
Abstract
Background
Research on incorporating integrative medicine (IM) into medical training is increasing. Programs and organizations around IM have been established, but there has not previously been a needs assessment focused on integrating IM into psychiatry training.
Objectives
The results of a needs assessment of training directors and faculty, focused on interest and priorities for developing an IM curriculum for psychiatry training programs, are described.
Methods
Psychiatry Training Directors and faculty were invited to participate in a detailed electronic survey. Areas of inquiry included (a) IM content areas to include in training; (b) IM approaches to specific medical conditions; (c) existing IM content; (d) importance, interest, and strategies for IM training; and (e) availability of wellness programs for trainees.
Results
Thirty-six respondents from psychiatry training programs completed the survey. Of the training programs represented by the respondents, 50% indicated that they currently had IM content in their curriculum; only 11.8% of them rated their programs’ existing IM content as sufficient. Content areas rated most highly for inclusion in a psychiatry IM curriculum included sleep health, motivational interviewing, and self-care. Respondents indicated incorporating IM into the psychiatry training curriculum (47%) or as an elective (44%) as the desired implementation strategy, with experiential onsite activities demonstrating IM topics (67%) and online modules supplemented by local faculty (58%) as the 2 most desirable learning formats. Significant barriers identified were time constraints, lack of faculty expertise in IM, current lack of curricular requirements for IM competencies, and budgetary limitations.
Conclusion
Responses to the survey suggest that faculty need support and additional education in implementing IM training. A standardized, online curriculum could help meet that need. Our results also indicate that wellness programs for residents are currently inadequate; bolstering them could help address burnout and increase the knowledge psychiatrists have of IM modalities. The types of institutions represented by faculty interested in further developing IM offerings vary considerably, as do their current efforts to integrate IM into training programs.
Introduction
In 2012, 33.2% of U.S. adults and 11.6% of children used complementary health approaches,1,2 amounting to an annual out-of-pocket expenditure of 30 billion dollars. 3 Complementary and alternative medicine (CAM) has been defined as “a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine”; 4 most approaches fall into 1 of 2 subgroups—natural products or mind–body medicine. Mind–body medicine techniques include breathing techniques, guided imagery, meditation and mindfulness, emotional awareness and expression, and biofeedback to enhance self-regulation. Most psychiatric patients already use CAM approaches to complement treatment provided by psychiatrists and other mental health professionals. 5 Depression, anxiety, and insomnia are the most frequently cited reasons patients begin using CAM, and 79% of those with major depressive disorder using CAM did not disclose their use of such treatment to their psychiatrist. 6 Lack of communication about modalities patients use without their physician’s knowledge can increase the risk of harm. These risks may include drug/herb-supplement interactions as well as harm resulting from the use of modalities that lack evidence of safety and are costly.
Integrative medicine (IM), as defined by the National Center for Complementary and Integrative Health, is a bringing together of conventional and complementary approaches in a coordinated way. A number of initiatives over the past 2 decades have sought to assess the incorporation of IM into medical training. Organizations such as the Academic Consortium for Integrative Medicine & Health have been established to promote research, education, and clinical programs in IM. The University of Arizona Center for Integrative Medicine (UACIM) has developed a comprehensive academic curriculum in IM.
Integrative Medicine in Residency (IMR), the 200-hour interactive online curriculum developed by UACIM, was piloted in 8 family medicine residencies between 2008 and 2011. 7 In addition, a 100-hour pediatric curriculum called Integrative Medicine in Residency-Pediatrics (IMR-P) is being piloted at 5 pediatric residency training programs. 8 IMR has demonstrated improvement in medical knowledge in IM as well as feasibility for implementation in residency training.7–9 To date, 77 residency training programs worldwide have used the IMR or IMR-P online curriculum, pairing these with various forms of onsite experiential learning.
No studies or programs have assessed how IM might be incorporated into psychiatric training. Research on IM in clinical practice is rapidly expanding as the field responds to rising demands from patients seeking more holistic and individualized options for their mental health care. 10 Furthermore, high rates of burnout among medical students and residents are spurring training programs to incorporate various aspects of self-care and other interventions rooted in the field of IM to promote physician wellness. 11 Modeled after the needs assessments used for developing the IMR curriculum, 12 this study assesses needs of psychiatry training programs to aid in designing an IM curriculum for psychiatric residents and fellows.
Methods
Data Collection and Analysis
Data were collected using an Internet-based survey website (Survey Monkey). Invitations were distributed via e-mail to all psychiatry residency and fellowship training program directors in the United States based on a list from the Accreditation Council for Graduate Medical Education (ACGME). The survey was open for a 3-month period from December 8, 2015, to March 8, 2016. Data were analyzed using IBM® SPSS® Statistics Desktop V22.0 (Armonk, NY). Descriptive statistics were generated for individual survey items. The study was submitted to the University of Arizona institutional review board for approval under the IMR-P curriculum evaluation project (project number 12-0492-00) and was deemed exempt (FWA 00004218). Informed consent was obtained as part of the electronic survey.
Survey Development and Content
The survey content was drawn from similar prior needs assessments conducted by UACIM when developing new online curriculum content. 12 Additional input on the survey design was obtained from faculty at the Center for Integrative Medicine and the Department of Psychiatry at the University of Arizona.
In the survey, IM was defined as a clinical practice that empowers individuals, social groups, and communities to achieve ways of living that promote health, resilience and wellbeing, and prevent disease. It advocates for person-centered healthcare that is informed by evidence and makes use of appropriate healthcare professionals, disciplines, healing traditions, and therapeutic approaches. IM includes both conventional and licensed complementary and alternative medicine (CAM) practitioners.13,a
IM content areas
Respondents were presented with a list of 16 potential IM content areas. Training program faculty were asked to rate the importance of exposing residents/fellows to the content areas. Items were rated on a 5-point Likert-type scale (1 = not important to 5 = very important). Respondents could provide additional content areas using a free-text field. Faculty were asked 2 additional questions to assess their readiness to teach IM and promote competence in their trainees. One probed their own level of confidence in answering resident/fellow questions concerning IM topics. The other explored faculty’s perception of their trainees’ confidence in answering patient questions about IM topics (1 = not at all confident to 5 = very confident).
Medical conditions
Respondents were asked to rate the importance of learning an IM approach for 18 specific medical conditions commonly encountered in or related to the practice of psychiatry (1 = not important to 5 = very important).
Existing IM content/expertise
Respondents were asked to indicate whether there was faculty with training or interest in IM at their training programs. Training program faculty were asked whether they had IM content in their existing training curricula. Those who responded yes (50%) were asked to detail the format(s) used for existing IM content in their curricula and whether they believed the content to be sufficient.
Importance, interest, and strategies for incorporating IM content into training programs
Faculty were asked several questions concerning interest in incorporating IM content (1 = not at all interested to 5 = very interested) and implementation strategies at their training programs. Implementation strategy questions included methods for incorporating IM content into training programs, ideal number of hours of content to provide, and learning formats. One question asked whether the respondent’s site would be interested in piloting an IM curriculum (yes/no). These programs were identified, and further analysis of those programs and IM implementation in them is included in the discussion section. Respondents also rated barriers to adding IM content into their programs on a 4-point scale (1 = not a barrier to 4 = major barrier). They could add other barriers and general comments on barriers. An open-ended question asked respondents to list the top 3 challenges of integrating IM content into their programs and suggestions for overcoming those challenges. Respondents were asked if they would need faculty education and training in IM in order to implement an IM curriculum (yes/no) for their trainees.
Wellness programs
Faculty were asked whether they had a program to promote self-care and wellness for psychiatric trainees (yes/no) and, if yes, what it included, based on a list of 9 wellness activities (yes/no). They were further asked to rate how well their existing program addressed resident/fellow burnout (1 = not at all to 5 = very well).
Results
Sample
A needs assessment was sent electronically to all psychiatry residency and fellowship training program directors in the United States, as identified by a list from the ACGME. There were 195 psychiatry faculty within psychiatry training programs on the list. Twenty of the e-mails were returned as undeliverable, which reduces the potential number of recipients to 175. Some of the e-mails on the list were generic in nature, along the lines of “psychres” or “psychiatryresidency.” Such e-mail addresses may be monitored by administrative staff rather than directly by program directors, and it is possible that the survey was not passed along to the intended recipient. Overall, 52 completed the consent and 36 completed the survey. The majority of survey respondents were faculty or program directors. Most sites were General Psychiatry residencies and many offered a Child & Adolescent Fellowship. Descriptive details of survey respondents are summarized in Table 1.
Survey Respondent Characteristics.
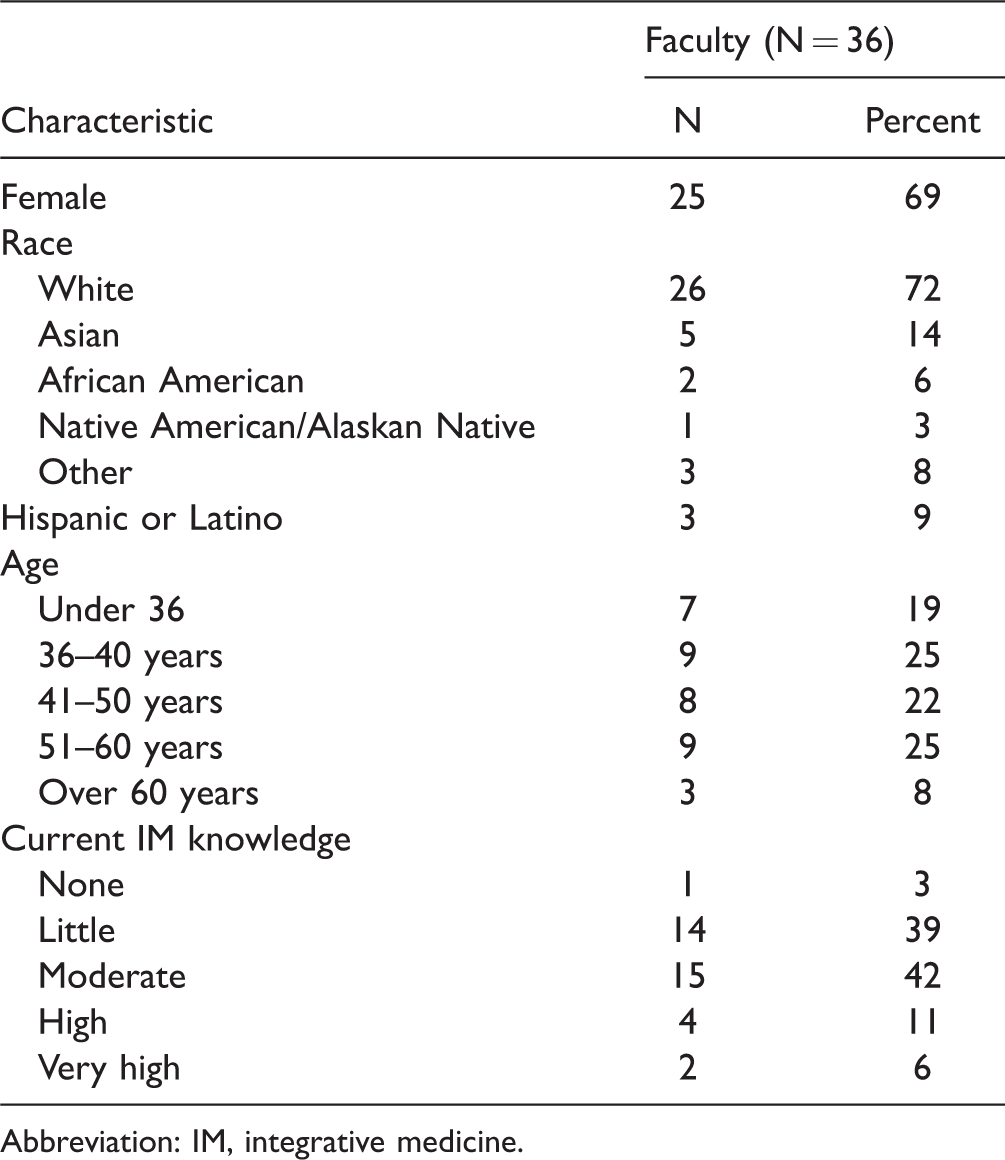
Abbreviation: IM, integrative medicine.
Psychiatry Faculty Characteristics
Of the 36 who completed the survey, about a third identified as program directors (n = 11; 31%). Training programs offered at the sites included general psychiatry residency (n = 30; 83%), child and adolescent fellowship (n = 23; 64%), geriatrics fellowship (n = 9; 25%), addiction fellowship (n = 8; 22%), psychosomatic fellowship (n = 7; 19%), forensic fellowship (n = 3; 8%), and other training programs (n = 2; 6%). The percentage of women responding was high at 69%, and the majority were white (72%).
IM Content Areas
Mean importance ratings of IM content areas are presented in Table 2. The majority of content areas were rated highly. Sleep health was the topic rated as highest importance by faculty in terms of resident/fellow exposure; this was followed by motivational interviewing, self-care, and stress-management. Additional content areas mentioned by faculty included yoga, tai chi, qi gong, and indigenous healing practices. Faculty mean rating of confidence in being able to answer trainee questions on IM topics was fairly low (on a scale from 1 [low] to 5 [high], the mean was 2.86; standard deviation [SD] = 1.1), with only 12 (33%) feeling confident (n = 10; 28%) or very confident (n = 2; 6.5%). Faculty confidence in their trainees’ ability to answer patient questions about IM was even lower (mean = 2.36; SD = 1.0), with only 4 (11%) feeling confident in trainees’ ability. No faculty respondent endorsed feeling “very confident” for this item.
Faculty Psychiatrists IM Content Area Importance Rating—Means in Order of Highest Rating.

Abbreviation: CAM, complementary and alternative medicine.
Medical Conditions
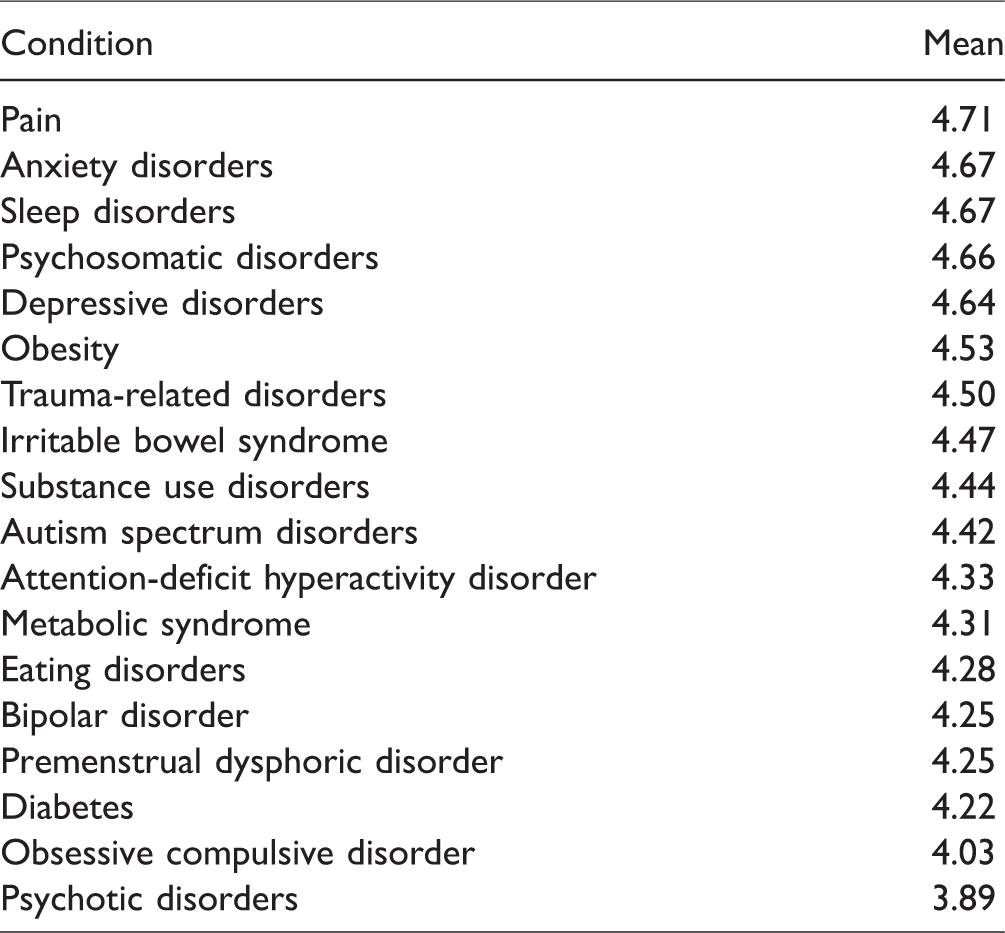
Ratings of the importance of learning an IM approach to specific medical conditions were high. Pain received the highest rating, while psychotic disorders received the lowest rating (see Table 3).
Medical Conditions—Importance of Learning an IM Approach—Means in Order of Highest Rating.
Existing IM Content/Expertise
Half of the faculty reported having existing IM content in their curriculum (n = 18; 50%). However, only 2 of those whose curricula had IM content felt it was sufficient (11%); half were unsure whether it was sufficient (n = 9; 53%) and one-third felt it was not sufficient (n = 6; 36%). Of those with IM content in their curriculum, almost half (n = 8; 44%) offered an IM course/elective; 4 offered 1 to 3 lectures per year (22%); 4 offered more than 3 lectures per year (22%); and 2 (11%) reported incorporating IM content throughout the curriculum. Forty-four percent (n = 16) of programs had a psychiatrist on faculty with some level of training in IM, and 72% (n = 26) had a psychiatrist on faculty with an interest in IM.
Importance, Interest, and Strategies for Incorporating IM Content Into Training Programs
Faculty rated the importance of teaching IM highly (mean = 4.4; SD = 0.9). Interest in incorporating IM content into their training programs was rated just as high (mean = 4.4; SD = 0.8) with 86% of respondents endorsing the top 2 categories for both importance and interest. The most commonly mentioned methods for implementing an IM curriculum were either to incorporate into general training (n = 17; 47%) or offer an elective track (n = 16; 44%). Nineteen respondents (53%) indicated interest in piloting an IM curriculum in their training program. Experiential onsite activities demonstrating IM topics (67%) and online modules supplemented by local faculty (58%) were the 2 most desirable learning formats.
Perceived barriers to incorporating IM content into the training programs are presented in Table 4. The top 3 implementation barriers were time constraints, lack of faculty expertise in IM, and no requirement of IM competencies. The lowest rated barriers were negative attitudes toward IM, resident interest, and administrative support. Similar to the perceived barriers, most comments mentioned time constraints (n = 15), for example, “finding time in the curriculum,” “time constraints given required educational experiences and balance with clinical responsibilities,” and “time constraints—adding to existing curriculum will mean adding lecture hours, unless this is elective and online.” In contrast to the barrier ratings, when asked about the 3 biggest challenges for integrating IM in their program, faculty listed lack of support as second (n = 10), for example, “having all the faculty on board with the idea to have this program,” “turf competition,” and “ensuring that institutional culture is aligned with this broader perspective on mental health and illness.” Other challenges mentioned included lack of faculty training (n = 9), lack of evidence (n = 9), lack of interest (n = 7), fit in curriculum (n = 5), funding (n = 4), not required content (n = 2), lack of knowledge of IM benefits (n = 2), IM practices not reimbursable (n = 1), too diverse a topic (n = 1), and that it is already “comparable to biopsychosocial model of practice” (n = 1). Eighty-one percent of respondents (n = 29) indicated that they would need faculty education and training in IM in order to implement an IM curriculum in their training program.
Barriers to Incorporating IM Content Into Training Program.

Abbreviation: IM, integrative medicine.
Wellness Programs
Many respondents indicated that their site had a program to promote resident/fellow self-care and wellness (n = 25; 69%). Of the 25 sites with wellness programs, the most frequently offered modes were retreats, individual counseling, support groups, and healthy food options (Table 5). Very few faculty rated their wellness program as adequate in addressing resident burnout, with only 4 (13%) endorsing the top 2 response categories.
Wellness Activities Offered at the Training Programs (N = 25).

Discussion
Scientific literature on efficacy and safety of IM approaches in mental health is expanding rapidly; yet it generally takes years for most new scientific discoveries to find their way to standardized medical practice. 14 This suggests that acceptance of IM approaches by clinicians may be slow to catch on, even though evidence is mounting for many modalities. Proper training and awareness of patient use trends enhances clinicians’ ability to educate their patients and to avoid potentially dangerous, non-evidence-based practices; this has led the Academy of Medicine to endorse incorporation of IM into medical profession training, thus forwarding the general goal of creating more comprehensive, patient-centered treatment plans rooted in the biopsychosocialspiritual model. IM training works to improve knowledge of potential risks and benefits of various IM modalities, ultimately providing patients with both better care and greater choice in their care. As the field of psychiatry aims toward a more patient-centered approach to care that concurrently emphasizes provider wellness and resilience, supplementing psychiatry residency training with an IM curriculum has great promise. 15
We acknowledge that there are limitations to this study. The sample size is relatively small. As is true with most voluntary surveys, this needs assessment may have a skewed response rate. Psychiatrists with a prior interest in IM may have been more likely to respond to the survey. Review of institutions expressing interest in the pilot revealed that in some instances multiple individuals from the same institution responded to the survey, further limiting the generalizability of the results. Efforts were made to minimize this bias by reaching out to psychiatrists nationally, by distributing the survey to all ACGME-approved psychiatry residency and fellowship training directors. Although it is true that those who chose to respond were likely more familiar with and favorably predisposed to IM than those who did not respond, the information they submitted could inform future research. An interest in IM among our respondents could suggest greater knowledge of its importance and use, and they may have experience with it themselves. This means that they may have informed opinions to provide, and their answers to our survey may provide insight into the ways that IM will find its way into the psychiatry training curriculum.
An analysis of the characteristics of the respondents and their programs may illuminate factors that contribute to the adoption of IM. Seventy-two percent of our sample were white, which is comparable to the national racial makeup of psychiatry faculty (69%). 16 It is worth noting that the response rate was highly skewed toward women. A total of 69% of our respondents were women, when women make up only 51.4% of psychiatric faculty in the United States. Women constitute only 31.5% of full professors in psychiatry, 45% of associate professors, and 57.6% of assistant professors.16,17 It is also notable that women in general are more likely than men to use CAM 18 and tend to regard it more favorably.
Respondents to the survey were asked whether they might be interested in delving more deeply into IM by participating in a pilot program. Nineteen individuals from 11 programs indicated interest in the pilot, and they represent a diversity of institutions. Six of the individuals who expressed an interest in the pilot were from 3 elite, top-ranked programs in big cities or densely populated areas of the country. Several faculty who responded with interest in participating in a pilot are in programs located in remote or sparsely populated areas. At least 4 of these programs are described as serving native populations, and those programs include approaches drawn from native traditions in treatment. Other programs expressing interest in the pilot serve Latinos, underprivileged populations, diverse communities, and veterans and, like those serving native populations, stress connections to the community.
Given the diversity of institutional types who were willing to take part in a pilot, and despite the fact that our sample was small, responses regarding the way in which IM implementation should happen can be considered instructive. Consistent with prior IMR and IMR-Pediatrics program evaluations, our results suggest that a combination of an interactive online curriculum, onsite activities, and faculty development are essential ingredients for the implementation of an IM curriculum in psychiatry training. The respondents indicated that a few psychiatry training programs already include IM content in their curriculum. The IM content in these programs is generally not comprehensive nor standardized and is based on individual initiatives of psychiatry faculty who have had IM training. The content includes a variety of lectures, handouts, retreats, and/or scholarly discussions. Our respondents largely viewed the content as being inadequate to meet the needs of their trainees and patients, which is unsurprising given the very small amount of time that is currently devoted to covering the vast topic of IM. In addition, only a minority of psychiatrists at training programs rated their own knowledge of IM highly or believed that they had either a moderate or extensive amount of formal training in IM. Even if there were an IM curriculum for residents, the faculty would still need training to be able to guide the residents.
IM in psychiatry is new, so it requires significant work to develop an adequate curriculum. Most programs that have some IM content only include a few hours, without a lot of structure, emphasis, or support from their department chairs. For instance, at one of the institutions represented by our respondents, IM is addressed in an elective course that consists of eight 2-hour lectures. One of these lectures covers acupuncture, Tai Chi, Qi Gong, and homeopathy, among other topics, and another is on nutritional medicine. The time allotted is not sufficient to gain an adequate understanding of the modality; thus, even though they receive some attention, the training can only be at a surface level. The IM field is so vast that until an organized, standardized curriculum is created and piloted and made available, scattered attempts at IM incorporation in various institutions are likely to feel inadequate and superficial.
The integration of IM into training could also help to address the problem of burnout among residents and promote well-being in health-care providers as well as in patients, “caring for the caregiver.” A large part of IM includes mind–body medicine techniques to help in stress management and self-care. Residents who first learn and practice these approaches themselves are in turn more apt to disseminate such tools to their patients. Mind–body techniques used by trainees have been demonstrated to decrease burnout.
19
The ACGME emphasizes the importance of training in physician well-being during residency. In response to high levels of documented burnout of trainees,20,21 the ACGME has incorporated physician well-being as a Common Program Requirement. The ACGME states Programs and Sponsoring Institutions have the same responsibility to address well-being as they do to ensure other aspects of resident competence. Further, self-care is also an important aspect of professionalism, and a skill that must be learned and nurtured in the context of other aspects of graduate medical education.
Our results demonstrate the ways in which our sample faculty of psychiatry training programs would like to see IM incorporated into curricula to provide trainees with an exposure to IM. Although our sample was limited, our respondents were likely more familiar with IM than the general psychiatry faculty, and this means that they can provide input on incorporating IM into training in a more informed manner. The majority of IM content areas for inclusion into a curriculum were rated highly. This assessment supports the perceived importance, by faculty, of trainees learning an integrative approach across diagnostic categories. Learning an integrative approach transcends diagnostic categories as improvement in areas such as nutrition, mindfulness, and sleep will improve a variety of disorders.
The results of this needs assessment pave the way for bringing together a cohort of interested psychiatry training program directors and faculty to develop a psychiatry-specific, interactive, online IMR curriculum that can be piloted across multiple sites. The University of Arizona Department of Psychiatry is currently piloting an IM elective for psychiatry residents and fellows, with promising preliminary data. The elective is being replicated at the University of New Mexico, and the addition of further sites is in progress. Experiences gained from IMR and IMR-Pediatrics, this needs assessment, and the current pilot program will be instrumental in developing a curriculum that can be distributed, implemented, and eventually evaluated across psychiatry training programs. We envision that a well-designed and collaboratively implemented IM curriculum can enhance the prevention and treatment of psychiatric disorders. It will address a need that our assessment indicates is currently unmet, contribute to caregiver wellness, and support patients in seeking a range of options for their mental health care.
Footnotes
Acknowledgments
The authors would like to thank the following people for their contributions: Paula Cook, Research Specialist Senior; Rhonda Hallquist, Instructional Web Developer; Karen Spear Ellinwood, PhD, JD, EdS; Kathy Smith, MD; Ole Thienhaus, MD, FACPsych; and Karen Alexander, PhD, who provided writing assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Weil Foundation awarded to the first author. The views expressed in this article are those of the authors and do not necessarily reflect the position of the Weil Foundation or the University of Arizona. Funding for writing assistance was provided by professional development funds from the University of Arizona.