
Abstract
Background/Objectives
This study was designed to test the impact of Tai Chi (TC) on healthcare utilization and cost in older adults living in low-income senior housing. We hypothesized that TC would improve overall health enough to reduce the use of emergency department (ED) and inpatient services.
Design
Cluster randomized controlled trial with randomization at the housing site level.
Setting
Greater Boston, Massachusetts.
Participants
The study includes 6 sites with 75 individuals in the TC treatment condition and 6 sites with 67 individuals in the health education control condition.
Intervention
Members of the treatment group received up to a year-long intervention with twice weekly, in-person TC exercise sessions along with video-directed exercises that could be done independently at home. The comparison group received monthly, in-person healthy aging education classes (HE). Study recruitment took place between August, 2015 and October, 2017. Key outcomes included acute care utilization (inpatient stays, observation stays and emergency department visits). In addition, the cost of utilization was estimated using the age, sex and race adjusted allowed amount from Medicare claims for a geographically similar population aged ≥ 65.
Results
The results suggested a possible reduction in the rate of ED visits in the TC group vs. controls (rate ratio = 0.476, p-value = 0.06), but no findings achieved statistical significance. Adjusted estimates of imputed costs of ED and hospital care were similar between TC and HE, averaging approximately $3,000 in each group.
Conclusion
ED utilization tended to be lower over 6 to 12 months of TC exercises compared to HE in older adults living in low-income housing, although estimated costs of care were similar.
Introduction
Currently, approximately 15% of older adults or 3.5 million people in the US live at or below the poverty level, 1 and many live in federal or state subsidized supportive housing facilities. Older adults living in public housing are twice as likely—57.3% vs. 26.9%—to report fair or poor health compared to those with no public housing experience. 2 They also tend to use more health care services, and account for a disproportionate share of Medicare spending, particularly for inpatient hospitalizations. 3
Given the large and growing challenge of supporting the health and health care needs of frail older adults living in subsidized housing, it is particularly important to identify interventions that can combat frailty, improve residents’ functional abilities, and ultimately reduce their health care costs. Tai Chi is an increasingly popular multimodal mind–body exercise that incorporates physical, cognitive, meditative, and social components in the same activity and offers a promising intervention for ameliorating many of the conditions that lead to poor health and excessive health care utilization. Studies have shown that Tai Chi exercise can improve a number of medical conditions relevant to frail older adults, including chronic heart failure,4–6 hypertension7,8 hyperlipidemia,9–11 coronary artery disease,12,13 chronic obstructive pulmonary disease,14–16 anxiety, 17 cardiorespiratory fitness,18,19 poor balance,20–23 reduced musculoskeletal strength and flexibility,19,22,24 Parkinson's disease, 25 cognitive decline,26,27 and overall mood.28,29 Preliminary studies also support the cost-effectiveness of Tai Chi programs delivered to older adults for fall prevention.25,30,31 However, few studies to date have specifically evaluated the benefits of Tai Chi on health and health care utilization in frail older adults living in subsidized housing.
The Mind Body-Wellness in Supportive Housing (Mi-WiSH) study is a cluster randomized, double-blind, attention-controlled trial designed to address this evidence gap. In a prior publication we reported on the impact of a year-long Tai Chi program on functional outcomes. 32 In this companion paper, we report the impact of Tai Chi on health care utilization and imputed health care costs (a co-primary aim).
Methods
Drawing on the Mi-WiSH trial and self-reported event data, this study assessed the impact of Tai Chi on healthcare utilization and cost for older adults living in low-income housing. As part of this work, we imputed cost for inpatient, emergency room and outpatient care using Medicare claims data from an age- and geographically-similar population.
Clinical Trial
Mi-WiSH was designed to test the impact of Tai Chi on health and health care utilization through a year-long intervention that involved twice weekly Tai Chi (TC) exercise sessions and video-directed exercises that participants could do independently at home. 32 The comparison group participated in a monthly healthy aging education (HE) program and randomization took place at the housing site level. Study recruitment occurred between August 3, 2015 and October 20, 2017. The study was halted prematurely after an interim analysis because the Data Safety Monitoring Board and National Institute on Aging sponsor determined the trial was unlikely to demonstrate treatment benefit for its primary outcome. Thus, only 8 out of 16 targeted sites were able to complete a full 12 months of participation in the randomly assigned treatment (i.e., TC or HE). For this analysis, we include data from 12 sites that had 6–12 months of the intervention.
Data
All participants received monthly phone calls to gather a range of data including falls and the use of medical services. In addition, research assistants recorded all self-reported emergency department visits, observation stays, and hospital use during Tai Chi or education group sessions. Since those in the Tai Chi arm had more intervention sessions, they had more opportunity to report service use. As a result, 92.6% of events came from monthly phone calls for the comparison group, compared to 73.2% for the treatment group. The remainder came from class logs or other communications with study staff.
Medicare claims data from beneficiaries living the greater Boston Hospital Referral Region (HRR), as defined by the Dartmouth Atlas, were used for price imputation. These data included inpatient facility (Part A) and physician bills (Part B) and enrollment information for 2015. The greater Boston HRR was used to limit the impact of variation in prices, although there is still some variation in the hospital wage index within this market. This more focused geography helps ensure that all beneficiaries experienced a similar healthcare and regulatory environment as the subjects of our study.
Sample
The clinical trial enrolled 180 participants from 14 randomized sites. However, analysis for health care utilization was restricted to the 12 sites at which the intervention was initiated and excludes 6 participants who completed baseline assessments but withdrew prior to initiation at their respective sites. The analysis sample therefore consisted of 75 individuals at sites offering Tai Chi and 67 individuals at sites offering the HE control condition. On average, Tai Chi participants completed 8.6 months of follow-up and HE participants completed 8.7 months of follow-up.
The Medicare cost imputation sample was limited to adults aged 65 years old or older with continuous Part A and B coverage for 2015 (N = 650,000). Those eligible for Medicare by virtue of having end-stage renal disease were excluded because they would most likely not meet the eligibility requirements for the MiWiSH trial. However, those who were eligible by virtue of a disability or dual enrollment in Medicaid and Medicare were included. This core sample was used in the regression analyses described below.
Utilization
Emergency department, observation, and hospital utilization events for study participants were collected during in-person sessions and telephone calls for members of both the treatment and comparison groups. Study staff asked about health care events since the last interaction and this information was recorded in a database with dates of service, a description of the type and reason for care, and a study participant ID. Members of the study team assigned a diagnosis code or DRG to each medical event based on the diagnostic information in the database.
Imputing Cost
For this study we used a gross costing method 33 that leverages Medicare claims data for the Boston HRR to determine the cost of care (to Medicare) for discrete inpatient and ambulatory events. With this approach, units of service are multiplied by an estimated unit cost, often from an external source. In our case we used hospital DRG payments for hospitalization greater than 3 nights and the institutional and provider costs for emergency department visits or observation stays.
To estimate costs, we considered removing indirect medical education (IME) and disproportionate share (DSH) hospital payments because we did not know how the use of academic or community-based institutions was distributed across study participants. However, there are many academic medical centers in Boston, so we decided to leave both IME and DSH payments as part of the average price per event.
Since participants reported inpatient, observation and emergency department visits, we estimated unit cost for these three types of services. For an inpatient stay, we first combined the institutional costs for the DRG and all Part B physician bills from the same window of time to come up with a total cost estimate for the stay.
For an observation stay, where the patient may only be in the hospital for one or two nights, we used the University of Wisconsin’s revenue center code method. 34 In this approach, both outpatient and inpatient revenue centers were used to identify events with revenue center code 0762. This allowed us to identify an observation stay and capture the institutional portion of this reimbursement. We then used the dates of service for the institutional bills to find all corresponding provider bills for the same time window. These were combined to create a total cost for each event.
Finally, for ED visits, we started with the provider bills to identify events with ED evaluation and management charges. This is a typical way to find ambulatory ED events. For ED events that converted to an inpatient stay, we identified care using revenue center code 0450-0459 or 0981. We then checked for outpatient facility charges for the same time window. In costing all three event types, the unit cost is the combined total for both the institutional and provider portion of reimbursements.
To estimate the average cost per DRG or diagnosis code, we developed an ordinary least squares (OLS) model that regressed unit cost on age, sex, race (non-white), original reason for Medicare eligibility (aged or disability), dual eligibility for Medicaid and Medicare, and diagnosis. The model was estimated separately for each type of service. Study participant parameters (e.g., age, sex, diagnosis) were then fed into the model to estimate an event cost.
Functional Measures
The primary physical function measure was the Short Physical Performance Battery (SPPB). 35 The SPPB includes measures of standing balance (timing of tandem, semi-tandem, and side-by-side stands, test-re-test (T-R-T) correlation = 0.97), 4-meter walking speed (T-R-T correlation = 0.89), and ability and time to rise from a chair 5 times (T-R-T correlation = 0.73). 36 The validity of this scale has been demonstrated by showing a gradient of risk for admission to a nursing home and mortality along the full range of the scale from 0–12. 35 In the EPESE population of community-dwelling elders over age 71, the SPPB captured a wide range of functional abilities, and summary scores less than 9 independently predicted disabilities in activities of daily living (ADL) and mobility at 1–6 years of follow-up.36,37
Depressive symptoms were assessed with the Center of Epidemiology Studies-Depression Scale Revised (CESD-R). 38 This validated measure has been used extensively in epidemiology studies and consists of 20 questions regarding feelings of depression, worthlessness, loneliness, energy level, and fear. The CESD-R has high internal consistency (r = 0.90) and a test-retest reliability of 0.51. 39
Falls were determined by questionnaire as any event in which the participant unintentionally came to rest on the ground or other lower level, not as a result of a major intrinsic event or an overwhelmingly external hazard. Study personnel questioned participants about falls in the past year, and also conducted monthly interviews in-person or by phone to determine the incidence and characteristics of falls during the study. All participants in both study groups were asked at each class about adverse events, health care utilization, and falls. When a fall or other event was reported, the participant was contacted within 24 hours to obtain details of the event.
Analysis
We performed unadjusted and adjusted analyses comparing health care utilization and cost of care for participants in the Tai Chi versus HE groups. Unadjusted analyses of utilization were compared by the Cochran-Armitage trend test. Adjusted analyses used mixed model Poisson regression with fixed terms for age, baseline SPPB score, baseline CES-D, and falls in the previous year and random intercepts and treatment effects by site pair. Unadjusted analyses of cost of care were compared by two-sample t-tests. Adjusted analyses of cost, which combined inpatient and observations says, used linear mixed models with fixed terms for age, baseline SPPB score, baseline CES-D, and falls in the previous year and random intercepts and treatment effects by site pair. This analysis produced a rate ratio (incidence rate for treatment/incidence rate for control) that allowed us to see how much more or less common the rate of utilization was in the treatment versus control group. Analyses were performed using SAS (version 9.4, SAS Institute, Cary NC).
Results
Baseline characteristics of Tai Chi and HE participants were well balanced with the exception of more black and fewer white participants in the Tai Chi group (Table 1). Both groups had similar rates of falls in the year prior to participation and similar SPPB scores.
Demographics and Baseline Characteristics.
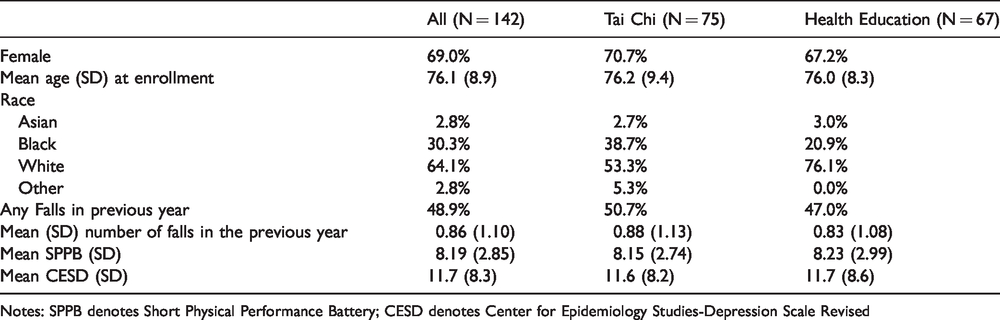
Notes: SPPB denotes Short Physical Performance Battery; CESD denotes Center for Epidemiology Studies-Depression Scale Revised
The overall proportion of participants reporting an ED visit was similar between Tai Chi and HE (27% vs. 33%; Table 2). The overall proportion of Tai Chi and HE participants reporting one or more inpatient stays (13% vs. 18%, respectively) was also similar. Reasons for admission included cardio- and cerebrovascular disease, respiratory illness, infections and joint replacement surgery (including fracture repair). The overall proportion of Tai Chi and HE participants reporting one or more fall that resulted in an ED visit or an inpatient stay (8% vs. 6%, respectively) was similar.
Unadjusted Comparison of Healthcare Utilization, Tai Chi and Health Education Groups (Number and Percent).

Notes: ED denotes emergency department.
Adjusted analyses that accounted for differing baseline characteristics (age, baseline SPPB, baseline CES-D, and falls in the year prior to enrolling) and differing time at risk showed trends toward lower rates of ED visits (rate ratio = 0.48, 95% CI 0.22 to 1.05, p = 0.06), inpatient/observation stays (rate ratio = 0.54, 95% CI 0.18 to 1.57, p = 0.19), and fall-related utilization (rate ratio = 0.57, 95% CI 0.11 to 2.85, p = 0.41) in the Tai Chi group, but none of these differences were statistically significant (Table 3).
Adjusted Comparison of Healthcare Utilization, Rate Ratio and 95% Confidence Interval.*
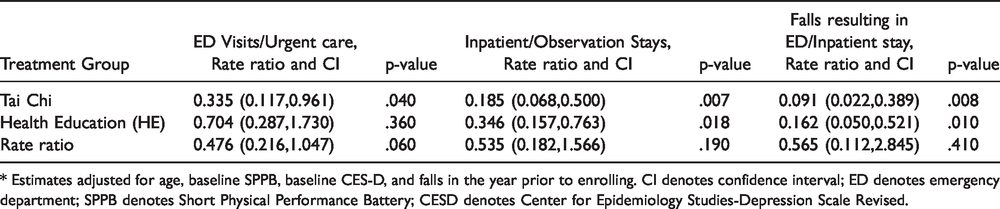
* Estimates adjusted for age, baseline SPPB, baseline CES-D, and falls in the year prior to enrolling. CI denotes confidence interval; ED denotes emergency department; SPPB denotes Short Physical Performance Battery; CESD denotes Center for Epidemiology Studies-Depression Scale Revised.
Both unadjusted and adjusted estimates of imputed costs of care were similar between Tai Chi and HE (Table 4). After adjusting for age, baseline functional status, depression, and falls in the year prior to enrolling, the estimated cost of adverse events was approximately $3,000 in each group. Note, this estimate does not include regular ambulatory care, which we assume is similar between the two groups.
Comparison of Total Imputed Costs, Unadjusted and Adjusted Results.*

* Estimates adjusted for age, baseline SPPB, baseline CES-D and falls in the year prior to enrolling. CI denotes confidence interval; SD denotes standard deviation; SPPB denotes Short Physical Performance Battery; CESD denotes Center for Epidemiology Studies-Depression Scale Revised.
Discussion
This study examined the healthcare utilization and costs of care for older adults residing in low-income housing who participated in a cluster randomized controlled trial of Tai Chi to improve strength, balance and mental health. We hypothesized that Tai Chi would improve overall health enough to reduce the use of emergency department (ED) and inpatient services. The results are suggestive of a possible effect, particularly in the area of ED visits, but no findings achieved statistical significance. The proportion of participants reporting an ED visit in our study (30%) was comparable to the 36% reported by the Center for Disease Control and Prevention for community-dwelling adults aged 65 and older. 40 Our results are consistent with the findings of our previously reported study of functional outcomes in the same cohort, which did not differ between those receiving Tai Chi or HE. 32
Li and Harmer found that Tai Chi was both effective for reducing fall risk, 41 as well as a cost-effective method for reducing fall related injury in older adults with high risk of falling. 42 Similar findings have been reported across a broad range of older adults.25,43–45 However, in our study, there was no observed difference in fall-related injuries among Tai Chi and HE groups. In fact, the rate of fall related injury was quite low, suggesting other proactive factors, such as safe housing (e.g., good lighting and hand rails), may have been in place.
One clear challenge was the small size of this study due to its early termination when the interim futility analysis revealed a null effect on functional outcomes. With only 75 older adults in the Tai Chi group and 67 in the HE group, it is possible that small effects were not detected. However, it is also important to consider the complexity of reducing emergency visits and inpatient stays for a multi-morbid population with other risk factors, such as low income. The impact of Tai Chi may be delayed, resulting in reduced inpatient stays during future periods rather than the first 6 to 12 months of participation. This study also took place in a healthcare market with a high concentration of value-based payment models. Area providers may have been working to reduce the use of ED and inpatient stays independent of this intervention.
For cost of care, we imputed prices using Medicare claims data for beneficiaries in the same market for a similar time period. This innovative strategy allowed us to add cost information to a cluster randomized controlled trial that did not have access to patient billing records. Since study participants included a mix of individuals in fee-for-service Medicare and Medicare Advantage (managed care) plans, we were able to apply consistent prices based on self-reported utilization, eliminating challenges associated with different billing systems, each with a different quality of utilization and reimbursement information. The primary challenge with this approach is the accuracy of patient self-reported utilization. Recall bias is a problem with all ages and is probably a greater issue for frail older adults. 46
Both groups had an average cost of about $3,000 in acute care utilization. This is quite low for Medicare in general, reflecting the fact that we only priced 3 types of services (ED visits, observation stays and inpatient stays). The cost would have been higher if we included prices for ambulatory care. Worth noting, there was one outlier case with a long rehabilitation stay in the treatment group. As a result, the cost variable was quite skewed, making it difficult to detect an effect with small numbers.
Many clinical trials evaluating the effects of Tai Chi training on balance, mobility, physical function, and fall prevention in older adults have demonstrated clinically meaningful and sometimes quite large benefits.22–25 However, a small number of well-designed and adequately powered studies indicate no apparent benefit of Tai Chi.26–29 In our published summary of our main clinical findings, 32 we enumerated possible explanations for the limited response of Tai Chi observed in this, compared to other studies, and emphasize that causal interpretation and comparisons with other positive findings is confounded by differences in study design, eligibility criteria, interventions (i.e., Tai Chi style and specific forms), control groups, duration and intensity of exposure, quality and fidelity of instruction, and intervention adherence rates.30–32
Nevertheless, it may be difficult for an intervention like Tai Chi to disrupt chronic conditions that are characterized by steady deterioration, and for some populations, greater benefits may be seen if it is combined with other interventions known to improve resiliency through social interactions, stress reduction, better sleep, or physical fitness.
Limitations
As noted above, our results could be affected by recall bias. Also, the Tai Chi group had more frequent contact with the study team. This created more opportunities for these study participants to report utilization events. This may have led to some under-reporting in the HE group. Also, the costing method takes an average from many patients with a similar chronic condition profile. This average cost pricing method is limited to factors that are observable in claims data, making the result an approximation. However, there is no reason to expect the cost estimation to be different between the Tai Chi and HE groups. Future work in this area should consider methods for building more sensitive pricing models or pricing the entire episode of care, not just the acute event.
Conclusion
Although these results do not show statistically significant differences between the two groups, utilization was numerically lower for the Tai Chi group by a large fraction. Future research in this area may require larger samples to detect any benefit from Tai Chi and might consider specific disease processes that are particularly amenable to the therapeutic benefits of Tai Chi.
Impact Statement
We certify that this work is novel, adding to the literature on Tai Chi by looking at its impact on utilization and cost.
Footnotes
Acknowledgments
The authors are grateful for the loyal participation of our older study volunteers and the staff of the facilities in which they lived. Dr. Lipsitz holds the Irving and Edyth S. Usen and Family Chair in Geriatric Medicine at Hebrew SeniorLife.
Author Contributions
Dr. Lipsitz (Hebrew Senior Life) and Dr. Wayne (Brigham and Women’s Hospital) and their colleagues designed and implemented the original cluster randomized trial. Dr. Thomas consulted to the team on utilization and cost analysis throughout the project. Dr. Perloff contributed the method for using Medicare claims data to cost utilization in a cluster randomized trial. All authors contributed to the writing and review of this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter Wayne is the founder and sole owner of the Tree of Life Tai Chi Center. His interests were reviewed and managed by the Brigham and Women’s Hospital and Partner’s HealthCare in accordance with their conflict of interest policies. The other authors declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants R01AG025037, K24 AT009282 and the Boston Roybal Center P30 AG048785 from the National Institute on Aging, Bethesda, MD. The authors are indebted to the Executive Teams, housing site managers, and residents of Brookline, Somerville, Cambridge, and Boston Housing Authorities, Center Communities of Brookline, Rogerson Communities, and the Center for Survey Research group at the University of Massachusetts Boston.
Sponsor’s Role
The sponsor had no role in designing or implementing this study.