
Abstract
Background
Given the large number of obesity-focused studies conducted in schools, there is a surprising lack of data regarding teacher workplace health behaviors in the United States.
Objective
To determine the feasibility and effectiveness of an onsite fitness facility with a structured integrative wellness program to improve health-related outcomes among teachers and staff at an urban elementary/middle school.
Methods
A 2-year mixed-methods analysis using Patient-Reported Outcomes Measurement Information System (PROMIS) measures and qualitative interviews included 39 teachers and staff employed at an urban elementary/middle school in Baltimore, Maryland. The fitness facility was dedicated exclusively to teachers and staff and the integrative wellness program included group exercise classes, yoga, mindfulness, and nutrition competitions. T tests were used to compare quantitative outcomes at baseline, the end of year 1, and the end of year 2.
Results
Compared to baseline, at year 1, there was a significant improvement in the PROMIS Sleep Disturbance score. From baseline to end of year 2, there were significant increases in the PROMIS Global Physical Health as well as significant decreases in Sleep Disturbances, Fatigue, and Social Isolation. Qualitative interviews conducted at the end of year 1 indicated that teachers who used the facility felt that it improved their mood, increased their energy, motivated them to eat healthily, and gave them opportunities to socialize with their colleagues in new ways. This impact was further enhanced in year 2.
Conclusions
An onsite fitness facility with an integrative wellness program may improve health-related outcomes among urban elementary school teachers and staff, with the greatest benefits seen after 2 years of implementation.
Introduction
There are approximately 3.8 million full-time elementary and secondary school teachers engaged in classroom instruction in the United States. 1 Limited available data suggest that overweight and obesity prevalence among teachers exceed national estimates, 2 and there is a high prevalence of cardiovascular disease risk factors and metabolic syndrome among this population.2–4 Furthermore, teaching is often regarded as a stressful occupation, 5 and the widespread work stress associated with teaching has been identified worldwide. 6 The high level of stress could potentially worsen the effect of poor lifestyle choices, considering that work stress has been associated as a risk factor for weight gain, obesity, coronary heart disease and stroke, type 2 diabetes, and metabolic syndrome.7–10 Therefore, strategies to improve the health and well-being of teachers are warranted.
Although faculty and staff health promotion has been considered 1 of the 8 components of the Center for Disease Control and Prevention’s coordinated school health approach for decades, a 2007 analysis of the School Health Policies and Programs Study concluded that few schools in the United States offer coordinated health and physical activity promotion services to their faculty and staff.11,12 Beyond the presumed health and cost-saving benefits to school districts and employees themselves, a small but growing body of evidence suggests that efforts to improve teacher wellness can also positively affect student health and wellness goals.13,14 This possibility provides even greater incentive to design, implement, and evaluate effective school-based employee wellness programs to promote physical activity and overall health. The few coordinated school employee wellness interventions in the literature focus on educational and behavioral strategies to improve sleep, weight gain prevention, physical activity, and overall wellness coupled with the availability of existing school physical activity facilities for faculty use.15–17 Existing school physical activity facilities, such as student gymnasiums, are limited by unfavorable perception and lack of privacy for school employees. To our knowledge, school-based wellness programs that provide an on-site fitness facility with dedicated exercise equipment and access to an instructor for the exclusive use of school employees do not exist in the literature. Such an on-site facility was hypothesized to directly surmount many of the common barriers to physical activity reported among American adults. Commonly reported barriers to physical activity include a perceived lack of time for exercise, lack of access to a fitness facility, and limited knowledge or confidence in one’s ability to engage in physical activity.18–20 It also represents a modification of the school employee environment, which may be perceived as an opportunity for teachers and staff to initiate positive changes in health behaviors. 21 Therefore, the purpose of this mixed-methods outcomes evaluation was to assess the feasibility and effectiveness of a novel wellness program that provided a free on-site fitness facility and accompanying integrative wellness programming on physical, mental, and social health of teachers and school staff within an urban elementary/middle school.
Methods
This study included a quantitative and qualitative evaluation of teachers and staff employed at an urban public elementary/middle school who participated in a wellness program offered at their school. All teachers and staff employed at this school were eligible to participate in this study. This study was approved by the institutional review board of the University of Maryland School of Medicine. Participants received up to $140 in incentives for completion of all assessments which included quantitative surveys administered at 3 time points (baseline, follow-ups at the end of year 1, and at the end of year 2) and 2 semistructured interviews conducted at the follow-up time points at the end of year 1 and year 2.
Teacher and Staff Wellness Program
Through a public–private partnership, a 1574-square-foot wellness center equipped with treadmills, an Arc exercise machine, bikes, a rowing machine, and additional fitness facility equipment with locker room facilities was constructed onsite at an urban public elementary/middle school in Summer of 2015 prior to the start of this study. The wellness center was freely accessible to all teachers and school staff before, during and after the school day at no cost. A local wellness company was supported by the funders of the public–private partnership to provide integrative wellness services as an addition to the exercise facility. Wellness services included an onsite personal trainer available several days per week who provided group fitness classes and educational classes on integrative wellness topics such as the importance of nutrition, sleep, and stress management. Group yoga instruction was also offered as a part of the wellness program. The fitness programming was modified from year 1 using input from teachers utilizing the space. As a result of feedback following year 1, a larger variety of fitness classes were offered in year 2, in addition to more internal competitions and events.
Teachers and staff were provided with a wearable fitness tracker, but these data were unavailable to the study evaluation team. Investigators involved in the evaluation of this study were not involved in the construction of the fitness facility, conceptualization of the teacher and staff wellness program, nor its implementation at the school.
Questionnaires to Assess Physical, Mental, and Social Health of Teachers
The quantitative questionnaire included validated measures from the Patient-Reported Outcomes Measurement Information System (PROMIS). 22 Items for each measure were scored on a 5-point Likert scale. To reduce participant burden in this evaluation, the short forms of each scale were used. The PROMIS Global Health (v1.1) consisted of 10 items to measure an individual’s physical (GPH) and mental health (GMH). The GPH score comprises 4 items on physical health, physical functioning, pain intensity, and fatigue and the GMH score includes 4 items on overall quality of life, mental health, satisfaction with social activities and relationships, and emotional problems. Two PROMIS global items (general health and social roles) are scored separately. 23 The PROMIS Sleep Disturbance scale (v1.0, 4a) consists of 4 items to assess self-reported perceptions of sleep quality, sleep depth, and restoration associated with sleep over the past 7 days. The PROMIS Social Isolation (v2.0, 4a) is a 4-item scale to assess perceptions of being excluded, detached or disconnected from others, and the 4-item PROMIS Satisfaction with Social Roles and Activities scale (v2.0, 4a) assessed satisfaction with carrying out typical social roles and activities. To assess one’s ability to maintain cognitive functioning pertaining to memory, processing, and mental clarity, the 4-item Applied Cognition-Abilities scale (v1.0, 4a) was used. Self-reported fatigue and tiredness over the previous 7 days was assessed using the 4-item Fatigue survey (v1.0, 4a). The Emotional Distress—Anxiety 4-item scale (v1.0, 4a) assessed fear, anxiety, and uneasiness over the previous 7 days. The Companionship 4-item scale (v2.0, 4a) assessed one’s perception of having friendly association, particularly with individuals who share one’s interest. For each PROMIS measure, mean scores were created from the responses and higher scores equate to more of the outcome being measured. For example, higher scores for responses to the Global Health scale indicate better health, whereas higher scores for responses to the Sleep Disturbance scale indicate greater sleep disturbances.
Qualitative Interviews
One-on-one semistructured interviews with teachers and staff were conducted at the end of years 1 and 2 of the wellness program. All qualitative interviews were conducted by trained interviewers in-person with participating teachers and staff. The interviews took approximately 20 minutes each, and open-ended interview guide questions were asked of each participant. Questions focused on overall use of the fitness facility and frequency of use (see Supplemental Table). For those who reported using the facility, questions focused on motivations for use, perceived benefits of use related to exercise, and aspects of well-being beyond exercise in the fitness facility. The interview questions also focused on changes in healthy lifestyle behaviors and other areas of their lives related to their participation in the wellness program. In addition to addressing nonquantifiable elements of the value of the fitness facility, the qualitative questions asked about food choices, energy levels, sleep, and parameters of emotional health and relationships with others to complement the PROMIS measures. For those who did not report using the facility, questions explored reasons for not using the facility and recommendations to improve the facility that would encourage usage. The interviews were audio-recorded, with permission, and subsequently transcribed in full and deidentified for confidentiality purposes.
In the first stage of data analysis, 2 researchers reviewed the transcripts using NVivo 12 Plus (QSR International, Pty Ltd. Version 12, 2018). One researcher coded the material initially, using agreed upon codes drawn from the interview guide questions, which amplified the PROMIS items and served as a guiding framework. In year 1, interviews were compared and contrasted for similarities and differences in the teachers’ experiences and summarized for a report. In year 2, the same analysis method was used, but with a focus on changes in the teacher responses from year 1 to year 2. Secondary coding and theme development were guided by the pragmatic approach recommended by Miles et al. 24
Statistical Analyses
The quantitative outcomes were compared at baseline, the end of year 1, and the end of year 2 of the wellness program using pooled or unpooled t tests when the data were normally distributed, and Wilcoxon signed-rank sum or Mann–Whitney test when the data were non-normally distributed. All quantitative data statistical analyses were conducted in SAS Version 9.4. Statistical significance was defined as P ≤ .05.
Results
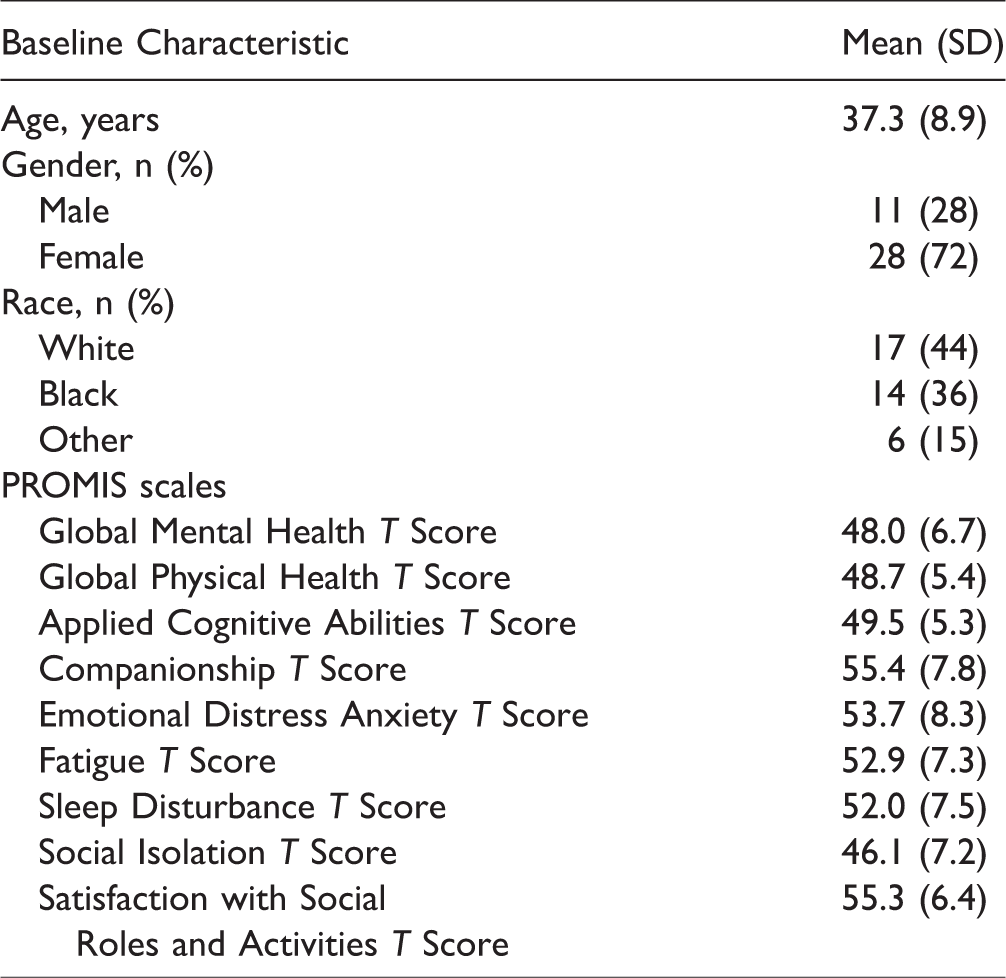
Moreover, 39 teachers and staff participated in at least 1 evaluation assessment, comprising ∼76% of all school employees. Of these participants, 33 completed the quantitative survey at baseline, 30 completed the survey at the end of year 1, and 29 completed the survey at the end of year 2. At follow-up time points, 1 teacher was unable to be reached, and 3 were no longer employed at the school. Demographics of teachers and mean baseline survey t scores are presented in Table 1. The sample was predominantly middle-aged females ranging in age from 24 to 60 years.
Baseline Characteristics and Mean PROMIS Measure Survey Scores of Teachers Participating in an Onsite School Wellness Program.
The changes in survey measures from baseline to years 1 and 2 are presented in Table 2. Compared to baseline, at year 1, there were statistically significant changes in the PROMIS Sleep Disturbance and Social Isolation scores. From baseline to end of year 2, there were statistically significant increases in GPH as well as decreases in Sleep Disturbances, Fatigue, and Social Isolation.
Changes in PROMIS Measures From Baseline to Follow-up Time Points Years 1 and 2 of Teachers Participating in an Onsite School Wellness Program.

Note: Bold text designates statistically significant changes from baseline.
Thirty-three teachers completed the semistructured interview at the end of year 1 and 38 completed the interview at the end of year 2. Twenty-eight teachers participated in semistructured interviews at both follow-up time points. In year 1, 61% of teachers reported using the fitness facility at least once a week. In year 2, the percentage of teachers using the fitness facility once a week or more throughout the year increased to 68%. The most common reported barrier to use of the fitness facility was limited time. Other barriers reported by teachers included a lack of child care, lack of motivation, self-consciousness, and inability to use the fitness facility due to disability. Key themes that emerged from the semistructured interviews are presented in Table 3. Teachers reported positive effects on sleep and overall mood as well as improvements in energy levels, reduced fatigue, and increased awareness of the food choices they were making. Teachers also reported that the fitness facility positively impacted the way that they socialized with their colleagues at work, and that students at the school displayed awareness and curiosity about the fitness facility.
Semistructured Interview Results.

Key themes related to use of wellness center and impact of wellness center utilization on physical and mental health.
Discussion
This study describes a novel approach to improving health-related outcomes among school teachers and staff by providing an onsite fitness facility with a tailored integrative wellness program to improve health behaviors among this diverse population. Using a mixed-methods approach, we were able to demonstrate that there are a variety of physical and mental health-related improvements associated with utilization of a wellness program exclusively for teachers and staff located on a school campus. These findings may be utilized to help improve health-related behaviors in teachers, a population at high risk for obesity, and comorbid conditions. Few studies have examined health-related behaviors among teachers, and to the authors’ knowledge, this is the first evaluation of a teacher wellness program where the exercise facility was constructed on school property for the exclusive use of teachers and staff.
The results from the PROMIS measures indicated more significant changes in health-related outcomes from baseline to year 2 as compared to changes from baseline to year 1. The qualitative interviews indicated that there was a greater sense of staff camaraderie surrounding the fitness center in year 2. Although motivation of coworkers was a common reason for use of the fitness facility in year 1, year 2 saw higher rates of participation in the group challenges, and more teachers reporting that the fitness facility brought staff together and improved their social life at work. Further reflecting this shift in staff culture around the fitness facility, the qualitative interviews revealed that self-consciousness as a barrier to use of the fitness facility was also reduced in year 2. Interestingly, reported participation in the fitness classes was stable between years 1 and 2, but individual independent use of the fitness facility increased. One possible explanation for this pattern is that teachers who only felt comfortable participating in group fitness classes in year 1 built up enough confidence to create their own workouts and use the fitness facility independently in year 2. Outside of the trainer-led fitness classes, multiple teachers reported gaining knowledge, assistance, and encouragement from their coworkers while using the fitness facility. At the end of year 2, interviewers observed that workout plans were written up in marker on the fitness facility mirrors so that teachers could have a workout to follow on their own if they could not make the classes. Interviews indicated a sense of pride and ownership of the fitness facility by the teachers as continued motivation for its use. More importantly, feedback from teachers after year 1 allowed for modifications to wellness programming that may have increased participation by tailoring the programming to the teachers’ requests. As such, engagement of teachers and staff in the evaluation process is critical for program sustainability. Furthermore, a review focused on the effectiveness of workplace health promotion programs by Goetzel et al. 25 reported that highly successful programs not only establish a culture of health within the organization but also include a long-term evaluation (3+ years) in order to fully assess changes in population health. Collectively, the quantitative and qualitative data for this study support this claim and suggest that it takes time for the optimal benefits of an on-site fitness facility and wellness program to manifest among school teachers and staff.
Results from our quantitative analyses and qualitative interviews indicated that teachers not only found relief from work-related stress by utilizing the fitness facility, but the onsite facility reduced some of the barriers to engaging in physical activity. The onsite facility was free to all teachers and available throughout the day which allowed teachers to utilize the fitness facility at their convenience. A recent analysis of a school district worksite wellness program found that wellness program participation among employees resulted in lower costs associated with medical claims, 26 although the evidence regarding effectiveness of approaches for obesity prevention was mixed. 16
In addition to adoption of new healthy behaviors and a greater sense of camaraderie among colleagues while at school, many teachers and staff reported that they had also carried their new health behaviors outside of school and into the lives of their families and friends. Furthermore, teachers reported that some of these healthy behaviors were passed on to students both in lesson plans and behavior modeling. Abi Nader et al. 27 reported that students accumulated more moderate to vigorous activity when teachers valued physical activity, suggesting that teachers with more positive views regarding health-related behaviors positively impact student behaviors and that the personal health knowledge of the staff may translate into positive environmental changes. This concept is consistent with data from the qualitative interviews which suggested that there were many positive effects that extended beyond the improvement in the health of teachers and staff. Traditionally, school-based interventions have focused on childhood obesity, 28 and few interventions have targeted health-related behaviors of the school staff, including teachers. Future studies should incorporate longitudinal measures of obesity-related health outcomes among both students and teachers to determine how or if these environmental changes translate to impact the health-related behaviors of the student as a result of improvement in teacher well-being and health.
We acknowledge several important limitations in this study. Although our qualitative interviews address use of the fitness facility and participation in the group fitness classes as well as perceived changes to dietary behaviors, we did not objectively measure anthropometrics, physical activity, or dietary intake. A notable strength of this study is the use of the PROMIS surveys that have been validated for use among adult populations to collect health-related outcome data. However, our sample population scored in the normal range on all the items measured at baseline, suggesting school staff in this study were representative of the mean health for the U.S. general population. Therefore, the observed changes may not be clinically relevant, and additional studies are needed to determine the impact on a less healthy population. Future studies should also incorporate other objective measures in addition to validated stress measures such as the perceived stress scale to complement the assessment of these outcomes. The sample size of the study was relatively small, although this was due primarily to the size of the school as participation in the outcomes evaluation was impressive with approximately 75% of the diverse population of school teachers and staff providing outcomes data. A final limitation is the limited generalizability due to the urban location and physical changes to the school environment which are not readily available to other school districts. The authors recognize that this fitness facility in this study was funded by public–private partnership, and this may not be feasible to build this type of facility in every public school. However, new schools are built every year, and a large number of schools are renovated in order to upgrade school facilities. It was estimated that the United States spent over $40 billion on school construction in 2011. 29 Incorporating physical fitness facilities into the school environment should be a priority when considering future construction projects. School nurses who participated in the planning and design process related to construction of health offices reported positive experiences. 30 Health professionals should utilize this opportunity to promote wellness in schools via direct modifications to the school environment and engaging school staff in the planning process to reduce barriers to increasing physical activity and promote healthy lifestyles among employees.
Conclusions
An on-site fitness facility and integrative wellness programming for teachers and staff was feasible, well-received, and offered immediate health benefits that increased over time. This may provide a model for wide-ranging health and wellness benefits derived from school-based environmental modifications and wellness programming. Future studies should focus on the design, implementation, and evaluation of effective school-based employee wellness programs to promote physical activity and overall health.
Supplemental Material
Supplemental material for An Onsite Fitness Facility and Integrative Wellness Program Positively Impacted Health-Related Outcomes Among Teachers and Staff at an Urban Elementary/Middle School
Supplemental Material for An Onsite Fitness Facility and Integrative Wellness Program Positively Impacted Health-Related Outcomes Among Teachers and Staff at an Urban Elementary/Middle School by Elizabeth A Parker PhD, RD Patrick F McArdle PhD Debbie Gioia PhD Ariel Trilling BA Mary Bahr-Robertson BA Nate Costa BS Brian M Berman MD Christopher R D’Adamo PhD in Global Advances in Health and Medicine
Footnotes
Acknowledgments
The authors thank the staff and administration of the University of Maryland School of Medicine Center for Integrative Medicine for their assistance with the study; and the administration and staff at the participating school for their assistance and collaboration throughout the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nate Costa is the President and CEO of FXwell, the company who provided integrative wellness programming at the school. The other authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work was supported by a grant from the JS Plank and DM DiCarlo Family Foundation, which had no role in study design, collection, analysis, or interpretation of data, writing the manuscript, or the decision to submit the manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.