yoga poses show promise for reversing adolescent idiopathic scoliosis. Telemedicine had greater non-compliance and lower efficacy but still produced patient improvement.
Introduction
Scoliosis is an abnormal three-dimensional spinal curvature currently estimated to affect 2% to 3% of Americans, or 6,000,000 – 9,000,000 individuals. 1 Since the virtual elimination of polio and tuberculosis, between 80% and 90% of scoliosis appears in adolescence, is without known cause, and is labeled Adolescent Idiopathic Scoliosis (AIS). 1 Degenerative Scoliosis (DS), appearing in adulthood, and older people who have retained their AIS largely account for the remaining cases of scoliosis. Severity of scoliosis is classically assessed by Cobb angles: The diagnosis is made with a Cobb angle of 10 degrees or more. Bracing is recommended for curves between 25−45 degrees, and surgery is considered for angles at or above 45 degrees. 2 In the absence of treatment, curvature is estimated to increase at a rate of 1% per year, although growth and vulnerability greatly accelerate curve increase in some adolescents,3,4 and authors disagree about the natural history.3,4
The International Society on Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT), a prominent group of scoliosis physicians, patients, their parents and therapists has recently delineated avoidance of surgery as the chief goal of conservative therapy. 2
Bracing is currently the favored modality, with positive studies reinforcing this belief. However, the Cochrane Data Base finds only “low” or “very low-quality evidence” supporting this strategy. 5 Physiotherapy frequently accompanies brace use, as does the Schroth Method, which attempts to restore normal spinal position with a rotational breathing technique, 6 the Clear Method, which uses stabilization, de-rotation, and ‘active self-correction’ and a number of other chiropractic methodologies. Here, again, no choice can be evidence-based, since weak and conflicting studies are all that exist at this point.7–13
The young human spine can be considered a tensegrity structure, 14 held erect by tension generated by the muscles that attach to it directly, or to the ribs. Other examples are tent poles and radio antennae, which are held aloft, paradoxically, by cables pulling symmetrically downward. In the human body, muscles pulling downward symmetrically, right and left, dorsally and ventrally, are what keep us erect. Looked at this way, scoliosis results from asymmetrical force applied to one or more parts of the spine, bending it toward the side exerting greater force. Strengthening the weaker (convex) side then might plausibly reduce the curvature. Since we are dealing here with postural muscles, strength and endurance are the chief attributes we seek. Our hypothesis was that isometric yoga and yoga-like positions, notably, side-planks and altered half- moon pose would logically do this (see Figure 1). Our main objective was to compare before-and-after Cobb measurements. Secondarily we compared outcomes after office visits with telemedicine.
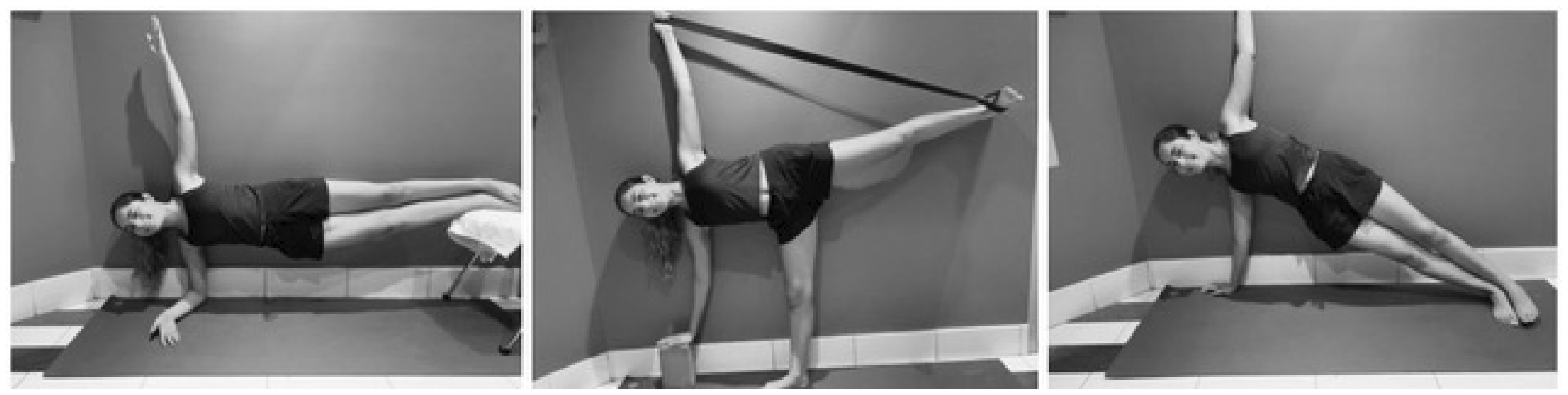
Yoga poses: Right: Side plank, used for lumbar and thoracolumbar curves. Center: Half-moon, with block and belt, used for thoracic and thoracolumbar curves. Left: Floating side plank, used with thoracic and thoracolumbar curves.
Materials and Methods
From November 22, 2017 to February 25, 2020 our Manhattan clinic saw 177 patients with AIS.
We studied Cobb angles of serial X-rays read by blinded radiologists, against the backdrop of the predicted natural history and comparison with those patients who did not do the yoga-like poses. Patients were seen in the office or by Internet depending on their convenience.
Inclusion criteria:
under 21 years of age, scoliotic curve equal to or greater than 10 degrees, parental consent for those under 18 years of age, stated willingness to do the yoga and yoga-like poses daily, and Cobb films read by independent radiologists.
Exclusionary criteria:
neurological, muscular or neuromuscular disease, (e.gs. cerebral palsy, myopathy, Guillain-Barre), genetic abnormalities that affect limb growth, proportionality or metabolism, (e.g., Marfans syndrome). pregnancy and other conditions prohibiting X-rays or minute(s)-long exertion (e.g., congestive heart failure, great weakness).
All patients qualifying for the study were taught the appropriate poses by a certified yoga therapist or experienced teacher in the clinic as follows: For the lumbar curve, the side plank, with convex side down (Figure 1). In this position, the weaker convex side is held up off the mat by its quadratus lumborum and paraspinal muscles, and the ipsilateral iliopsoas. The idea is that if the patient holds this pose for as long as possible, these muscles will grow in strength and stamina, generating forces more comparable to their contralateral counterparts.
The half-moon pose and the elevated side plank were prescribed for thoracic curves, with thoracic convexity down, using block and belt (see Figure 1). In the half-moon pose pulling forcibly on the belt attached to the horizontal foot is intended to induce the lower convex side’s latissimus dorsi and intercostal muscles to stay powerfully contracted, thereby increasing their strength and increasing their pull on the convex side of thoracic scoliosis. In the elevated side plank the patient’s weight is supported by contraction of the latissimus dorsi, the rhomboids, pectoralis and serratus anterior as well as the ipsilateral thoracic and contralateral lumbar paraspinal muscles. These muscles are strengthened with their prolonged involvement. Patients with S- or inverted S-curves were taught all three poses, each with the appropriate convex side down. For a summary of the positions, see Table 1.
Summary of poses and their applications.

Patients were encouraged to try out the poses for a few days, and then hold them for as long as possible at least once each day for 5 months, and then to have a repeat x-ray. Each patient had initial and later coronal plane x-rays read by radiologists blinded to participation in the study. Complex curves (i.e. S or inverted S) were analyzed into lumbar and thoracic components and assessed with the simple lumbar and simple thoracic curves. Thoracolumbar curves were analyzed with the lumbar curves. When possible, baseline and follow-up x-rays were done at the same facility. Control patients were also taught the appropriate poses. They were simply the people that did not do the poses (see Figure 2). None of the patients were handicapped or prevented from doing the pose for any reason but personal preference. No effort was made to reduce any bias that might have influenced their decision-process or that it might introduce positive or negative motivation.

Flow chart of study design.
This was a nonrandomized control trial: Fifty-six adolescents (mean age 14.0 years; mean Risser 3.0) were recruited from our clinic; 41 did the side-plank, the half-moon and elevated side plank poses as appropriate (treatment group) and 15 did not (controls). Thirty curves were treated in office, 30 via Internet. Curve change was evaluated by blinded serial Cobb angles, and analyzed using Mann-Whitney U, paired t-tests and χ2.
Our previous work 15 reached significance at 26 patients, with standard deviation of post-yoga Cobb angles, and a 10-degree effect, indicating that 29 patients would be adequate for the current study. In the Mann-Whitney U, paired t-tests and χ2 for linear trend we grouped patients according to the accepted limits of 10–24.9 degrees (expectant observation), 25–44.9 degrees (bracing recommended), and 45 degrees or more (surgical candidacy) (see Table 2).
Number of Patients by Severity (Cobb Score Grouping), Baseline Versus Follow-up, Those Doing the Yoga Poses Versus Those not Doing the Yoga Poses, by Type of Curve.

1 Shaded cells denote no change in severity grouping Time 1 vs Time 2; those below the diagonal improved; those above the diagonal got worse.
The study was approved by the Chesapeake Institutional Review Board, now Advarra.
Results
177 AIS patients were seen, of whom 131 agreed to the conditions of the study and were admitted. They were all shown and asked to perform in our presence the poses appropriate to their diagnosis. Seventy-five were lost to follow-up either because they did not get subsequent X-rays or because they did not respond to repeated telephone calls and emails. Of the 131 patients, 56 patients (42.8%) submitted follow-up x-rays; at that time 41 (31.3%) self-reported doing the yoga poses for as long as they could hold them, at least 4 times weekly, and 15 (11.5%) reported that they did not do the poses at least that often. Table 3 presents descriptive statistics for the study sample: those 41 patients who did the yoga poses (treatment group) versus the 15 who did not (control group). Groups did not differ by age, Risser number, gender, curve type or interval between first and second x-ray. Baseline and follow-up x-rays were not uniformly timed and there was a broad range in the interval between them (from ∼3 months to 2.5 years). We multiply telephoned and emailed patients with incomplete data, and eventually excluded those whose data sets remained incomplete. At baseline, lumbar and thoracolumbar Cobb angles were comparable between groups (Mann-Whitney U statistic = 288.5, P = .656) but thoracic Cobb angles differed significantly with the treatment group having higher (i.e. more severe) scores (U = 82.0, P = .030). At follow-up, lumbar & thoracolumbar Cobb angles differed significantly with the treatment group having lower (i.e.; less severe) scores (U = 159.0, P = .030) while the thoracic Cobb angles had become comparable between groups (U = 60.0, P = .562). In the treatment group median baseline versus follow-up lumbar Cobb angles were 28.0 and 20.0 respectively and median baseline versus follow-up thoracic Cobb angles were 40.3 and 25.0. Mean change in lumbar & thoracolumbar Cobb angles was −9.2 (95% CI = −11.8, −6.6) in the treatment group and 5.4 (95% CI = 1.7, 9.0) in the control group. For both groups, paired t-tests indicated statistical significance: t = −7.1, df = 40, P = .000 for the treatment group and t = 3.2, df = 12, P = .008 in the control group. Mean change in thoracic Cobb angles was −7.1 (95% CI = −13.1, −1.2) in the treatment group and 9.3 (95% CI = 4.5, 14.6) in the control group. For both groups, paired t-tests indicated significance; t = −3.3, df = 21, P = .022 for the treatment group and t = 4.5, df = 5, P = .006 in the control group.
Descriptive Statistics for the Study Population.

1Independent samples t-test, d.f. = 54.
2χ2 with continuity correction, d.f. = 1 for gender; Pearson χ2, d.f. = 2 for diagnosis.
3Interquartile range.
Table 4 presents a cross-classification of x-ray pairs, baseline versus follow-up, by level of scoliotic severity. In the treatment group 20 (49%) of lumbar and thoracolumbar x-ray pairs showed clinically significant improvement at follow-up and 21 (51%) held steady; in the control group no one had improved, 10 (77%) held steady and 3 (23%) showed deterioration. Among thoracic x-ray pairs, 5 (29%) in the treatment group showed clinically significant improvement at follow-up, 11 (65%) held steady and 1 (6%) showed deterioration; in the control group none showed improvement, 2 (33%) held steady and 6 (67%) showed deterioration. Table 4 summarizes the flow through the pre- versus post-severity grid by group and x-ray site. At both sites, the two groups differ in a way that indicates improvement in the treatment group and deterioration in the control group (χ2 for linear trend = 13.8, P = .000 for the treatment group and 7.9, P = .005 for the control group, both with df = 1). Among those who did the yoga poses there were no significant differences in age, gender, Risser number, baseline Cobb angle or baseline to follow-up interval between those who did and did not improve; this was true for both lumbar and thoracolumbar x-rays and for thoracic x-rays.
Worsening, Stability or Improvement of Lumbar and Thoracolumbar and Lumbar Curves at Follow-up for Those Who Did Yoga Poses and Those Who Did Not Do Yoga Poses.
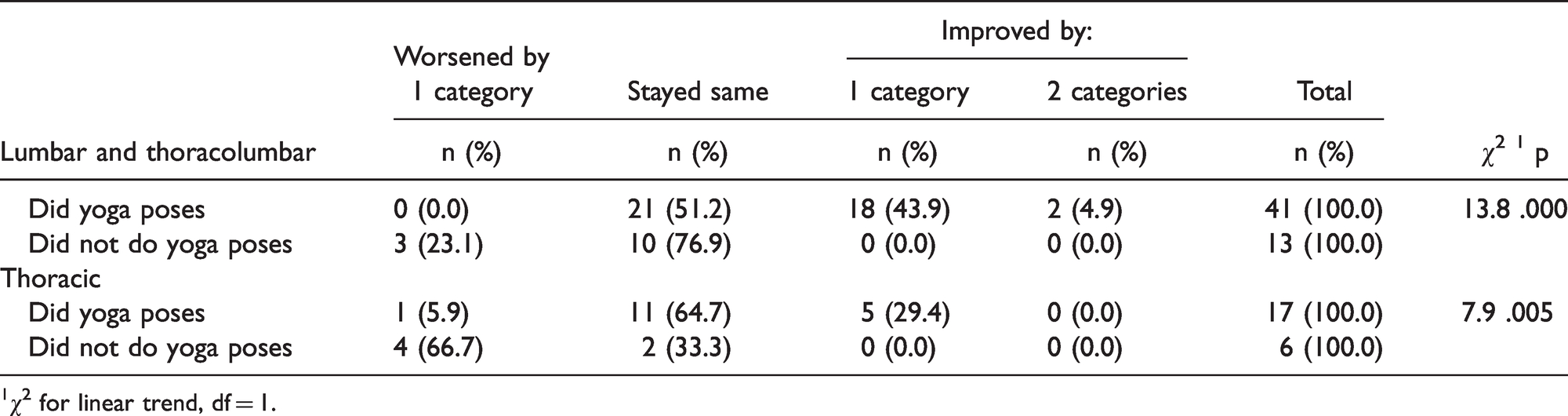
1χ2 for linear trend, df = 1.
Because prolonged attempts to reach patients often increased the times between X-rays in ways that had no direct bearing on their results, we isolated the 20 patients and the 6 controls with less than 1 year between their initial and subsequent X-rays: Compliant group’s mean age at first X-ray was 12.9 years (s.d. 2.2), with mean initial curve angle of 35.41 (s.d. 20.1). Mean gain for the compliant patients over that period was 8.65 degrees (s.d. 8.32) in mean 5.6 months (s.d. 2.2) = 1.6 degrees per month or 4.4% per month. Those who did not do the pose(s) had mean age at initial X-ray of 14.9 (s.d. 2.8), with initial curve of 35.2 (s.d. 11.9).and a mean 9.7 months (s.d. = 2.8) between X-rays. They lost 2.73 degrees (s.d. 2.86) over that period or 0.28 degrees/month or 0.07%/month.
Thirty curves belonged to patients seen in the office, and thirty were evaluated and treated over the Internet, on Skype, Zoom and Facetime. Six patients were non-compliant in the office-visit group; 11 were non-compliant in the telemedical group. Compliant office-seen patients began with a mean curve of 36.5 degrees and had mean gain of 10.9 degrees in a mean 7.7 months, gaining 1.6 degrees/month or 5.5% per month. Telemedicine patients began with a mean 33.5-degree curve, which was reduced by 8.5 degrees over 11.8 months, for a mean 0.72 degree gain/month and 3.3%/month reduction in curve.
Non-compliance was significantly higher in the telemedical group (11 of 30 vs. 6 of 30) and improvement per month was somewhat lower in the telemedicine group. Still Internet yoga definitely had a positive effect.
Discussion
These observational data strongly suggest that simple yoga and yoga-like poses applied to thoracic and lumbar AIS curves can be effective in reducing curve magnitude. Group differences were significant at both x-ray sites and improvements were in evidence across the range of severity. The intervention presents no strong obstacles to compliance and is extremely cost-effective. A recent study 16 to “replicate” our previous work with the side plank for lumbar scoliosis came to negative conclusions. However, close scrutiny of the composition of the intervention group in that study revealed that it did not have even one patient with lumbar scoliosis, the condition for which the side plank was shown helpful in our previous paper 15 and in this paper. The vicissitudes of randomization had unfortunately produced a study group containing no patients relevant to evaluating this method.
An innocuous, effective and almost costless treatment for AIS has three advantages. To see them we must first consider a young girl or boy entering the teen years: 1) their bodies are changing, 2) their intimate impulses are gathering, and 3) their peer-group affiliations are changing from their parents to their friends. Bracing and surgery may: 1) alter one’s relationship to one’s own body, 17 2) interfere with dancing, sports and any closer contact, and 3) frequently leave young patients alienated or even ostracized from their social group. 17 The recommended yoga poses take less than 5 minutes a day and do not impact any of these areas of concern.
Secondly, a simple patient-initiated way to treat scoliosis reduces the strain and uncertainty for all parties, from physician to family to young patient, who are otherwise all helplessly watching serial x-rays hoping the curves do not progress. In the current method patients are obliged to do the poses every day; as their curves decrease, their pride and sense of competence increases.
Third, an innocuous and practically free treatment can be initiated on young people with curves of 6 or 8 degrees. Although most children with curves under 10 degrees do not progress to bracing or operable levels, there is no doubt that all the curves of more than 10 degrees once were 6 and 8 degrees. This ounce of prevention may be indicated in young people with family histories, given the harmless and time-sparing nature of this virtually free method.
Weaknesses of the Study
This was not a randomized controlled trial. As such, the study sample was characterized by much variation vis-a-vis curve type, magnitude of baseline Cobb angle, interval between baseline and follow-up x-rays and, no doubt, fidelity of compliance, which was assessed by a single item self-report. Indeed, treatment and control groups were defined retroactively based on self-report of compliance at follow-up. There was no attempt to further quantify frequency or duration of yoga poses, but anecdotal evidence suggests that it generally rose from 30 seconds at first to 1.5 minutes. Still, people’s inclination to tell interviewers what they want to hear may make compliance appear greater than it actually was.
Conclusion
Sustaining the side plank, half-moon and elevated side plank positions for AIS shows promise for preventing further deterioration and reversing the condition. Secondarily, yoga appears to be successfully transmitted via the Internet, albeit less successfully than in person. A larger study with randomized control group is clearly preferable, with enough patients to also re-assess the efficacy of Internet treatment. The longevity of the improvements seen here must also be determined.
Supplemental Material
sj-pdf-1-gam-10.1177_2164956120988259 - Supplemental material for Isometric Yoga-Like Maneuvers Improve Adolescent Idiopathic Scoliosis—A Nonrandomized Control Trial
Supplemental material, sj-pdf-1-gam-10.1177_2164956120988259 for Isometric Yoga-Like Maneuvers Improve Adolescent Idiopathic Scoliosis—A Nonrandomized Control Trial by Loren M Fishman MD, BPhil (Oxon) in Global Advances in Health and Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.